Pathology Update 2020 - RCPA
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Diagnosis of Malignant Mesothelioma &
Other Diffuse Pleural Tumours
Pathology Update 2020
Saturday, 21 March 2020
Jeffrey L. Myers, M.D.
A. James French Professor of Diagnostic Pathology
Vice Chair for Clinical Affairs & Quality
Director, MLabs
Interim Director, Anatomic Pathology
University of Michigan, Ann Arbor, MI
myerjeff@med.umich.edu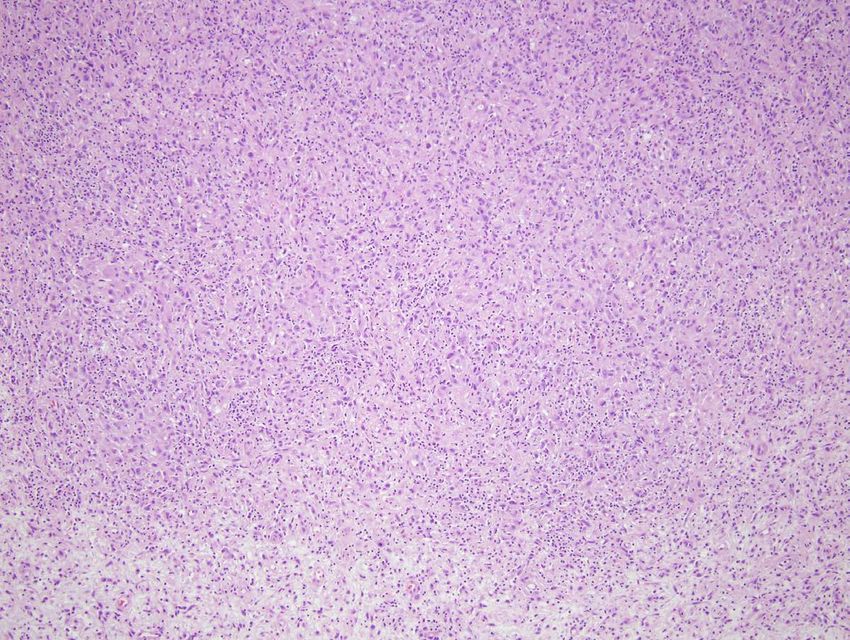
Diagnosis of Malignant Mesothelioma &
Other Diffuse Pleural Tumours
No disclosures relevant to this talk.
Jeffrey L. Myers, M.D.
A. James French Professor of Diagnostic Pathology
Vice Chair for Clinical Affairs & Quality
Director, MLabs
Interim Director, Anatomic Pathology
University of Michigan, Ann Arbor, MI
myerjeff@med.umich.edu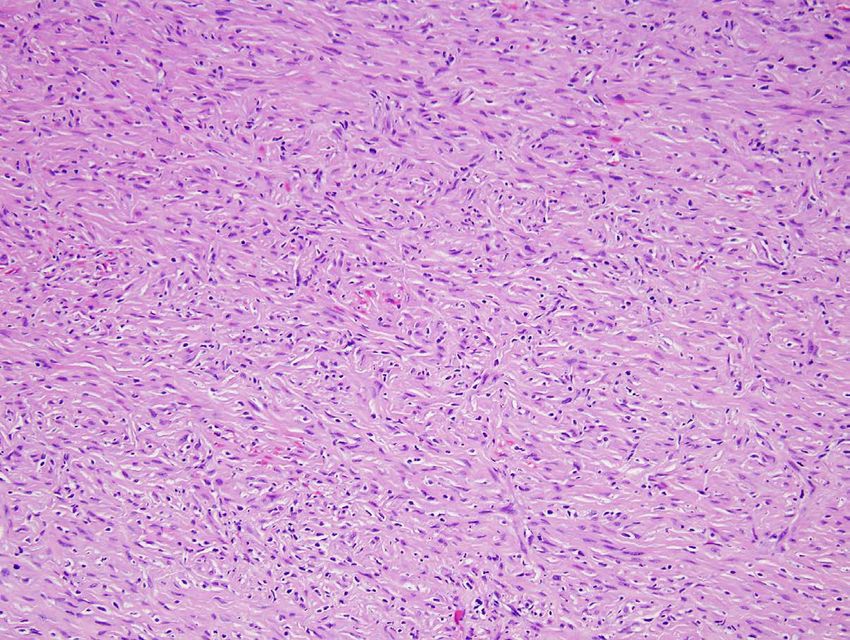
Diffuse Pleural Tumours
Objectives
• apply current criteria to histopathologic diagnosis of
malignant mesothelioma,
• appropriately apply immunohistochemistry to
separate mesothelioma from its mimics, and
• appropriately apply immunohistochemical stains and
molecular tests helpful in separating benign from
malignant mesothelial proliferations.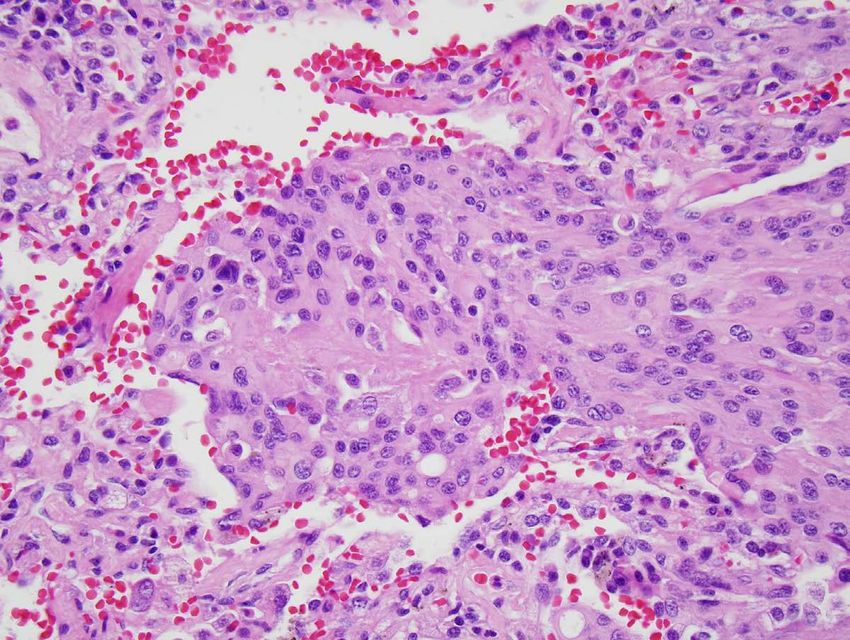
Diffuse Pleural Tumours • Diffuse mesothelioma • Pseudomesotheliomatous carcinoma • Epithelioid hemangioendothelioma • Benign vs malignant mesothelial proliferations

[Diffuse] Malignant Mesothelioma
Definition†
a malignant tumor originating from
mesothelial cells and showing
epithelioid/mesenchymal/spindle cell
morphology and a diffuse pattern of growth
over the pleural surfaces.
†modified from Galateau-Salle et al. IN: WHO Classification of Tumours of the
Lung, Pleura, Thymus and Heart. Lyon: IARC Press; 2015: 156.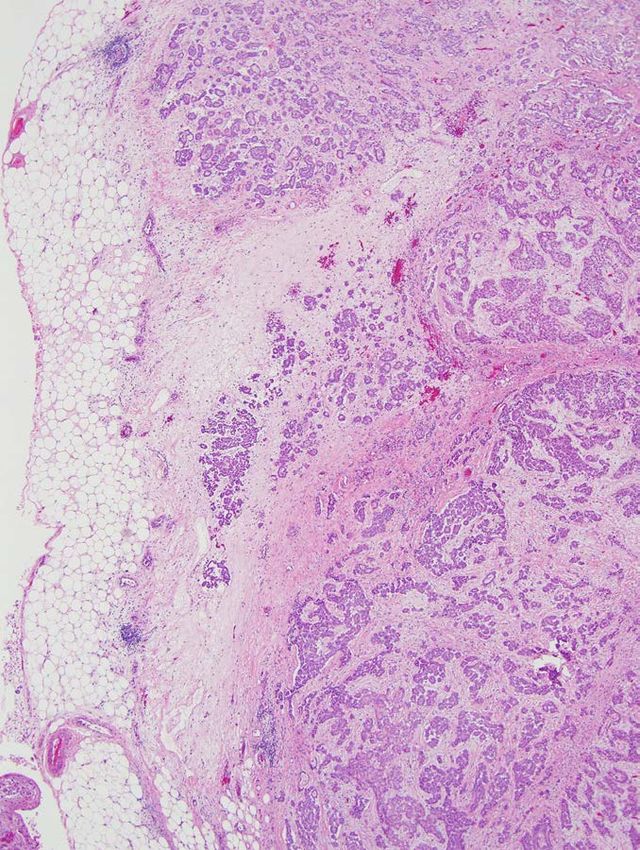
Malignant Mesothelioma
Clinical Findings
• median age ~ 60 years
• men>>women
• chest pain, shortness of breath
• metastases uncommon as presenting feature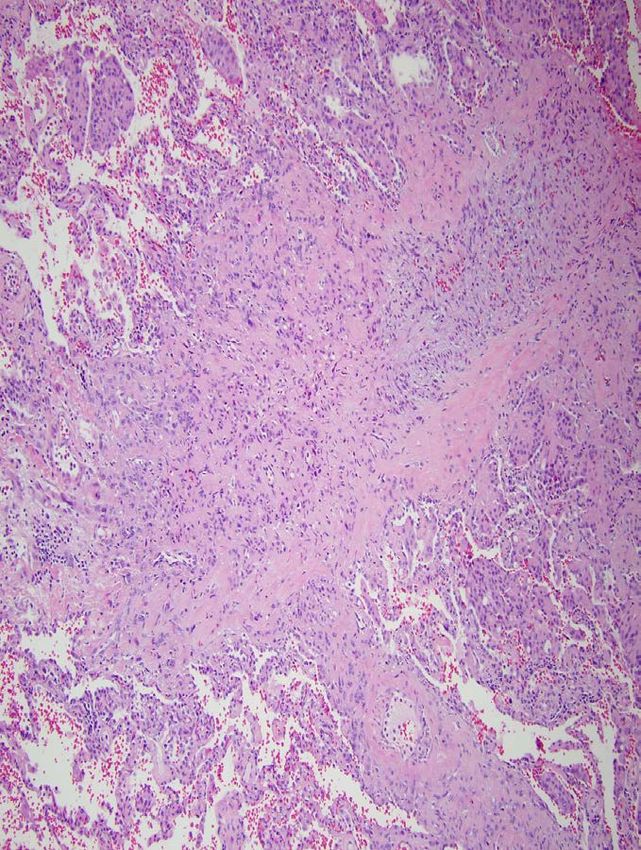
Malignant Mesothelioma
Radiological Findings
• pleural effusion in >
90%
• pleural nodularity/
thickening
• Involvement of medial/
mediastinal pleural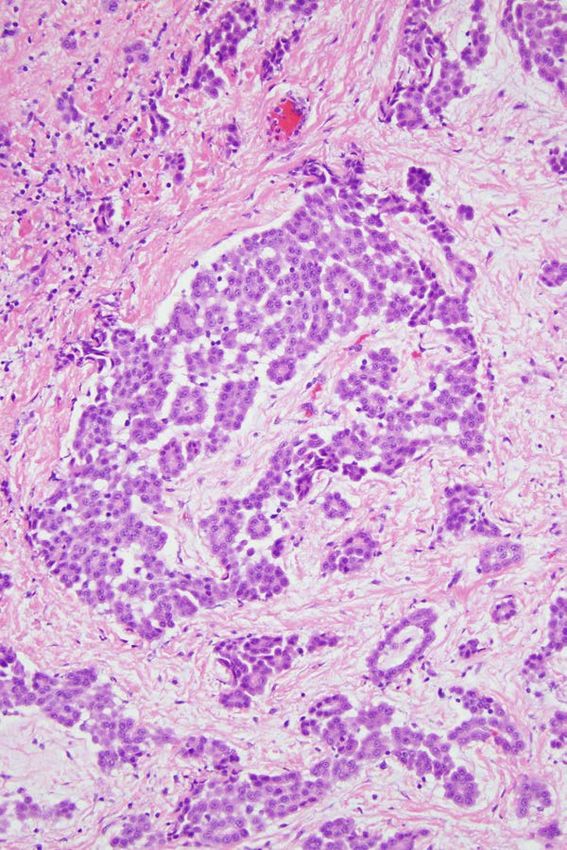
Malignant Mesothelioma
Link Between Epidemiology and Practice†
“. . . a history of exposure to asbestos
should play no role in diagnosis; diagnosis
depends only on the gross, microscopic, and
special technique observations, as it does
with any other tumor.”
†Churg,
Cagle, & Roggli: Tumors of the Serosal Membranes. Atlas of
Tumor Pathology, 4th Series, 2006.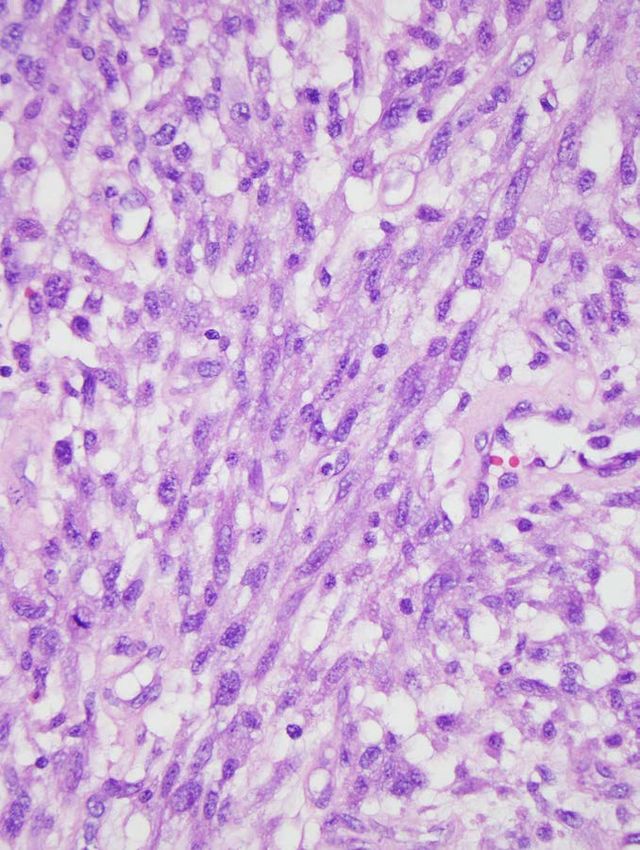
Pleural Mesotheliomas Histologic Subclassification in 382 Cases* • epithelial (epithelioid) 55% • biphasic 24% • sarcomatous (sarcomatoid) 22% *from Legha et al. Ann Int Med 1977; 87: 613
KER CALR
WT-1Pleural Mesotheliomas
Variants of Epithelioid Mesothelioma
• solid • clear cell
• tubulopapillary • transitional
• trabecular • deciduoid
• micropapillary • small cell
• microcystic • pleomorphic
(adenomatoid) • lymphohistiocytoidPleural Mesotheliomas Histologic Subclassification in 382 Cases* • epithelial (epithelioid) 55% • mixed 24% *from Legha et al. Ann Int Med 1977; 87: 613
Pleural Mesotheliomas Histologic Subclassification in 382 Cases* • epithelial (epithelioid) 55% • mixed 24% • sarcomatous (sarcomatoid) 22% *from Legha et al. Ann Int Med 1977; 87: 613
Pleural Mesotheliomas
Unusual Histologic Features
sarcomatous (sarcomatoid)
– mesothelioma with heterologous (rhabdo-,
osteo-, chondrosarcomatous) elements
– desmoplastic mesotheliomaKER CALR
Malignant Mesothelioma
Differential Diagnosis – Malignant
Mesothelioma Type Differential Diagnosis
met adenocarcinoma
epithelioid
Epithelioid hemangioendothelioma
epithelioid angiosarcoma
sarcomatoid carcinoma
Mixed synovial sarcoma
sarcomatoid carcinoma
Sarcomatoid synovial sarcoma
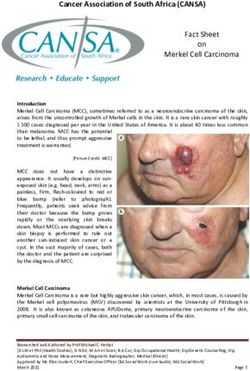
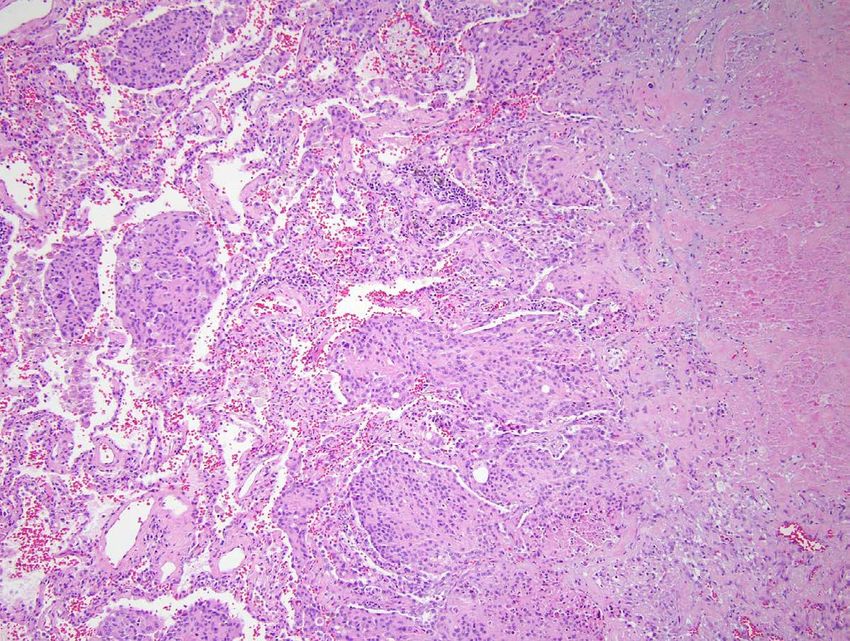
angiosarcomaPseudomesotheliomatous Carcinoma
Metastatic Attanoos & Gibb,
breast ca Histopathology 2003; 43: 444
(n = 53)
lung 47 (89%)
adca 34 (72%)
sq cell 4 (9%)
small cell 2 (4%)
other 7 (15%)
non-lung 6 (11%)
urothelial 2 pancreas 1
Lung RCC 1 prostate 1
adenoca parotid 1Pleural Mesotheliomas
Immunostains in Epithelioid Mesothelioma
Marker Sensitivity Specificity
MESOTHELIAL
calretinin > 90% 90-95%
CK 5/6 75-100% 80-90%
WT1 70-95% ≈ 100%
D2-40 90-100% 85%
ADENOCARCINOMA
MOC31 95-100% 85-98%
BerEP4 95-100% 74-87%
BG8 (Lewis Y) 90-100% 93-97%
CEA (monoclonal) 80-100% > 95%Pleural Mesotheliomas
Immunostains in Epithelioid Mesothelioma
Marker Sensitivity Specificity
MESOTHELIAL
calretinin > 90% 90-95%
“aCKthree-antibody
5/6 immunohistochemical
75-100% panel
80-90%
including
WT1 calretinen, BG8, and MOC-31 . ≈. 100%
70-95% . provided
over 96% sensitivity and specificity for distinguishing
D2-40 90-100% 85%
epithelioid mesothelioma from AdCA.”
ADENOCARCINOMA Yaziji et al. Mod Pathol 2006
MOC31 95-100% 85-98%
BerEP4 95-100% 74-87%
BG8 (Lewis Y) 90-100% 93-97%
CEA (monoclonal) 80-100% > 95%Malignant Mesothelioma
Differential Diagnosis – Malignant
Mesothelioma Type Differential Diagnosis
met adenocarcinoma
epithelioid
Epithelioid hemangioendothelioma
epithelioid angiosarcoma
sarcomatoid carcinoma
Mixed synovial sarcoma
sarcomatoid carcinoma
Sarcomatoid angiosarcoma
synovial sarcomaPleural Mesotheliomas
Immunostains in Sarcomatoid Mesothelioma†
• sarcomatoid mesotheliomas almost invariably stain, at
least focally, with the
AE1/AE3 broad-spectrum antikeratin antibody
cocktail,
the pancytokeratin antibodies OSCAR and KL1,
as well as with the CAM5.2 antibody
• keratin negative in 5-10%
†Galateau-Salleet al. Epithelioid Mesothelioma. IN: Travis et al. (editors) WHO Classification
of Tumours of the Lung, Pleura, Thymus and Heart. Lyon: IARC Press; 2015: 156.Pleural Mesotheliomas
Sarcomatoid Mesothelioma vs Sarcomatoid Carcinoma†
100%
90%
75%
Sarcomatoid meso
Sarcomatoid carcinoma
50% 45% 42%
73%
25% 21%
12%
0%
AE1/3 EMA CK5/6 CALR D2-40 WT1 p40 p63 CEA (m) TTF1
†Marchevsky et al. Hum Pathol 2017; 67: 160-8.Pleural Mesotheliomas
Sarcomatoid Mesothelioma vs Sarcomatoid Carcinoma†
GATA3 positive (strong, diffuse)
100%
in nearly all sarcomatoid mesotheliomas
100%
Total Score
(intensity
75% +
diffuseness)
sarcomatoid mesothelioma
0-1
50% 2-6
25%
15%
sarcomatoid carcinoma
0%
SMM (19) SCa (13)
†Berg and Churg. GATA3 Immunohistochemistry for Distinguishing Sarcomatoid and Desmoplastic
Mesothelioma From Sarcomatoid Carcinoma of the Lung. Am J Surg Pathol 2017; 41: 1221-5.Malignant Mesothelioma
Differential Diagnosis – Malignant
Mesothelioma Type Differential Diagnosis
met adenocarcinoma
epithelioid
Epithelioid hemangioendothelioma
epithelioid angiosarcoma
sarcomatoid carcinoma
Mixed synovial sarcoma
sarcomatoid carcinoma
Sarcomatoid synovial sarcoma
angiosarcomaDiffuse Pleural Tumours • Diffuse mesothelioma • Pseudomesotheliomatous carcinoma • Epithelioid hemangioendothelioma
Epithelioid Hemangioendothelioma
Definition†
“. . . a malignant endothelial neoplasm
composed of cords of epithelioid
endothelial cells and characterized in most
cases by WWTR1-CAMTA1 gene fusion.”
†Galateau-Salle et al. IN: WHO Classification of Tumours of the Lung, Pleura,
Thymus and Heart. Lyon: IARC Press; 2015: 156.Epithelioid Hemangioendothelioma
Radiological Findings
• multiple, bilateral nodules (1-2 cms), ± Ca++
• differential diagnosis: metastases
granulomatous diseaseEpithelioid Hemangioendothelioma
Pathologic Features
• central necrosis/hyalinization
• epithelioid “histiocyte-like” cytology with coarse
cytoplasmic vacuoles
• intralumenal “polyps” resembling organizing
pneumonia
• growth along lymphatic pathwaysEpithelioid Hemangioendothelioma
Unusual Manifestations
• solitary nodule
• lymphangitic metastases
• diffuse “interstitial lung disease”
• diffuse pleural involvementKER
Epithelioid Hemangioendothelioma
Immunohistochemical and Molecular
Findings†
Immunohistochemistry
ERG pos (100%)
CD31 pos (100%)
CD34 pos ( 81%)
D2-40 pos ( 71%)
ERG
pankeratin ± (31%)
CK8.18 ± (30%)
FLI-1 pos (100%)
FISH/RT-PCR
WWTR1-CAMTA1 33/35
YAP1-TFE3 2/35
†Flucke et al. Diagn Pathol 2014; 9:131.Diffuse Pleural Tumours • Diffuse mesothelioma • Pseudomesotheliomatous carcinoma • Epithelioid hemangioendothelioma • Benign vs malignant mesothelial proliferations
“the issue of whether a mesothelial
proliferation is benign or malignant is now
the most frequent question in the cases
circulated to the whole US-Canadian
[Mesothelioma Reference] Panel”
Churg & Galateau-Salle. Arch Pathol Lab Med 2012; 136: 1217Malignant > Benign Mesothelial
Proliferations †
•hemorrhagic effusion
•circumferential pleural thickening
(mediastinal pleura)
•nodular pleural thickening
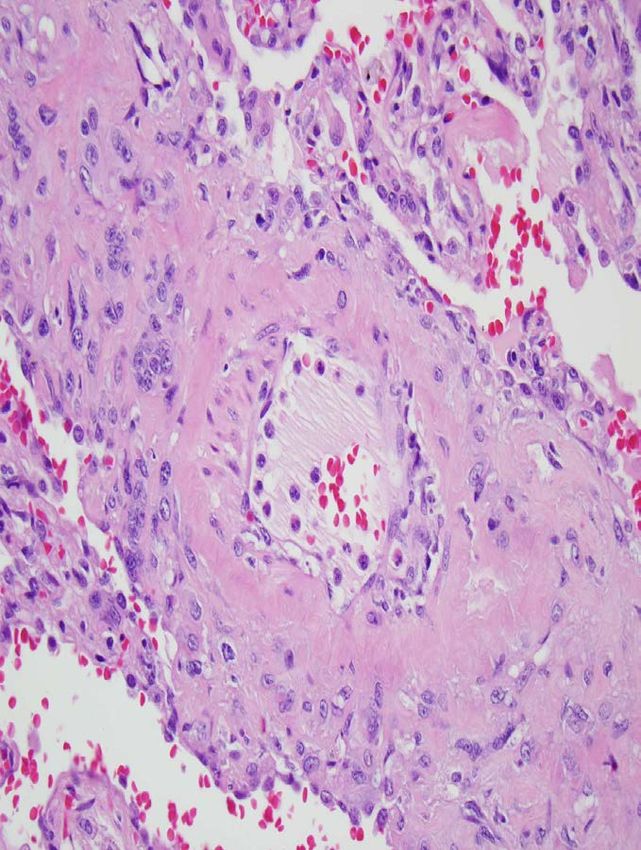
Churg & Galateau-Salle. Arch Pathol Lab Med 2012; 136: 1217Benign vs Malignant
Mesothelial
Proliferations†
“unless one has overt tumor
fragments, invasion of the
stroma remains the single
best criterion for diagnosing
malignant mesothelioma.”
“Pan-keratin stains can be
extremely helpful in showing
subtle invasion that may not
be readily apparent on
keratin stains useful for hematoxylin-eosin-stained
demonstrating invasion specimens.”
†Galateau-Salle et al. J Thorac Oncol 2016; 11: 142-54.Benign vs Malignant
Mesothelial Proliferations†
Atypical Mesothelial Malignant
Histologic Feature Hyperplasia Mesothelioma
Stromal invasion absent present
full thickness,
Cellularity, growth surface, layering, nodules,
pattern zonal expansile,
random
simple, single-cell complex,
Papillae
layer stratification
capillaries
irregular,
Vascularity perpendicular to
haphazard
pleural surface
†Galateau-Salle et al. J Thorac Oncol 2016; 11: 142-54.Benign vs Malignant
Mesothelial Proliferations†
Atypical Mesothelial Malignant
Histologic Feature Hyperplasia Mesothelioma
Stromal invasion absent present
full thickness,
Cellularity, growth surface, layering, nodules,
pattern zonal expansile,
random
simple, single-cell complex,
Papillae
layer stratification
capillaries
irregular,
Vascularity perpendicular to
haphazard
pleural surface
†Galateau-Salle et al. J Thorac Oncol 2016; 11: 142-54.“layering”
non-invasive, zonal distribution of mesothelial
cells = benignBenign vs Malignant
Mesothelial Proliferations†
Atypical Mesothelial Malignant
Histologic Feature Hyperplasia Mesothelioma
Stromal invasion absent present
full thickness,
Cellularity, growth surface, layering, nodules,
pattern zonal expansile,
random
simple, single-cell complex,
Papillae
layer stratification
capillaries
irregular,
Vascularity perpendicular to
haphazard
pleural surface
†Galateau-Salle et al. J Thorac Oncol 2016; 11: 142-54.“full thickness”/random variation in cellularity
≈ malignanttumefactive nodules away from pleural surface
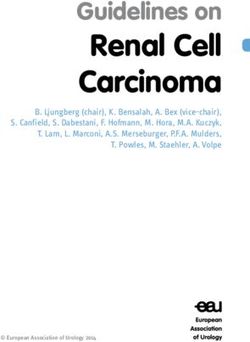
≈ malignantDesmoplastic Mesothelioma†
“Desmoplastic mesothelioma is
characterized by areas of atypical
spindle cells arranged in a so-called
patternless pattern within a dense,
hyalinized, fibrous stroma constituting
at least 50% of the tumour.”
†Roggliet al. IN: WHO Classification of Tumours of the
Lung, Pleura, Thymus and Heart. Lyon: IARC Press; 2015.Desmoplastic Mesothelioma vs Fibrous Pleurisy†
• paucicelluar, storiform or “patternless pattern
of Stout”
+
• invasion (chest wall and/or lung), or
• bland necrosis, or
• frankly sarcomatoid areas, or
• distant metastases
†Mangano et al. Am J Clin Pathol 1998; 110: 191-9Benign vs Malignant Mesothelial Proliferations
Emergence of Molecular Tools
recurrent alterations in multiple genes that function as tumor suppressors
BAP1 (BRCA1-associated protein 1)
• DNA repair, proliferation, cell cycle, cell death
• IHC – wild type = positive nuclear staining (NEGATIVE result)
mutations/deletions = negative staining (POSITIVE result)
Frequency of BAP1 Loss by
Immunohistochemistry
loss of
expression Mesothelioma
Mixed/ Benign Meso
Epithelioid Sarcomatoid Proliferations
internal
controls 56% - 81% 10% - 60% 0
from Sheffield et al. AJSP 2015; 39: 977Benign vs Malignant Mesothelial Proliferations
Emergence of Molecular Tools
recurrent alterations in multiple genes that function as tumor suppressors
p16INK4a (CDKN2A) – 9p21.3 CDKN2A (p16) – orange
chromosome 9 – green
• prevents cell cycle progression
• FISH – deletion
90%
80% p16 pos (IHC)
70%
60%
p16 deletion
(FISH)
50%
40%
Paraffin-Embedded Tissue
30% 52 mesotheliomas
20% 28 TMA, 24 whole sections
10% 40 acute & chronic pleuritis
0%
pleural pleuritis Chiosea et al. Mod Pathol 2008; 21: 742
mesotheliomaSarcomatous/Desmoplastic Mesothelioma
Role of BAP1 IHC and p16 FISH†
100%
p16 deletion • p16 deletion more sensitive than BAP1
BAP1 loss loss
75% • small increase in sensitivity by using
both (17/20 vs 16/20)
50% • p16 deletion cannot reliably distinguish
89%
SMM from sarcomatoid carcinoma
73%
25%
22% 27%
9%
0%
DMM (11) SMM (9) sarc ca (13)
†Hwang et al. Am J Surg Pathol 2016; 40: 714-8Benign vs Malignant Mesothelial Proliferations
Role of IHC for BAP1 and MTAP†
recurrent alterations in multiple genes that function as tumor suppressors
MTAP (methylthioadenosine phosphorylase)
• polyamine metabolism and adenine and methionine salvage
• IHC – wild type = positive nuclear staining (NEGATIVE result)
mutations/deletions = negative staining (POSITIVE result)
Sensitivity Specificity
MTAP 45% 100%
BAP1 61% 100%
BAP1/MTAP 77% 100%
9p21 FISH 61% 100%
BAP1/9p21 FISH 84% 100%
†Hida et al. Lung Cancer 2017; 104: 98-105Take Home Messages • Diagnosis of malignant mesotheliomas begins (and sometimes ends) with routine histology and knowledge of disease distribution. • Immunostains useful to distinguish metastatic carcinoma from epithelioid mesotheliomas, and are less useful in sarcomatoid variants. • EHE is a rare mimic of diffuse pleural mesothelioma. • IHC and molecular assays useful in separating benign mesothelial proliferations from mesothelioma
Diffuse Pleural Tumours
Objectives
• apply current criteria to histopathologic diagnosis of
malignant mesothelioma,
• appropriately apply immunohistochemistry to
separate mesothelioma from its mimics, and
• appropriately apply immunohistochemical stains and
molecular tests helpful in separating benign from
malignant mesothelial proliferations.myerjeff@med.umich.edu
You can also read