All of Us Research Program and The Precision Medicine Initiative - Elizabeth Karlson, MD, MS May, 2018 - Joint Biology Consortium
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

All of Us Research Program and The Precision Medicine Initiative Elizabeth Karlson, MD, MS May, 2018
“My hope is that this becomes the foundation,
the architecture, whereby in 10 years from
now we can look back and say that we have
revolutionized medicine.”
—President Barack Obama
3
The All of Us Research Program
Mission
To accelerate health research and medical
breakthroughs, enabling individualized
prevention, treatment, and care for all of us.
• The cornerstone of the larger PMI – led by the NIH
• The largest-ever biomedical research study
st
• Funded at $1.5 Billion over 10 years (21 Century Cures Act)
• One million or more volunteers, reflecting the broad diversity of the U.S.
• Opportunities for volunteers to provide data on an ongoing basis over 10+ years
• A platform for research for decades to come
All of Us Core Principles • Participation in the All of Us Research Program will be open to interested individuals • The program will reflect the rich diversity of America • Participants will be partners in the program • Trust will be earned through robust engagement and full transparency • Participants will have access to information and data about themselves • Data from the program will be broadly accessible to empower research • The program will adhere to Privacy and Trust Principles and the Data Security Policy Principles and Framework • The program will be a catalyst for innovative research programs and policies

Our New England Consortium – 60% of enrollment at PHS, 40% at BMC
Partners HealthCare System* Boston Medical Center
Mass General Brigham & Women’s Newton-Wellesley Boston Medical Center
Chelsea Revere Jen Center Brookside Codman Square DotHouse Health
• New England’s largest regional system with • New England’s largest safety
more than five hospitals and affiliated net hospital with more than
community health centers. 65% underrepresented
• We plan recruitment activities at clinics and minorities.
community health centers that serve diverse • Includes Boston HealthNet
populations and are embedded in our network of 14 community
communities. health centers,
5 & 13 FQHCs.
* PHS includes other sites where we plan recruitment in subsequent years (e.g., Spaulding Rehabilitation Center and McLean Hospital).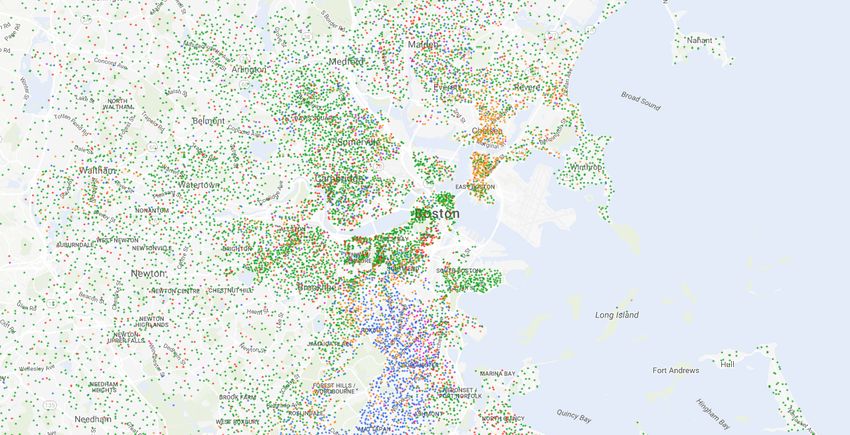
National Network of Inaugural Partners
National Trans-
Partners American
Precision Hudson River
Mayo Clinic Community Health Center, Inc.
Medicine Health Care
(Biobank)
Consortium
Regional New England Precision
Medical San Francisco
Medicine Consortium
General Hospital
Centers Foundation All of Us, Wisconsin
New York City Precision
Illinois Precision University of Medicine Consortium
FQHCs Medicine Consortium Pittsburgh
Wondros Federal Partners: HCM
Vanderbilt Univ. Medical White House, HHS, NIH,
Community Scripps Translational
Center, with Broad & Verily
(Data and Research Center)
ONC, HRSA, VA, USDS
Partners Science Institute
(Participant Center)
Cherokee
Health Eau Claire Vibrent
Systems Cooperative (Participant Technology
University of Arizona Southern All of Us
Health Center Systems Center)
California Precision (w/Banner Health) Network
Medicine Consortium
FiftyForward
Jackson-Hinds National Alliance
Comprehensive for Hispanic Health
San Ysidro Health Health Center
Center
Delta Research
SouthEast and Educational
Enrollment Center Foundation
All of Us New England Enrollment Sites
MGH Revere HealthCare Center
MGH Chelsea HealthCare Center
MGH Assembly Row Primary Care
Massachusetts General Hospital
Brigham and
Newton-Wellesley Women’s Hospital
Hospital
Boston Medical Center
Legend
Brookside Community Health Center Hospital
Faulkner Hospital
FQHC
DotHouse Health
SJP Community Health Center Community
Codman Square Health Center Health Center
Clinic
All of Us New England Enrollment Sites
Revere
Chelsea
MGH Assembly Row
Legend
MGH
BWH
BMC
NWH Brookside Hospital
Faulkner
FQHC
DotHouse
SJP Community
Codman Square Health Center
Clinic
9
Demographics at our Enrollment Sites
Clinic or Community Health Center & N (1 yr) I A B H W O U
BWH Phyllis Jen Center for Primary Care 15,580 - 4% 25% 12% 51% 4% 5%
MGH Chelsea HealthCare Center (CHC) 31,715 - 3% 6% 49% 30% 12% -
MGH Revere HealthCare Center (RHC) 21,205 - 9% 5% 12% 60% 14% -
MGH Everett Family Care (EFC) 6,350 - 6% 10% 11% 63% 10% -
BWH Brookside Community Health Center (BCH) 8,970 - 1% 9% 72% 13% 10% 2%
BWH Southern Jamaica Plain Health Center (SJP) 8,107 - 1% 12% 51% 29% 10% 2%
BWH Main Campus 448,940 - 3% 6% 6% 69% 3% 14%
MGH Main Campus 652,650 - 5% 5% 6% 75% 7% 6%
NWH Main Campus 208,945 - 6% 3% 2% 82% 3% 6%
BMC Main Campus 5% 28% 9% 37% 5% 16%
BMC Primary Care (Loyalty Cohort) 1% 3% 55% 14% 22% - 19%
BMC Codman Square 22,971 - 1% 91% 8% 5% 2% -
BMC DotHouse 23,094 1% 37% 34% 17% 13% 12% -
PHS metrics are unique patients in FY16 (10/01/15 to 09/30/2016), from EHR.
BMC metrics are from EHR for BMC Main and HRSA Health Center Program for Codman Square and DotHouse
10
Recruitment Strategies
⦿ Partners Biobank Recontact – Email blast to 50k Partners
Biobank participants yielded >1,000 consents in a week (2%). It
will skew our demographics to white/highly educated.
⦿ Clinic Recruitment – Challenge low consent rate (6%).
⦿ Employee Recruitment – Leadership enrollment campaigns,
email invitations, featuring enrollment of hospital leadership..
⦿ Partners Patient Research Portal – Passive strategy that
yields a few enrollments each day.
⦿ Volunteer Tabling: Many RAs report that this approach allows
them the time needed to speak to potential participants and
complete consent process, but it is hit/miss.
⦿ Planned: Email campaign to patients via Patient Gateway
• Engagement with local community organizations
• Engage Clinician Champions and Community Ambassadors
• Continued campaigns for employee awareness
• Media push for national launch with local news (print, web, TV)
• Regular radio slot on WZBR – The BASS of Boston
• Leverage existing relationships with local celebritiesAll of Us ℠ Research Program Data Collection
The Program will start by collecting a limited
set of standardized data from sources that will
include:
• Participant surveys
• Electronic health records
• A baseline physical evaluation
• Biospecimens (blood and urine
samples)
• Mobile/wearable technologies
• Geospatial/environmental data
Data types will grow and evolve with science,
technology, and trust.
All of UsSM | The Precision Medicine Initiative®Surveys
Baseline
• Basics
• Personal Health Habits
• Health Status
90 days after enrollment
• Healthcare Utilization
• Family medical history
• Personal medical history
• Medications
Under development
• Diet/Nutrition
• Physical activity/Occupation
• Social Determinants of
Health
• Mental Health/Substance
Abuse
• DisabilityA Transformational Approach to Data Access • Data sharing will be swift to both researchers and participants • Participants will have access to study information and data about themselves (eg. all results) • Data collection will start small and will grow over time • Privacy and security will adhere to the highest standards • Will invest to level the playing field so diverse researchers can play All of UsSM | The Precision Medicine Initiative®
14
Security Protections
• Maintaining data security and privacy within
the All of Us Research Program will be
paramount to maintaining participants’ trust
and engagement
• Extensive regulations, policies, governance,
compliance, and technical safeguards are
being implemented to ensure that participant
data security and privacy are appropriately
protected
• The Data Research Center applies an
iterative risk-based approach at the federal
guidelines (FISMA moderate baseline)15
FISMA & Significance to the All of Us Research Program …
FISMA was signed into law as part of the Electronic Government Act of 2002
•The National Institute of Standards and Technology (NIST) outlines 9 steps toward compliance
with FISMA:
(1) Categorize the information to be protected
(2) Select minimum baseline controls
(3) Refine controls using a risk assessment procedure
(4) Document the controls in the system security plan
(5) Implement security controls in appropriate information systems
(6) Assess the effectiveness of the security controls once they have been implemented
(7) Determine agency-level risk to the mission or business case
(8) Authorize the information systems for processing
(9) Monitor the security controls on a continuous basis
• By following the principled approach, combined with meeting the FISMA compliance
requirements, we will implement the core data security functions of identify, Protect, Detect,
Respond, and Recover at all TimesData Access: Background Concepts
Data Tiers i) Public - Data that poses minimal risks to the
privacy of research participants. It can be
Public
accessed without logging into the Platform.
Registered
ii) Registered- Data that has some risk of
identifying research participants and therefore
Controlled poses some privacy risk to participants. It can
only be accessed after logging into the
Research Platform. Access to this data will be
logged and may be audited.
All data tiers have obvious iii) Controlled - Data that poses the most
identifiers removed
significant risks to the privacy of research
Access to identifiers, recontact, participants, and researchers must be approved
or biospecimens requires new
IRB proposal
by the RAB to access it.Process for Accessing Data
Workspaces 21st Century Cures Act
“...on the appropriate Internet website of the
Department of Health and Human Services, identify
any entities with access to such information and
provide information with respect to the purpose of
such access, a summary of the research project for
which such access is granted, as applicable, and a
description of the biological material and associated
information to which the entity has access.”
Curated Data
Repository
Each workspace will have a researcher purpose associated with it in both human-
and machine-readable form. We plan to post every workspace, along with the
researchers that are members of it, along with the research purposeData Access Protocol
Public Registered Controlled
Access Registration and Identity Registration and Identity
(no login required) Verification Verification
Research Ethics Training Research Ethics Training
Sign Code of Conduct Sign Code of Conduct
eRA Commons ID
RAB Approval RAB Approval
Create Workspace and state Create Workspace and state
purpose purpose
Access Data Access DataI. Definition of AoU Authorized User
Any individual may become an All of Us Researcher (AOU Researcher) if
they attest to the Code of Conduct:
•I will:
•Read and respect the All of Us Research Program core values
•Respect the security and privacy of research participants at all times, and as
soon as possible report any violations that I observe to the RAB
•Follow all applicable US and state laws
•Credit the All of Us Research Program and its research participants in talks and
publications
•Allow my queries and work to be logged and audited for monitoring compliance
•Provide a meaningful description of my research purpose for the benefit of
research participants and the scientific community
•Respond to requests from participants and the public about my research or its
purpose using All of Us Research Program
•Researchers using All of Us Research Program data agree to deposit to National
Library of Medicine's PubMed Central an electronic version of their final, peer-
reviewed manuscripts upon acceptance for publication, to be made publicly
available no later than 12 months after the official date of publicationII. Code of Conduct
•I will:
•NOT attempt to re-identify research participants or their relatives
•NOT redistribute individual-level All of Us data
•NOT use All of Us data for advertising purposes
•NOT use All of Us data for research that is discriminatory or stigmatizing of
individuals, families, or communities
•NOT attempt to contact All of Us participants without explicit approval from
the RAB
•NOT share my login information with any other user
•NOT download individual-level data resources without approval from CAPS
(including taking screenshots or other means of acquiring individual-level
data)
•NOT attempt to link individual-level All of Us data with individual-level data
from other sources without explicit permission from RAB
•NOT represent that the All of Us Research Program endorses or approves
of my researchIII. Punishments for Bad Behavior
Violations of the Code of Conduct
The RAB will determine whether an investigator has violated the Code of
Conduct and notify the All of Us Research Program office of the violation.
The AOURP office will:
Notify the investigator of any violation of the AOURP Code of Conduct.
Potentially revoke and/or deny access by violator to all non-public
AOU data.
Potentially post name and affiliation of violator on public AOURP
webpage.
The AOURP will work with the Office of the General Counsel at HHS to
understand all options for enforcement of violations to Controlled Access
Data.
Violations involving malicious misuse or breach of the AOURP data system
may also have legal liabilities under the Federal Information Security
Management Act (FISMA).Certificate of Confidentiality 9
• All of Us at Partners Healthcare holds a Certificate of Confidentiality
affording protections as expanded under the 21st Century Cures Act
• Protections cover:
• Identifiable and potentially identifiable information
• All copies of that information and associated biospecimens
• Protections include:
• Mandatory withholding from all non-research personnel including for
the purposes of legal proceedings
• Immunity from the legal process
• Exceptions to mandatory withholding include:
• Federal, state, or local legal requirements
• Medical treatment of the individual
• With individual’s consent
• For research23
All of Us consent form: COC text
All of Us has Certificates of Confidentiality from the U.S. government. These will help us fight
any legal demand (such as a court order or a request from federal, state, or local law
enforcement) to give out information that could identify you.
• There are a few times when we might need to give out your name or other information that
identifies you.
• We will give out information about you to protect your health or the health of others.
• If we learn or suspect that you are being abused.
• If we learn or suspect you are abusing, neglecting or have abandoned someone who depends
on you for care, like a child or dependent adult.
• If we learn that you plan to harm yourself or someone. If we learn that you have a disease that
is a risk to public health, like measles.
• We will give out any data needed to meet U.S. research laws and regulations. This may include
information that identifies you.24
Talking Points: Privacy
Who gets access to my personal data?
• Study staff who work on processing the data need access to identifiable data
• Staff with secure, password-protected access to the identifiable data
• Will go through a security clearance
• Take ethics training
• Follow strict privacy guidelines
• Go through portal to access data
• Are monitored and auditedScientific Opportunities: > 1300 studies proposed to date Develop quantitative estimates of risk for a range of diseases by integrating environmental exposures and genetic factors Identify the causes of individual variation in response to commonly used therapeutics = pharmacogenomics Discover biological markers that signal increased or decreased risk of developing common diseases Develop solutions to health disparities Use mobile health technologies to correlate activity, physiological measures, and environmental exposures with health outcomes Empower study participants with data and information to improve their own health Create a platform to enable trials of targeted therapies
The Value of Participating in All of Us ⦿An opportunity to learn some of your own health indicators and get your own data ⦿An opportunity to fight disease and improve the health of future generations ⦿The opportunity to ensure that your community is included in the studies that may lead to new understanding and new treatments ⦿The opportunity to be part of a movement to make our health care more precise, more personal, and more effective
How We Became Involved in All of Us: Partners Biobank
• Repository of consented patient samples linked to
the EHR, supplemented with genomic data and PPI
• 84,000+ patients enrolled; ~2000 added/month
• Infrastructure and workflows mirror AoU:
• Electronic Consent: In-person and online
• CLIA-certified biobanking
• Consent for re-contact for additional studies
• Enterprise-wide marketing of the study
• Community engagement
• Return of research results
• Automated pipeline for linkage of rich phenotype data from the EHR and PPI
• State-of-the-art and comprehensive suite of IT solutions for enrollment and data management
• Data sharing with national repositories.What’s Involved in Joining All of Us New England? 1. Complete informed consent process (www.joinallofus.org) 2. Complete 3 surveys 3. Schedule and complete visit for physical measurements and blood/urine sample collection (at MGH, Assembly Row Primary Care, NWH, MGH, BWH or community health center) 4. OR complete all at once by stopping by our information desks
Thank you! Want to learn more? • Visit https://www.joinallofus.org/en • Call us at (617) 768-8300
You can also read