Advances in the diagnosis and management of gastroesophageal reflux disease
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
STATE OF THE ART REVIEW
Advances in the diagnosis and management of
BMJ: first published as 10.1136/bmj.m3786 on 23 November 2020. Downloaded from http://www.bmj.com/ on 7 January 2021 by guest. Protected by copyright.
gastroesophageal reflux disease
David A Katzka,1 Peter J Kahrilas2
A BST RAC T
1
Gastroesophageal reflux disease (GERD) is a multifaceted disorder encompassing
Mayo Clinic, Division of
Gastroenterology and a family of syndromes attributable to, or exacerbated by, gastroesophageal
Hepatology, Rochester, MN,
USA
reflux that impart morbidity, mainly through troublesome symptoms. Major GERD
2
Northwestern University, phenotypes are non-erosive reflux disease, GERD hypersensitivity, low or high
Feinberg School of Medicine,
Department of Medicine, grade esophagitis, Barrett’s esophagus, reflux chest pain, laryngopharyngeal
Chicago, IL USA
reflux, and regurgitation dominant reflux. GERD is common throughout the world,
Correspondence to: PJ Kahrilas
p-kahrilas@northwestern.edu and its epidemiology is linked to the Western lifestyle, obesity, and the demise of
Cite this as: BMJ 2020;371:m3786
http://dx.doi.org/10.1136/bmj.m3786
Helicobacter pylori. Because of its prevalence and chronicity, GERD is a substantial
Series explanation: State of the
economic burden measured in physician visits, diagnostics, cancer surveillance
Art Reviews are commissioned
on the basis of their relevance
protocols, and therapeutics. An individual with typical symptoms has a fivefold risk
to academics and specialists of developing esophageal adenocarcinoma, but mortality from GERD is otherwise
in the US and internationally.
For this reason they are written rare. The principles of management are to provide symptomatic relief and to
predominantly by US authors.
minimize potential health risks through some combination of lifestyle modifications,
diagnostic testing, pharmaceuticals (mainly to suppress or counteract gastric acid
secretion), and surgery. However, it is usually a chronic recurring condition and
management needs to be personalized to each case. While escalating proton pump
inhibitor therapy may be pertinent to healing high grade esophagitis, its applicability
to other GERD phenotypes wherein the modulating effects of anxiety, motility,
hypersensitivity, and non-esophageal factors may dominate is highly questionable.
Introduction symptomatically, endoscopically, or by physiological
Gastroesophageal reflux disease (GERD) has been testing, which impart morbidity through troublesome
defined from varied perspectives. According to the symptoms and/or risk.
Montreal definition,1 “GERD is a condition which Being a common disease with diverse
develops when the reflux of stomach contents causes manifestations, GERD is managed by many clinicians
troublesome symptoms and/or complications.” The across many specialties: general practitioners,
elegance of this definition is in its simplicity, uniting internists, gastroenterologists, surgeons,
a large, seemingly unrelated set of symptoms and emergency department physicians, hospitalists,
potential complications. However, the Montreal otolaryngologists, pulmonologists, obstetricians,
definition does not consider cofactors that interact and pediatricians. This has spawned a variety of
with reflux, leading to atypical phenotypes captured perspectives. Several management topics—including
under that umbrella. The Lyon Consensus definition2 the usage and safety of proton pump inhibitors
is physiomorphologic, defining GERD by the presence (PPIs), the indications for endoscopy, recommended
of excess gastroesophageal reflux, esophageal motor dietary interventions, and the roles of surgical and
perturbations, and increased epithelial permeability endoscopic interventions—have evolved in recent
that can be associated with reflux. However, most of years, resulting in a somewhat overwhelming volume
these features are non-specific for GERD. The Rome of publications. This narrative review is intended to
IV Conference definition3 is symptom based, focused simplify this often contradictory literature on GERD
on defining functional syndromes with GERD in the adult population for clinicians, academicians,
characteristics. However, functional syndromes can and clinical researchers.
mimic GERD without reflux causality. Merging these
documents is challenging. In this review, GERD is Sources and selection criteria
defined as a family of syndromes attributable to, or We searched PubMed, Medline, and the Cochrane
exacerbated by, gastroesophageal reflux, evident databases from 2010 to May of 2020 using the search
the bmj | BMJ 2020;371:m3786 | doi: 10.1136/bmj.m3786 1STATE OF THE ART REVIEW
Pathogenesis
ABBREVIATIONS
BMJ: first published as 10.1136/bmj.m3786 on 23 November 2020. Downloaded from http://www.bmj.com/ on 7 January 2021 by guest. Protected by copyright.
Obesity and the Western lifestyle
EAC: esophageal adenocarcinoma; EGJ: Several studies have shown a correlation between
esophagogastric junction; GERD: gastroesophageal obesity and GERD and a stronger correlation between
reflux disease; H2RA: histamine-2 receptor antagonist; central adiposity and GERD complications including
LES: lower esophageal sphincter; MSA: magnetic EAC.13 A meta-analysis of 107 international studies
sphincter augmentation; NERD: non-erosive reflux demonstrated a 1.73 relative risk of at least weekly
disease; PCAB: potassium competitive acid blocker; GERD symptoms in obese patients, albeit in a pooled
PPIs: proton pump inhibitors; TIF: transoral incisionless analysis with a large amount of heterogeneity among
fundoplication studies.5 In a separate meta-analysis of 40 studies,
patients with central adiposity had a 1.87 relative
terms gastroesophageal reflux, gastroesophageal risk of erosive esophagitis (95% confidence interval,
reflux disease, esophagitis, Barrett’s esophagus, 1.51 to 2.31) and a 1.98-fold risk of Barrett’s
esophageal hypersensitivity, hypersensitive esophagus that persisted after adjusting for body
esophagus, non-erosive gastroesophageal reflux, mass index.13 Mechanistically, central adiposity
and functional heartburn. Sifting through the results, leads to increased intra-abdominal and intragastric
we prioritized studies by design, likely interest to the pressure challenging the anti-reflux barrier and
readership, and publication date, and we included promoting the development of hiatus hernia. Obesity
older studies of continued relevance. Our initial is also associated with overeating, causing gastric
search returned more than 13 000 unique citations distension and eliciting transient lower esophageal
making it especially difficult to limit this narrative sphincter (LES) relaxations.14 Metabolic sequelae of
review. No patient input was solicited. central obesity may also play a role: even without
pathologic reflux, the distal esophageal epithelium
Prevalence and geographic distribution of obese patients exhibits increased permeability,
GERD is a worldwide disease with reported prevalence indicative of a perturbed epithelial barrier.15
values ranging from 2.5% in China to 51.2% in
Greece.4 5 This range is likely reflective of both true Helicobacter pylori
differences and methodological factors, with some Although discovered relatively recently, H pylori is
surveys equating GERD with weekly heartburn known to have infected humans for at least 50 000
and/or regurgitation and others stipulating erosive years.16 Its strongest disease associations are in
esophagitis. Interestingly, although the prevalence promoting peptic ulcers and gastric cancer. However,
of GERD symptoms is similar among racial groups,6 the infection may also provide protective effects with
complications of GERD such as erosive esophagitis respect to GERD. Epidemiologic data demonstrate
and esophageal adenocarcinoma (EAC) are more that erosive esophagitis, Barrett’s esophagus, and
common in white people, particularly with central EAC are inversely related to H pylori infection.17 18
obesity. Reflux is also increasingly common in young The proposed protective mechanism is that chronic H
adults with the greatest increase seen in people aged pylori gastritis leads to atrophic gastritis and relative
30-39 7 and EAC increasing in patients under 50.8 hypochlorhydria, which in turn diminishes the
acidity of gastroesophageal reflux. Supporting this
Morbidity and mortality concept, PPIs are more effective in the presence of H
Although GERD itself is not a fatal condition, pylori,19 owing to the already diminished gastric acid
potentially morbid complications include EAC, secretion. However, two large randomized controlled
bleeding, esophageal rupture, aspiration, lung trials of H pylori eradication versus placebo did not
transplant rejection, aspiration pneumonia, and show an increase in reflux symptoms two years after
iatrogenic causes including surgery and dilations. eradication,20 21 leaving open the possibility that
The Canadian annual death rate directly related to the observed inverse association between H pylori
GERD was estimated as 65 patients.9 In a Swedish infection and GERD is not a causal one.
population study, the annual death rate was
0.20/100 000 caused by hemorrhagic esophagitis Physiology: the Lyon Consensus
(51.9%), aspiration pneumonia (34.6%), perforated The Lyon Consensus analyzed the role of physiological
esophageal ulcer (9.6%), and spontaneous testing in GERD diagnosis.2 This consensus agreed
esophageal rupture (3.9%).10 that the cornerstone of GERD pathophysiology is
On the other hand, the societal cost of GERD incompetence of the esophagogastric junction (EGJ)
is substantial. In 2004-05, the annual direct evident both by separation between the crural
cost for GERD care in Canada was C$52 235 910 diaphragm and LES as occurs with hiatus hernia,22
(£30.2 million , €33.4 million).9 In the US, GERD and a low EGJ contractile index, an integral of
accounted for 8 863 568 physician visits, 65 634 sphincter pressure over time derived from high
hospitalizations, and an estimated $12.3 billion resolution manometry.23 Whereas historically,
spent on upper endoscopies in a year.11 In Japan, the investigators have focused solely on low LES pressure
mean medical cost for GERD patients aged 20-59 was as indicative of an impaired reflux barrier, the EGJ
$266 per patient per month in 2014, about 2.4 times contractile index broadens the concept to include
the mean national healthcare cost.12 both the crural diaphragm and the LES. A low EGJ
2 doi: 10.1136/bmj.m3786 | BMJ 2020;371:m3786 | the bmjSTATE OF THE ART REVIEW
contractile index is common with erosive esophagitis in high grade esophagitis patients, first healed
BMJ: first published as 10.1136/bmj.m3786 on 23 November 2020. Downloaded from http://www.bmj.com/ on 7 January 2021 by guest. Protected by copyright.
and Barrett’s esophagus. with PPIs, and then observed to develop recurrent
Many GERD patients have an EGJ contractility esophagitis with cessation of PPI therapy.31 These
index within the normal range yet still exhibit findings suggest that alternative pharmacologic
excessive acid reflux by the mechanism of transient approaches independent of acid suppression may be
LES relaxation,24 the physiologic mechanism of feasible to treat esophagitis.
belching. Transient LES relaxations occur through
a vago-vagal reflex triggered by distension of the Diagnostic testing: endoscopy, reflux monitoring,
proximal stomach.25 What appears to differentiate motility testing
GERD patients from normal controls is the frequency Endoscopy is the primary test for suspected GERD
with which transient LES relaxations are associated syndromes because of its availability, relative
with acid (liquid) reflux as opposed to only venting safety, biopsy capability, therapeutic potential,
gas.24 Mechanistically, this is facilitated by increased and specificity of potential findings. Using the
compliance of the EGJ, leading to wider opening (and Los Angeles Classification, four severity grades of
larger volumes of reflux) during relaxation.26 esophagitis (A-D) are defined, based on the extent of
erosions (mucosal breaks) in the distal esophagus.
Hiatus hernia: the co-conspirator The Lyon Consensus considered only Los Angeles C
Axial or sliding hiatal hernia is strongly associated and D esophagitis to be hard evidence of GERD, but
with GERD, particularly with peptic esophagitis and we extend that to include Los Angeles B esophagitis
its complications, to the point that some patients with the caveat that it must be accurately graded. Los
and physicians view hiatal hernia and GERD as Angeles A esophagitis, on the other hand, is found in
being synonymous. While that is clearly erroneous, 5-7% of normal individuals and is not hard evidence
the contribution of a hiatal hernia to GERD of GERD.32 33 Other potentially relevant findings are
pathophysiology is profound and multifaceted. peptic strictures, Barrett’s metaplasia, and hiatus
The most obvious effect is of separating the two hernia.
functional components of the EGJ, the LES and the Prolonged ambulatory esophageal reflux
crural diaphragm, thereby diminishing their ability monitoring (pH or combined pH impedance) has three
to work in concert as a barrier to reflux events and potential uses in managing GERD: 1) quantifying
in promoting esophageal acid clearance following abnormal esophageal acid exposure in the absence of
reflux. Another mechanistic role of hiatal hernia in esophagitis; 2) determining if a patient’s symptoms
GERD has been proposed: the repositioning of the correlate with reflux events; and 3) determining if
acid pocket.27 The acid pocket forms postprandially gastroesophageal reflux (acid or weakly acidic in
as newly secreted acid layers on top of ingested the case of pH impedance studies) is controlled by
food, becoming the reservoir for postprandial reflux. therapy. This becomes relevant in evaluating atypical
With a hiatal hernia, the acid pocket migrates into symptoms or refractory symptoms despite ostensibly
the hernia compartment and facilitates exposure adequate pharmacologic and/or surgical therapy.
of the distal esophageal epithelium to gastric Verifying physiologically defined disease is also
acid during any period of LES relaxation, even essential when considering procedural therapies for
that associated with swallowing or secondary GERD.
peristalsis.28 A postulated mechanism of action of High resolution manometry can detect
alginate compounds in treating GERD is of capping physiological abnormalities associated with
the acid pocket with a protective gelatinous raft GERD such as a low EGJ contractility index, hiatus
and displacing it away from the LES.29 The Lyon hernia, or weak/absent peristalsis, but is not useful
Consensus endorsed the significance of hiatal hernia in defining treatment. The exception is when
in GERD pathophysiology, particularly when >3 cm procedural treatments are contemplated, in which
in size. case manometry is mandated to detect unsuspected
achalasia and to ascertain that peristaltic function
The inflammation hypothesis is sufficiently preserved for the contemplated
The conventional model of reflux esophagitis has intervention.34 35
been the “burn hypothesis” proposing that the
caustic effects of hydrochloric acid combined with GERD phenotypes
enzymatic digestion by pepsin erodes the esophageal Implicit in the Montreal definition is that GERD
epithelium from the lumen inward. However, recent can be defined either by endoscopic features or by
experiments have challenged this concept, instead a symptom complex caused by gastroesophageal
proposing that much of the injury is chronic and reflux. This creates management challenges because
chemokine mediated.30 In rats, acutely induced the determinants of mucosal injury differ from
reflux esophagitis was associated with lymphocyte the determinants of symptoms and it would be
infiltration, initially at the submucosa, progressing to unreasonable to think that treatment strategies should
the epithelial surface. The lymphocytic inflammation not differ as well. The evolving concept is that rather
was associated with secretion of IL-8 and IL-1β than being a continuum of disease with esophagitis
and an injury pattern that persisted for weeks. An simply exemplifying more severe non-erosive reflux
analogous process was subsequently demonstrated disease (NERD), GERD has distinct phenotypes, each
the bmj | BMJ 2020;371:m3786 | doi: 10.1136/bmj.m3786 3STATE OF THE ART REVIEW
with unique and shared features.36Table 1 itemizes that has much better survival or, more commonly,
BMJ: first published as 10.1136/bmj.m3786 on 23 November 2020. Downloaded from http://www.bmj.com/ on 7 January 2021 by guest. Protected by copyright.
the major GERD phenotypes along with important the precursor lesion, Barrett’s metaplasia. Hence,
distinguishing features. societal guidelines (with considerable variability,
Supporting the concept of GERD as a family table 239-44) have proposed using symptom burden
of phenotypes are 20 year longitudinal data as criteria for endoscopic screening and subsequent
showing that progression from NERD to high grade surveillance of Barrett’s esophagus.38 45 Although
esophagitis, stricture, or Barrett’s esophagus is controversial, a systematic analysis of retrospective
uncommon. Additionally, patients with severe case-control studies suggested that such Barrett’s
esophagitis or Barrett’s esophagus have important surveillance programs lead to earlier EAC diagnosis
predispositions, typically being white, male, having and improved mortality.46 Up to 40% of EAC patients
central obesity, and family history. This is in contrast present without a preceding history of significant
to NERD where there is neither racial nor gender reflux symptoms, however.47 Furthermore, 80%-
predilection. The degree to which esophageal 95% of EAC patients present de novo.48 49 In other
hypersensitivity plays into pathophysiology also words, only a small minority of EAC patients have
varies widely among phenotypes. The Rome IV a symptom burden of sufficient severity to warrant
classification conceptualized this within the NERD endoscopic screening for a Barrett’s surveillance
population by subdividing it into “true NERD,” reflux program.
hypersensitivity, and functional heartburn with reflux
as the dominant symptom determinant at one end Atypical and extraesophageal manifestations
and hypersensitivity as the dominant determinant at Reflux has been implicated in causing myriad
the other end (functional heartburn).37 In summary, atypical and extraesophageal syndromes—
although gastroesophageal reflux is a contributing laryngitis, pharyngitis, chronic cough, postnasal
element to all of these syndromes (with the possible drip, non-cardiac chest pain, bronchiectasis, poorly
exception of functional heartburn), its dominance as controlled asthma, globus, cardiac arrhythmias,
a pathophysiological determinant ranges widely. laryngeal cancer, subglottic stenosis, vocal fold
granulomata, halitosis, dental erosions, hiccups,
Barrett’s esophagus and esophageal aspiration pneumonia, pulmonary fibrosis, lung
adenocarcinoma transplant rejection, sleep apnea, burning tongue,
The most severe potential consequence of GERD is dysgeusia, and chronic sinusitis—with the strength
EAC, a cancer whose incidence has risen precipitously of supportive evidence for each entity ranging from
in the West for the past three decades, paralleling sheer conjecture to supportive treatment trials.50
that of GERD. A now classic epidemiological study Reliable attribution of these syndromes to GERD
links these trends, and shows a dose dependent is confounded by proposed pathogenesis models
relation such that patients with severe reflux distinct from those of esophageal syndromes,
symptoms (>3 times per week for >5 years) have a 16- promoting the hypothesis that physiologic (or
fold increased risk of EAC.38 Furthermore, most EAC “silent”) reflux may be injurious. Symptoms such
presents at an advanced stage with poor prognosis as cough or arrhythmias may result from shared
and poor 5 year survival. This led to screening neural pathways stimulated by reflux, but not to the
endoscopy protocols to detect either early EAC threshold required to elicit esophageal symptoms. It
Table 1 | Major GERD phenotypes with key distinguishing features
GERD syndrome Distinguishing features
Non-erosive reflux disease (NERD) • Heterogeneous population
➢ When defined by pH-metry, very similar to low grade esophagitis, but when defined by symptoms, overlaps with GERD
hypersensitivity and functional heartburn
Reflux hypersensitivity • Esophageal hypersensitivity
Functional heartburn ➢ Conceptually differentiated by pH-metry or pH impedance findings, but in practice, these entities can be clinically indistinguishable
Low grade erosive esophagitis • Poor EGJ barrier function with excess acid reflux and typical reflux symptoms (heartburn and regurgitation)
(Los Angeles grade A or B) ➢ LA A esophagitis found in about 6% of asymptomatic controls making it a non-specific finding
High grade erosive esophagitis, • Prolonged esophageal acid clearance with grossly abnormal EGJ function and prominent recumbent (nocturnal) reflux
(LA grade C or D) ➢ Usually associated with hiatus hernia and impaired esophageal motility
Barrett’s esophagus • Greatest risk for esophageal adenocarcinoma
➢ Endoscopic spectrum from intestinal metaplasia at the EGJ to short segment Barrett’s to long segment Barrett’s (>3 cm)
➢ Biological spectrum from non-dysplastic metaplasia to low grade dysplasia to high grade dysplasia
➢ Indicative of both acid and bile reflux
➢ Independent risk factors: central obesity, male gender, white ethnicity, smoking, genetics
Reflux chest pain syndrome • Chest pain that can be indistinguishable from angina
➢ Reflux is the most common cause of esophageal chest pain
➢ Much more amenable to GERD therapy when associated with +pH-metry, esophagitis, or typical reflux symptoms
➢ Partial rather than complete symptom resolution with treatment is common
Regurgitation dominant • Grossly incompetent EGJ barrier with frequent large volume reflux often elicited by postural changes or abdominal straining
reflux disease ➢ Much less responsive than heartburn to medical therapy
➢ Need to differentiate from rumination and achalasia
Laryngopharyngeal reflux (LPR) • Usually multifactorial with dominant non-esophageal cofactors exacerbated by reflux
Chronic cough ➢ Strongly driven by neuronal hypersensitivity
➢ More amenable to GERD therapy when associated with abnormal pH-metry, esophagitis, or typical reflux symptoms
4 doi: 10.1136/bmj.m3786 | BMJ 2020;371:m3786 | the bmjSTATE OF THE ART REVIEW
Table 2 | Societal guidelines for Barrett’s/EAC screening and surveillance endoscopy
BMJ: first published as 10.1136/bmj.m3786 on 23 November 2020. Downloaded from http://www.bmj.com/ on 7 January 2021 by guest. Protected by copyright.
Society Screening endoscopy recommendations Surveillance endoscopy recommendations
BSG39 • Not feasible or justified for an unselected population with reflux symptoms • Suspected Barrett’s 5 years) and/or frequent reflux symptoms and • Barrett’s with no dysplasia, 3-5 years
2015 ≥2 risk factors (age >50 years, white, central obesity, smoking, first degree • After initial examination, no repeat endoscopy in 1 year
relative with Barrett’s or EAC)
• Not recommended in females
• Consider with multiple risk factors (age >50 years, white, chronic and/or
frequent reflux symptoms, central obesity, smoking, first degree relative with
Barrett’s or EAC).
CCA44 • Consider based on age, sex, reflux history, central adiposity, smoking, and • Barrett’s with intestinal metaplasiaSTATE OF THE ART REVIEW
of lifestyle modifications, diagnostic testing, Antacids, alginates, and surface acting compounds
BMJ: first published as 10.1136/bmj.m3786 on 23 November 2020. Downloaded from http://www.bmj.com/ on 7 January 2021 by guest. Protected by copyright.
pharmaceuticals, and surgery. The decision of Antacids neutralize gastric acid without reducing
whether or not to perform diagnostic testing is acid secretion, thereby briefly relieving GERD
based on the management history, risk assessment, symptoms. However, their efficacy may be
and symptom assessment. Generally speaking, enhanced when combined with alginates, natural
empiric therapy is appropriate for typical GERD polysaccharide polymers that precipitate into a low
symptoms, whereas atypical symptoms, a history of density viscous gel on contact with acid. The acid
failed treatments, or alarm symptoms (dysphagia, also releases CO2 from the bicarbonate. With the CO2
bleeding, vomiting, or unintentional weight loss) trapped in the alginate gel, this mixture floats to the
prompt endoscopic evaluation. The objective of top of the gastric content.64 Newly secreted acid also
endoscopy is both diagnostic and to control the layers on top of an ingested meal forming the “acid
risk of EAC by detecting early cancers or identifying pocket” evident within 20 minutes of eating and
Barrett’s metaplasia as a marker of a high risk group serving as the reservoir for post-cibal acid reflux.65 66
suitable for subsequent endoscopic surveillance. The alginate-antacid gel displaces the acid pocket
Performing endoscopy on patients with typical reflux distally, positioning it away from the EGJ causing
symptoms, but without alarm symptoms, is unlikely the gel to reflux in lieu of acid.67-69 Analogous to
to alter management, however. Illustrative of this this, a hyaluronic acid-chondroitin sulfate based
are data from a US database of 543 103 endoscopies bioadhesive formulation has been developed to
performed from 2003 through 2014 which identified create a barrier on the esophageal mucosa to reduce
73 535 (13.5% of the total) done for uncomplicated contact with refluxate. A randomized, double blind
GERD symptoms.58 Expressed as a percentage of trial of 154 patients with NERD showed that the
positive findings, the yield of these procedures was combination of the mucosal protectant and acid
0.1% for esophageal tumors, 0.1% for gastric tumors, suppression improved symptom relief in NERD
2.8% for esophageal strictures, 2% for high grade patients compared with acid suppression alone
esophagitis, and 1.4% for suspected long segment (53% v 32%, P4 is a
index and frequent reflux symptoms.60 The benefit reliable physiomarker of effectiveness in high grade
of weight loss for controlling GERD symptoms has esophagitis,71 72 with the target being 50-70% of a 24
not been demonstrated in clinical trials, however, hour period.73 This value varies from 35-68% of the
and instead rests on observational epidemiology.61-63 day at 5 day steady state among different PPIs (with
Nonetheless, if weight gain paralleled the substantial inter-individual variability) and is up to
development of reflux symptoms, even without 93% of the day on the first day of administration for
the individual being overweight, it is reasonable to the PCAB, vonoprazan (fig 1). However, translating
propose weight loss as a treatment strategy. the data in figure 1 to the clinical endpoint of healing
6 doi: 10.1136/bmj.m3786 | BMJ 2020;371:m3786 | the bmjSTATE OF THE ART REVIEW
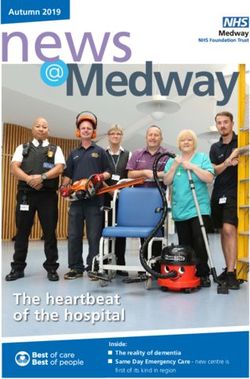
esophagitis is challenging. This is exemplified in of therapy. However, with their widespread long
BMJ: first published as 10.1136/bmj.m3786 on 23 November 2020. Downloaded from http://www.bmj.com/ on 7 January 2021 by guest. Protected by copyright.
figure 2, which illustrates the results of a randomized, term use over the past few decades, the relation
double blind, parallel group, dose ranging study, in between PPIs and a multitude of adverse outcomes
732 subjects comparing vonoprazan with a mid- has been scrutinized, causing a backlash against
potency PPI, lansoprazole 30 mg.74 Although trends PPI use. Adverse consequences are the proposed
toward greater efficacy are evident at the two week result of either profound acid inhibition, secondary
time point for LA C/D esophagitis with the higher hypergastrinemia, or idiosyncratic reactions.
doses of vonoprazan, none of the differences are However, most of this literature stems from
clinically or statistically significant. It should also be observational population based studies and only
emphasized that a drug’s efficacy in healing high grade one relevant randomized controlled trial: a placebo
esophagitis does not necessarily parallel its efficacy controlled, randomized, double blind trial of 17 598
for symptomatic clinical endpoints wherein reflux participants with stable cardiovascular disease
acidity is but one of multiple symptom determinants. randomized to pantoprazole 40 mg daily or placebo
Figure 3 compares the randomized controlled trial as well as one of four anticoagulant regimens.79
data on the efficacy of PPIs for healing esophagitis Prospective data were collected for a median of
with that of resolving key symptomatic endpoints: three years (53 152 patient years of follow-up) on a
resolving heartburn and regurgitation. Not only is variety of adverse outcomes put forth in population
the efficacy substantially lower for the symptomatic based studies as PPI “risks”: pneumonia, Clostridium
endpoints, but within the individual PPI trials that difficile infection, other enteric infections, fractures,
tested multiple doses, no dose-response relation was gastric atrophy, chronic kidney disease, diabetes,
seen for either heartburn or regurgitation relief.75-77 chronic obstructive lung disease, dementia,
Furthermore, a 13% difference in therapeutic gain is cardiovascular disease, cancer, hospitalizations, and
evident for heartburn dependent on whether or not it all cause mortality. The only significant difference
occurs in the context of erosive esophagitis or NERD, found between the pantoprazole and placebo groups
suggesting that its specificity as an acid induced was for enteric infections (1.4% versus 1.0% in the
symptom is less in the absence of esophagitis. placebo group; odds ratio, 1.33). For all other safety
Whatever the presentation of GERD, the likelihood outcomes, proportions were similar between groups
of spontaneous, sustained remission is low and except for C difficile infection, which exhibited a
maintenance therapy is usually required. Although trend to being more common with pantoprazole.
even the most severe esophagitis can be healed Proponents of population based epidemiology
with PPIs, recurrence is in approximately 80% of argue that the 3 year randomized controlled trial was
patients within six months of discontinuation78 and still too small and too short to detect rare long term
the likelihood of recurrence is directly related to the adverse events associated with PPI use. Instead they
initial severity of esophagitis. Symptoms also usually point to the many population based studies and meta-
relapse after PPI discontinuation. Maintenance analyses of PPI risks summarized in table 3.80-101
therapy should be adjusted to the minimal level of acid However, the mechanistic hypotheses that link these
suppression necessary to maintain symptom relief. adverse outcomes to PPI use are without support
Irrespective of instructions, most patients do this on from experimental studies. Population based studies
their own, adopting on-demand or intermittent PPI are subject to unrecognized, uncontrolled bias (for
dosing as required for symptom control.59 instance, frailty), or recognized but inadequately
controlled bias, such that odds ratios of less than
PPI safety 3 in such studies rarely prove to be meaningful.102
For short term use, PPIs have proven quite safe. Applying that filter to the data in table 3 reduces the
Side effects include headache (4 for 50%-70% of the day to facilitate healing of high grade esophagitis
the bmj | BMJ 2020;371:m3786 | doi: 10.1136/bmj.m3786 7STATE OF THE ART REVIEW
LOW GRADE ESOPHAGITIS (Los Angeles A/B) HIGH GRADE ESOPHAGITIS (Los Angeles C/D)
BMJ: first published as 10.1136/bmj.m3786 on 23 November 2020. Downloaded from http://www.bmj.com/ on 7 January 2021 by guest. Protected by copyright.
92% 83%
Lansoprazole 30 mg
97%
N=86 94%
N=46
86% 78%
Vonoprazan 5 mg
98%
N=88 95%
N=55
93% 89%
Vonoprazan 10 mg
96%
N=89 93%
N=44
94% 96%
Vonoprazan 20 mg
93%
N=94 100%
N=50
94% 96%
Vonoprazan 40 mg
95%
N=84 96%
N=50
0% 20% 40% 60% 80% 100% 0% 20% 40% 60% 80% 100%
2 weeks
8 weeks
Fig 2 | Results of a dose ranging randomized controlled trial comparing vonoprazan with lansoprazole for healing low and high grade esophagitis.
Healing was assessed by endoscopy after two weeks and eight weeks of treatment. Although a trend toward faster healing with high grade
esophagitis was evident, none of the differences in healing rates are significant. Data from Ashida, 2015
of which are also supported by either prospectively GABAB agonist inhibits the vagal pathway for transient
collected data in the case of enteric infections or very LES relaxations, but the side effects of somnolence
convincing case reports in the case of acute interstitial and dizziness limit its clinical utility for GERD. Hence,
nephritis. In summary, although observational novel GABAB agonists were developed to avoid these
epidemiological data have prompted great concern, side effects. Lesogaberon was the candidate drug
prospective studies have yet to show any significant that progressed furthest in clinical trials, but phase
risk of chronic PPI use. II clinical trials failed to show clinically significant
additive benefit to PPIs and, with only that modest
Reflux inhibition and prokinetic drugs benefit,103 development was halted. Consequently,
Since transient LES relaxations are a common baclofen remains the only reflux inhibitor currently
mechanism of reflux, their pharmacological inhibition available, albeit without that approved indication
represents an attractive treatment target. Baclofen, a and with very limiting side effects.
83.6%
Esophagitis healing
28.2%
NNT=1.8
56%
Heartburn relief
16%
NNT=2.4
With or without esophagitis
39.7%
Heartburn relief
12.6%
NNT=3.7
Without esophagitis
47%
Regurgitation relief
30%
NNT=5.9
With or without esophagitis
0% 25% 50% 75% 100%
PPI
Placebo
Fig 3 | The diminishing efficacy of PPIs going from healing esophagitis to treatment for cardinal GERD symptoms with
or without coexistent esophagitis. Data are from randomized controlled trials using once daily PPIs. NNT=number
needed to treat to benefit one individual
8 doi: 10.1136/bmj.m3786 | BMJ 2020;371:m3786 | the bmjSTATE OF THE ART REVIEW
Table 3 | Summary of observational epidemiology reports (meta-analyses or population clinical guidelines recommend against its use in
GERD.59
BMJ: first published as 10.1136/bmj.m3786 on 23 November 2020. Downloaded from http://www.bmj.com/ on 7 January 2021 by guest. Protected by copyright.
based studies) of adverse outcomes associated with long term PPI use. For each adverse
outcome, only one report (most recent, largest, or highest quality) is included. Note
that these associations do not prove causation and only the adverse outcome of enteric Visceral hypersensitivity
infections has been supported by randomized controlled trial data (see text) Evident in table 1, several of the major GERD
OR, HR, or 95% Confidence phenotypes have esophageal or visceral
Adverse outcome RR with PPI use interval Patients analyzed
hypersensitivity as a distinguishing feature.
All cause mortality80 1.68 1.53-1.84 20k
Bone related
Antidepressants may modulate esophageal
All fractures81 1.5 1.16-1.45 1.5m sensitivity, potentially benefiting these syndromes.
Dental implant failure82 2.02 1.41-2.88 5k Supportive of this, trazodone, a serotonin antagonist
Hip fracture83 1.2 1.14-1.28 2.1m and reuptake inhibitor, was more effective than
Osteoporosis81 1.23 1.06-1.42 100k placebo in 29 symptomatic patients with motility
Spine fracture81 1.49 1.31.-1.68 700k abnormalities completing a 6 week, double blind,
Wrist fracture83 1.09 0.95-1.20 —
placebo controlled trial.107 Similarly, a selective
Cancer
serotonin reuptake inhibitor, citalopram, reduced
Colorectal cancer84 1.55 0.88-2.73 100k
Gastric cancer85 2.5 1.74-3.85 900k esophageal acid sensitivity, and significantly
Pancreatic cancer84 3.52 0.36-34.49 10k improved symptoms in a 10 patient randomized,
Cardiovascular placebo controlled, crossover, double blind acute
Cardiovascular events86 1.25 1.11-1.42 400k study92 and in a placebo controlled randomized
Infections trial of 252 patients with pH impedance defined
C difficile87 1.99 1.73-2.30 400k hypersensitivity (67% v 23%).108 109 However, in
Recurrent C difficile88 1.73 1.39-2.15 8k
an 83 patient randomized, placebo controlled
Enteric infections89 4.28 3.01-6.08 —
Pneumonia90 1.43 1.30-1.57 7.6m
trial testing the efficacy of a low dose tricyclic
SIBO*91 1.71 1.20-2.43 7k antidepressant (imipramine) for treating esophageal
Kidney related hypersensitivity and functional heartburn, the
Acute interstitial nephritis92 3.76 2.36-5.99 600k response rates (judged by 50% reduction in GERD
Acute kidney injury92 1.61 1.16-2.22 2.4m symptoms) were 37.2% and 37.5% for imipramine
Chronic kidney disease93 1.32 1.19-1.46 800k and placebo respectively, with no observed difference
End stage renal disease94 1.88 1.71-2.07 500k between patients with hypersensitivity and those
Neurological
with functional heartburn.110 Imipramine treatment
Alzheimer’s95 0.96 0.83-1.09 400k
Dementia95 1.23 0.90-1.67 100k
was, however, associated with improved quality of
Miscellaneous life as assessed by SF-36 score, offering some support
Risk of fall96 1.27 1.07-1.50 400k to its use.
Fundic gland polyps97 2.46 1.42-4.27 40k
Gastric mucosal atrophy98 1.55 1.00-2.41 3k Barrett’s esophagus
Hypomagnesemia99 1.44 1.13-1.76 100k Retrospective case-control studies report conflicting
Microscopic colitis100 2.68 1.73-4.17 0.4k
results as to whether or not medical treatment prevents
OR=odds ratio; HR=hazard ratio; RR=risk ratio.
k=103; m=106. progression of Barrett’s epithelium to EAC.111 112
*Small intestinal bacterial overgrowth. The Aspirin and Esomeprazole Chemoprevention
in Barrett’s metaplasia trial (AspECT) was a large
In theory, drugs that augment esophageal randomized controlled trial intended to clarify the
motility or gastric emptying can be beneficial in issue. Some 2557 non-dysplastic Barrett’s patients at
GERD by reducing the occurrence of reflux and/or 84 centers in the UK were randomized to standard or
enhancing the process of esophageal acid clearance. high dose esomeprazole with or without aspirin (four
Prucalopride and mosapride are 5-HT4 agonists groups) and followed for at least eight years. The
commercialized as prokinetics with potentially primary composite endpoint was time to all cause
beneficial physiological effects for GERD when mortality, EAC, or high grade dysplasia. The high
tested in normal volunteers. However, neither dose PPI and aspirin group was significantly more
was shown to be beneficial as add-on therapy to likely to achieve the composite endpoint, but the
PPIs either in a double blind, placebo controlled, effect was driven mainly by improved overall survival
randomized, crossover study of 21 healthy rather than reduced progression of Barrett’s.113
volunteers (prucalopride) or in a randomized trial of Hence, this remains an open question, with experts
116 esophagitis patients (mosapride).104 105 differing on their interpretation of these data.
The prokinetic most widely used for GERD is A major advance in the management of Barrett’s
metoclopramide, an antidopaminergic drug that pertains to patients with high grade dysplasia and
also has 5-HT3 antagonist, 5-HT4 agonist, and early cancers. Whereas these patients would formerly
cholinomimetic properties.106 However, no high be treated with esophagectomy, the current standard
quality data support the use of metoclopramide as of practice is complete endoscopic ablation of the
monotherapy or adjunctive therapy in any GERD Barrett’s segment with endoscopic resection of visible
syndrome. Furthermore, the drug has the potential for lesions followed by high dose acid suppression and,
substantial central nervous system toxicity (tremor, if necessary, fundoplication.114 115 The dominant
Parkinsonism, depression, tardive dyskinesia), and ablation method used is radiofrequency energy as
the bmj | BMJ 2020;371:m3786 | doi: 10.1136/bmj.m3786 9STATE OF THE ART REVIEW
reported in a randomized controlled trial involving fitted around the LES laparoscopically. The beads
BMJ: first published as 10.1136/bmj.m3786 on 23 November 2020. Downloaded from http://www.bmj.com/ on 7 January 2021 by guest. Protected by copyright.
127 patients with dysplastic Barrett’s. In that trial, separate when the LES opens during peristalsis and
the ablation group had better Barrett’s eradication their magnetic attraction then augments sphincter
and developed fewer cancers compared with the closure. In an uncontrolled trial reporting on 100
sham treated group (77.4% v 2.3%, P3 cm hiatal hernia compared TIF and placebo
them to either laparoscopic Nissen fundoplication with sham surgery and 40-80 mg omeprazole.125
or 20-40 mg esomeprazole.116 Estimated remission After six months of treatment, a larger proportion
rates at 5 years, defined as not needing a PPI of TIF patients achieved the primary endpoint of
in the surgical group or adequately controlled elimination of troublesome regurgitation (67% v
symptoms in the PPI group, were 92% with PPIs 45% for PPI, P3 cm hiatal hernias, or morbid
encountered 79% screening failures, 67% of those obesity.
treated improved with fundoplication compared All surgical and procedural trials have specifically
with 28% with active medical management and 12% excluded patients with morbid obesity leaving open
with control medical management (PSTATE OF THE ART REVIEW
through troublesome symptoms and/or injury.
RESEARCH QUESTIONS
BMJ: first published as 10.1136/bmj.m3786 on 23 November 2020. Downloaded from http://www.bmj.com/ on 7 January 2021 by guest. Protected by copyright.
GERD is common throughout the world with its
epidemiology largely linked to the Western lifestyle • How to better define the reflux contribution to myriad
and obesity. Because of its prevalence and chronicity, putative laryngopharyngeal reflux syndromes?
GERD is a huge economic burden. However, apart • How to better identify and treat visceral
from the roughly fivefold risk of developing EAC, hypersensitivity as a determinant of reflux
mortality related to GERD is very rare. The principles syndromes?
of management are both to provide symptomatic • What are effective early detection/prevention
relief and to minimize potential health risks through strategies for esophageal adenocarcinoma?
some combination of lifestyle modifications,
diagnostic testing, pharmaceuticals to suppress
gastric acid secretion, and surgery. However, HOW PATIENTS WERE INVOLVED IN THE CREATION
management needs to be personalized to the specific OF THIS ARTICLE
GERD phenotype recognizing that each has distinct No patients were directly involved in the creation of this
pathophysiological features. Management principles article.
are shown in the summary (box 1).
Contributors: Both authors contributed equally to the conception,
Box 1: Summary of GERD management analysis, interpretation of data, drafting, revising, and final proofing of
the work. PJK is the guarantor of the work.
Diagnosis Funding: PJK was supported by P01 DK092217 (PI: John E
Symptom assessment Pandolfino) from the US Public Health Service.
• With typical heartburn and/or regurgitation, GERD is confirmed by an expected Competing interests: The BMJ has judged that there are no
response to treatment disqualifying financial ties to commercial companies. The authors
declare the following other interests: PJK has advised Ironwood on
Endoscopy drug development for GERD, and Bayer on drug development to treat
• The primary test in the evaluation of suspected GERD syndromes chronic cough, and received grants from the US National Institute
of Health and Ironwood Pharmaceuticals outside the scope of this
○○Alarm symptoms: (dysphagia, bleeding, vomiting, or unintentional weight loss) article. DAK is a member of the governing board for the American
○○Atypical symptoms Gastroenterological Association (no relation to this article), undertook
○○Unsatisfactory response to empiric PPI therapy research (unpaid) for Shire and Celgene, and gave an academic
lecture on eosinophilic esophagitis to Celgene.
○○Barrett’s/EAC risk—regional guidelines vary regarding the specific indications for
screening and surveillance Further details of The BMJ policy on financial interests are here:
https://www.bmj.com/about-bmj/resources-authors/forms-policies-
○○Evaluate for disorders, particularly eosinophilic esophagitis, infectious and-checklists/declaration-competing-interests
esophagitis Provenance and peer review: commissioned; externally peer
Prolonged ambulatory esophageal reflux monitoring reviewed.
• Suspected GERD syndrome without esophagitis (or only Los Angeles grade A)
1 Vakil N, van Zanten SV, Kahrilas P, Dent J, Jones R, Global Consensus
○○Ascertain the presence and severity of physiologically defined GER Group. The Montreal definition and classification of gastroesophageal
○○Determine if symptoms correlate with reflux events reflux disease: a global evidence-based consensus. Am J
○○Determine if gastroesophageal reflux is being controlled by therapy Gastroenterol 2006;101:1900-20, quiz 1943. doi:10.1111/j.1572-
0241.2006.00630.x
High resolution manometry 2 Gyawali CP, Kahrilas PJ, Savarino E, et al. Modern diagnosis of
GERD: the Lyon Consensus. Gut 2018;67:1351-62. doi:10.1136/
• No diagnostic role for GERD gutjnl-2017-314722
• Indicated to exclude alternative diagnoses (eg, achalasia) and to evaluate peristalsis 3 Drossman DA, Hasler WL. Rome IV-functional GI disorders: disorders
when procedural therapies are being considered of gut-brain interaction. Gastroenterology 2016;150:1257-61.
doi:10.1053/j.gastro.2016.03.035
Treatment 4 Richter JE, Rubenstein JH. Presentation and epidemiology of
Lifestyle modifications gastroesophageal reflux disease. Gastroenterology 2018;154:267-
76. doi:10.1053/j.gastro.2017.07.045
• Tailor to the individual patient’s triggers and symptom patterns 5 Eusebi LH, Ratnakumaran R, Yuan Y, Solaymani-Dodaran M, Bazzoli
• Emphasize weight loss if at all relevant to the individual F, Ford AC. Global prevalence of, and risk factors for, gastro-
oesophageal reflux symptoms: a meta-analysis. Gut 2018;67:430-
Antacids, alginates, H2RAs 40. doi:10.1136/gutjnl-2016-313589
• Mild intermittent symptoms: use on demand 6 El-Serag HB, Sweet S, Winchester CC, Dent J. Update on the
epidemiology of gastro-oesophageal reflux disease: a systematic
• Breakthrough symptoms while on maintenance PPI therapy review. Gut 2014;63:871-80. doi:10.1136/gutjnl-2012-304269
PPIs, PCABs 7 Yamasaki T, Hemond C, Eisa M, Ganocy S, Fass R. The changing
epidemiology of gastroesophageal reflux disease: are patients
• Preventive treatment for frequent/severe symptoms, erosive esophagitis, and/or getting younger?J Neurogastroenterol Motil 2018;24:559-69.
stricture doi:10.5056/jnm18140
• Atypical symptoms that respond to empirical 8 week therapeutic trial 8 Sawas T, Manrique GC, Iyer PG, Wang KK, Katzka DA. Young adults
with esophageal adenocarcinoma present with more advanced
• Tailor dosing and patterning of usage to the specific syndrome stage tumors and have shorter survival times. Clin Gastroenterol
Hepatol 2019;17:1756-62. doi:10.1016/j.cgh.2018.09.031
Procedural therapies: Nissen fundoplication is the standard
9 Fedorak RN, Veldhuyzen van Zanten S, Bridges R. Canadian
• Physiological or endoscopic unequivocal GERD with: Digestive Health Foundation Public Impact Series: gastroesophageal
○○PPI intolerance reflux disease in Canada: incidence, prevalence, and direct and
indirect economic impact. Can J Gastroenterol 2010;24:431-4.
○○Regurgitation dominant disease poorly responsive to PPIs doi:10.1155/2010/296584
○○Uncontrolled recumbent reflux 10 Rantanen TK, Salo JA. Gastroesophageal reflux disease as a
○○Chronic recurrent aspiration causing pulmonary injury (bronchiectasis, cause of death: analysis of fatal cases under conservative
treatment. Scand J Gastroenterol 1999;34:229-33.
pneumonia) doi:10.1080/00365529950173609
the bmj | BMJ 2020;371:m3786 | doi: 10.1136/bmj.m3786 11STATE OF THE ART REVIEW
11 Peery AF, Dellon ES, Lund J, et al. Burden of gastrointestinal disease in 31 Dunbar KB, Agoston AT, Odze RD, et al. Association of acute
the United States: 2012 update. Gastroenterology 2012;143:1179- gastroesophageal reflux disease with esophageal histologic changes.
BMJ: first published as 10.1136/bmj.m3786 on 23 November 2020. Downloaded from http://www.bmj.com/ on 7 January 2021 by guest. Protected by copyright.
1187.e3. doi:10.1053/j.gastro.2012.08.002 JAMA 2016;315:2104-12. doi:10.1001/jama.2016.5657
12 Miwa H, Takeshima T, Iwasaki K, Hiroi S. Medical cost, incidence rate, 32 Takashima T, Iwakiri R, Sakata Y, et al. Endoscopic reflux esophagitis
and treatment status of gastroesophageal reflux disease in Japan: and Helicobacter pylori infection in young healthy Japanese
analysis of claims data. J Med Econ 2016;19:1049-55. doi:10.1080/ volunteers. Digestion 2012;86:55-8. doi:10.1159/000338849
13696998.2016.1192551 33 Zagari RM, Fuccio L, Wallander MA, et al. Gastro-oesophageal reflux
13 Singh S, Sharma AN, Murad MH, et al. Central adiposity is associated symptoms, oesophagitis and Barrett’s oesophagus in the general
with increased risk of esophageal inflammation, metaplasia, and population: the Loiano-Monghidoro study. Gut 2008;57:1354-9.
adenocarcinoma: a systematic review and meta-analysis. Clin doi:10.1136/gut.2007.145177
Gastroenterol Hepatol 2013;11:1399-1412.e7. doi:10.1016/j. 34 Pandolfino JE, Kahrilas PJ, American Gastroenterological
cgh.2013.05.009 Association. American Gastroenterological Association
14 Wildi SM, Tutuian R, Castell DO. The influence of rapid food medical position statement: Clinical use of esophageal
intake on postprandial reflux: studies in healthy volunteers. manometry. Gastroenterology 2005;128:207-8. doi:10.1053/j.
Am J Gastroenterol 2004;99:1645-51. doi:10.1111/j.1572- gastro.2004.11.007
0241.2004.30273.x 35 Pandolfino JE, Kahrilas PJ, American Gastroenterological
15 Blevins CH, Dierkhising RA, Geno DM, et al. Obesity and GERD impair Association. AGA technical review on the clinical use of esophageal
esophageal epithelial permeability through 2 distinct mechanisms. manometry. Gastroenterology 2005;128:209-24. doi:10.1053/j.
Neurogastroenterol Motil 2018;30:e13403. doi:10.1111/ gastro.2004.11.008
nmo.13403 36 Katzka DA, Pandolfino JE, Kahrilas PJ. Phenotypes of
16 Atherton JC, Blaser MJ. Coadaptation of Helicobacter pylori gastroesophageal reflux disease: where Rome, Lyon, and Montreal
and humans: ancient history, modern implications. J Clin meet. Clin Gastroenterol Hepatol 2020;18:767-76. doi:10.1016/j.
Invest 2009;119:2475-87. doi:10.1172/JCI38605 cgh.2019.07.015
17 Labenz J, Jaspersen D, Kulig M, et al. Risk factors for erosive 37 Drossman DA. Functional Gastrointestinal Disorders: History,
esophagitis: a multivariate analysis based on the ProGERD study pathophysiology, clinical features and Rome IV. Gastroenterology
initiative. Am J Gastroenterol 2004;99:1652-6. doi:10.1111/j.1572- 2016;150:1262-79. doi:10.1053/j.gastro.2016.02.032
0241.2004.30390.x 38 Lagergren J, Bergström R, Lindgren A, Nyrén O. Symptomatic
18 Wang Z, Shaheen NJ, Whiteman DC, et al. Helicobacter pylori infection gastroesophageal reflux as a risk factor for esophageal
is associated with reduced risk of Barrett’s esophagus: an analysis adenocarcinoma. N Engl J Med 1999;340:825-31. doi:10.1056/
of the Barrett’s and Esophageal Adenocarcinoma Consortium. Am NEJM199903183401101
J Gastroenterol 2018;113:1148-55. doi:10.1038/s41395-018- 39 Fitzgerald RC, di Pietro M, Ragunath K, et al, British Society of
0070-3 Gastroenterology. British Society of Gastroenterology guidelines
19 Kulig M, Leodolter A, Vieth M, et al. Quality of life in relation to on the diagnosis and management of Barrett’s oesophagus.
symptoms in patients with gastro-oesophageal reflux disease-- Gut 2014;63:7-42. doi:10.1136/gutjnl-2013-305372
an analysis based on the ProGERD initiative. Aliment Pharmacol 40 Weusten B, Bisschops R, Coron E, et al. Endoscopic management
Ther 2003;18:767-76. doi:10.1046/j.1365-2036.2003.01770.x of Barrett’s esophagus: European Society of Gastrointestinal
20 Moayyedi P, Feltbower R, Brown J, et al, Leeds HELP Study Group. Endoscopy (ESGE) Position Statement. Endoscopy 2017;49:191-8.
Effect of population screening and treatment for Helicobacter pylori doi:10.1055/s-0042-122140
on dyspepsia and quality of life in the community: a randomised 41 Spechler SJ, Sharma P, Souza RF, Inadomi JM, Shaheen NJ, American
controlled trial. Lancet 2000;355:1665-9. doi:10.1016/S0140- Gastroenterological Association. American Gastroenterological
6736(00)02236-4 Association technical review on the management of Barrett’s
21 Harvey RF, Lane JA, Murray LJ, Harvey IM, Donovan JL, Nair P, esophagus. Gastroenterology 2011;140:e18-52, quiz e13.
Bristol Helicobacter Project. Randomised controlled trial of doi:10.1053/j.gastro.2011.01.031
effects of Helicobacter pylori infection and its eradication 42 Cohen J, Desilets DJ, Hwang JH, et al. Gastrointestinal Endoscopy
on heartburn and gastro-oesophageal reflux: Bristol Editorial Board top 10 topics: advances in GI endoscopy in
helicobacter project. BMJ 2004;328:1417-20. doi:10.1136/ 2018. Gastrointest Endosc 2019;90:35-43. doi:10.1016/j.
bmj.38082.626725.EE gie.2019.03.020
22 Pandolfino JE, Kwiatek MA, Ho K, Scherer JR, Kahrilas PJ. Unique 43 Shaheen NJ, Falk GW, Iyer PG, Gerson LB, American College of
features of esophagogastric junction pressure topography in Gastroenterology. ACG Clinical Guideline: Diagnosis and Management
hiatus hernia patients with dysphagia. Surgery 2010;147:57-64. of Barrett’s Esophagus. Am J Gastroenterol 2016;111:30-50, quiz
doi:10.1016/j.surg.2009.05.011 51. doi:10.1038/ajg.2015.322
23 Kahrilas PJ, Bredenoord AJ, Fox M, et al, International High Resolution 44 Whiteman DC, Appleyard M, Bahin FF, et al. Australian clinical
Manometry Working Group. The Chicago Classification of esophageal practice guidelines for the diagnosis and management of Barrett’s
motility disorders, v3.0. Neurogastroenterol Motil 2015;27:160-74. esophagus and early esophageal adenocarcinoma. J Gastroenterol
doi:10.1111/nmo.12477 Hepatol 2015;30:804-20. doi:10.1111/jgh.12913
24 Pandolfino JE, Zhang QG, Ghosh SK, Han A, Boniquit C, Kahrilas 45 Gaddam S, Maddur H, Wani S, et al. Risk factors for nocturnal
PJ. Transient lower esophageal sphincter relaxations and reflux: reflux in a large GERD cohort. J Clin Gastroenterol 2011;45:764-8.
mechanistic analysis using concurrent fluoroscopy and high- doi:10.1097/MCG.0b013e318205e164
resolution manometry. Gastroenterology 2006;131:1725-33. 46 Codipilly DC, Chandar AK, Singh S, et al. The effect of endoscopic
doi:10.1053/j.gastro.2006.09.009 surveillance in patients with Barrett’s esophagus: a systematic review
25 Liu J, Pehlivanov N, Mittal RK. Baclofen blocks LES relaxation and and meta-analysis. Gastroenterology 2018;154:2068-86 e2065.
crural diaphragm inhibition by esophageal and gastric distension in 47 Sawas T, Killcoyne S, Iyer PG, et al. Identification of prognostic
cats. Am J Physiol Gastrointest Liver Physiol 2002;283:G1276-81. phenotypes of esophageal adenocarcinoma in 2 independent
doi:10.1152/ajpgi.00080.2002 cohorts. Gastroenterology 2018;155:1720-8 e1724.
26 Pandolfino JE, Shi G, Trueworthy B, Kahrilas PJ. Esophagogastric 48 Dulai GS, Guha S, Kahn KL, Gornbein J, Weinstein WM. Preoperative
junction opening during relaxation distinguishes nonhernia prevalence of Barrett’s esophagus in esophageal adenocarcinoma: a
reflux patients, hernia patients, and normal subjects. systematic review. Gastroenterology 2002;122:26-33. doi:10.1053/
Gastroenterology 2003;125:1018-24. doi:10.1016/S0016- gast.2002.30297
5085(03)01210-1 49 Visrodia K, Singh S, Krishnamoorthi R, et al. Systematic review with
27 Clarke AT, Wirz AA, Manning JJ, Ballantyne SA, Alcorn DJ, McColl KE. meta-analysis: prevalent vs. incident oesophageal adenocarcinoma
Severe reflux disease is associated with an enlarged unbuffered and high-grade dysplasia in Barrett’s oesophagus. Aliment Pharmacol
proximal gastric acid pocket. Gut 2008;57:292-7. doi:10.1136/ Ther 2016;44:775-84. doi:10.1111/apt.13783
gut.2006.109421 50 Vaezi MF, Katzka D, Zerbib F. Extraesophageal symptoms and
28 Kahrilas PJ, McColl K, Fox M, et al. The acid pocket: a target for diseases attributed to GERD: where is the pendulum swinging
treatment in reflux disease?Am J Gastroenterol 2013;108:1058-64. now?Clin Gastroenterol Hepatol 2018;16:1018-29. doi:10.1016/j.
doi:10.1038/ajg.2013.132 cgh.2018.02.001
29 Rohof WO, Bennink RJ, Smout AJ, Thomas E, Boeckxstaens GE. An 51 Toros SZ, Toros AB, Yüksel OD, Ozel L, Akkaynak C, Naiboglu
alginate-antacid formulation localizes to the acid pocket to reduce B. Association of laryngopharyngeal manifestations and
acid reflux in patients with gastroesophageal reflux disease. Clin gastroesophageal reflux. Eur Arch Otorhinolaryngol 2009;266:403-
Gastroenterol Hepatol 2013;11:1585-91, quiz e90. doi:10.1016/j. 9. doi:10.1007/s00405-008-0761-2
cgh.2013.04.046 52 Zerbib F, Roman S, Bruley Des Varannes S, et al, Groupe Français
30 Souza RF, Huo X, Mittal V, et al. Gastroesophageal reflux might De Neuro-Gastroentérologie. Normal values of pharyngeal and
cause esophagitis through a cytokine-mediated mechanism rather esophageal 24-hour pH impedance in individuals on and off
than caustic acid injury. Gastroenterology 2009;137:1776-84. therapy and interobserver reproducibility. Clin Gastroenterol
doi:10.1053/j.gastro.2009.07.055 Hepatol 2013;11:366-72. doi:10.1016/j.cgh.2012.10.041
12 doi: 10.1136/bmj.m3786 | BMJ 2020;371:m3786 | the bmjYou can also read