Understanding Non-Hodgkin Lymphoma - A guide for people with cancer, their families and friends
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Understanding
Non-Hodgkin
Lymphoma
A guide for people with cancer,
their families and friends
Cancer
information
www.cancercouncil.com.auUnderstanding Non-Hodgkin Lymphoma A guide for people with cancer, their families and friends First published May 2002 (as Understanding Non-Hodgkin’s Lymphoma). This edition December 2013. © The Cancer Council NSW 2013 ISBN 978 1 921619 94 6 Understanding Non-Hodgkin Lymphoma is reviewed approximately every two years. Check the publication date above to ensure this copy is up to date. Acknowledgements We thank the reviewers of this booklet: Dr Emily Blyth, Haematologist and Bone Marrow Transplant Physician, Westmead Hospital, NSW; Jason Gardner, Consumer; Carol Hargreaves, Cancer Information Consultant, Cancer Council NSW Helpline; and Cathie Milton, Clinical Nurse Consultant Haematology, Calvary Mater Newcastle, NSW. Editor: Ainsley Burgess Designer: Luisa Chisari Printer: SOS Print + Media Group Note to reader Always consult your doctor about matters that affect your health. This booklet is intended as a general introduction to the topic and should not be seen as a substitute for medical, legal or financial advice. You should obtain appropriate independent professional advice relevant to your specific situation and you may wish to discuss issues raised in this book with them. All care is taken to ensure that the information in this booklet is accurate at the time of publication. Please note that information on cancer, including the diagnosis, treatment and prevention of cancer, is constantly being updated and revised by medical professionals and the research community. Cancer Council Australia and its members exclude all liability for any injury, loss or damage incurred by use of or reliance on the information provided in this booklet. Cancer Council NSW Cancer Council is the leading cancer charity in NSW. It plays a unique and important role in the fight against cancer through undertaking high-quality research, advocating on cancer issues, providing information and services to the public and people with cancer, and raising funds for cancer programs. This booklet is funded through the generosity of the people of NSW. To make a donation to help defeat cancer, visit Cancer Council’s website at www.cancercouncil.com.au or phone 1300 780 113. Cancer Council NSW 153 Dowling Street, Woolloomooloo NSW 2011 Cancer Council Helpline 13 11 20 Telephone 02 9334 1900 Facsimile 02 9334 1741 Email feedback@nswcc.org.au Website www.cancercouncil.com.au ABN 51 116 463 846
Introduction
This booklet has been prepared to help you understand more about
non-Hodgkin lymphoma. This is also known as non-Hodgkin’s
lymphoma or lymphatic cancer as it affects the lymph nodes.
Many people feel understandably shocked and upset when told they
have non-Hodgkin lymphoma. We hope this booklet will help you
understand how the disease is diagnosed and treated.
We cannot advise you what is the best treatment for you. You need
to discuss this with your doctor. However, we hope this information
will answer some of your questions and help you think about
questions you may want to ask your doctor or other health carers.
You may like to pass this booklet on to your family and friends for
their information. This booklet does not need to be read from cover
to cover – just read the parts that are useful to you. Some medical
terms are defined in the glossary on page 54.
Different lymphomas
There are two main types called Reed-Sternberg is
of lymphatic cancers: seen in Hodgkin lymphoma,
non-Hodgkin lymphoma but it is not found in non-
(85% of cases) and Hodgkin Hodgkin lymphoma.
lymphoma (15% of cases).
For a free booklet on Hodgkin
The difference between the lymphoma, call Cancer Council
lymphomas is how they look Helpline 13 11 20.
under a microscope. A cellContents What is cancer?................................................................. 4 The lymphatic system....................................................... 6 Key questions.................................................................... 8 What is non-Hodgkin lymphoma?......................................................... 8 What types are there?........................................................................... 8 What are the causes?............................................................................ 9 What are the symptoms?.................................................................... 10 How common is it?............................................................................. 10 Diagnosis.......................................................................... 11 Biopsy................................................................................................. 11 Further tests........................................................................................ 12 Prognosis............................................................................................ 16 Stages of non-Hodgkin lymphoma..................................................... 17 Which health professionals will I see?................................................. 18 Key points........................................................................................... 20 Treatment......................................................................... 21 Low-grade (indolent) lymphoma......................................................... 21 High-grade (aggressive) lymphoma.................................................... 22 Chemotherapy..................................................................................... 23 Biological therapies............................................................................. 26 Radiotherapy....................................................................................... 27 Steroid therapy.................................................................................... 29 Peripheral blood stem cell transplant.................................................. 30 Palliative treatment.............................................................................. 35 Key points........................................................................................... 36
Making treatment decisions........................................... 37 Talking with doctors............................................................................ 38 A second opinion................................................................................ 38 Taking part in a clinical trial................................................................. 39 Looking after yourself..................................................... 40 Healthy eating..................................................................................... 40 Being active......................................................................................... 40 Complementary therapies................................................................... 41 Relationships with others.................................................................... 42 Sexuality, intimacy and cancer............................................................ 43 Changing body image......................................................................... 44 Life after treatment.............................................................................. 45 What if lymphoma returns?................................................................. 47 Seeking support.............................................................. 48 Practical and financial help................................................................. 49 Talk to someone who’s been there...................................................... 50 Caring for someone with cancer................................... 51 Useful websites............................................................... 52 Question checklist........................................................... 53 Glossary........................................................................... 54 How you can help............................................................ 60
What is cancer?
Cancer is a disease of the cells, which are the body’s basic
building blocks. Our bodies constantly make new cells to help
us grow, to replace worn-out cells and to heal damaged cells
after an injury.
Normally, cells multiply and die in an orderly way but sometimes
something goes wrong with this process and cells grow in an
uncontrolled way. This uncontrolled growth may cause blood
or lymph fluid in the body to become abnormal, or form a lump
called a tumour. A tumour can be benign or malignant.
• Benign tumour – Cells are confined to one area and are not
able to spread to other parts of the body. This is not cancer.
• Malignant tumour – This is made up of cancerous cells, which
have the ability to spread by travelling through the bloodstream
or lymphatic system (lymph fluid).
The cancer that first develops in a tissue or organ is called the
primary cancer. A malignant tumour is usually named after the
organ or type of cell affected. A tumour that has not spread to
other parts of the body is called a localised cancer. A malignant
tumour may invade deeper into surrounding tissue and can grow
its own blood vessels (angiogenesis).
With cancers that affect the blood and bone marrow, abnormal
cells multiply in such a way that they crowd the bone marrow
and reduce its ability to make normal blood cells. Sometimes the
abnormal cells also clump together to form a tumour.
4 Cancer CouncilIf you have non-Hodgkin lymphoma, which is a type of blood
cancer, the cancer cells usually affect and enlarge your lymph
nodes at one or more lymph node sites around the body. The
cancer cells can spread to any organ, in particular, the bone
marrow, spleen and liver. Occasionally, it can spread to the brain
and spinal cord.
When cancer spreads it is called a secondary cancer, a metastasis
or advanced cancer. A metastasis keeps the name of the original
cancer. For example, non-Hodgkin lymphoma that has spread to
the liver is still called non-Hodgkin lymphoma.
How cancer starts
Normal cells Abnormal Angiogenesis
cells
Boundary
Lymph vessel
Blood vessel
Normal cells Abnormal cells Abnormal cells Malignant or
multiply invasive cancer
What is cancer? 5The lymphatic system
Non-Hodgkin lymphoma is a cancer of the white blood cells that
starts in the lymphatic system. The lymphatic system is a key
part of the immune system, which helps protect the body against
disease and infection.
The lymphatic system includes a network of thin tubes (lymph
vessels) found throughout the body, as well as organs, such as the
spleen and thymus.
Lymph vessels carry a clear fluid called lymph. This fluid
travels to and from tissue in the body before being emptied
into the bloodstream. Lymph contains white blood cells
called lymphocytes, which help fight infection. The two main
types of lymphocytes, B-cells and T-cells, are produced in the
bone marrow.
There is a network of small, bean-shaped structures called lymph
nodes or glands along the lymph vessels. Lymph nodes are found
throughout the body, including the neck, underarms, chest,
abdomen and groin. When lymph nodes become swollen, it is a
sign that your body is fighting infection. For example, glands in
your neck may swell when you have a sore throat.
Other parts of the lymphatic system include:
• spleen – contains lymphocytes, filters waste products from the
blood, and destroys old cells, abnormal cells and bacteria
• thymus – a gland where lymphocytes develop and mature
6 Cancer Council• tonsils – a collection of lymphatic tissue at the back of the
throat that traps inhaled or ingested germs
• bone marrow – the soft, spongy material inside bones that
makes three types of blood cells: red blood cells (carry oxygen);
white blood cells, including lymphocytes (fight infection); and
platelets (help the blood to clot).
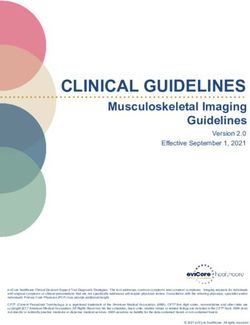
The lymphatic system
Tonsils
Thymus gland Lymph vessels
Underarm lymph nodes Diaphragm
Liver Spleen
Groin lymph nodes
The lymphatic system 7Key questions
Q: What is non-Hodgkin lymphoma?
A: Non-Hodgkin lymphoma is a type of lymphoma, which
is a general term for cancers that develop in lymphatic
tissue. Sometimes non-Hodgkin lymphoma is also called
non-Hodgkin’s lymphoma.
If you have non-Hodgkin lymphoma, your lymphocytes
become damaged. They grow abnormally and multiply
uncontrollably, causing your lymph nodes to enlarge and
form painless lumps called tumours. As the abnormal
lymphocytes replace the normal ones, your immune system
becomes less effective.
Non-Hodgkin lymphoma can occur in one lymph node,
a group of lymph nodes or another organ. The disease can
often be found in several parts of the body at the same time.
Q: What types are there?
A: There are many types of non-Hodgkin lymphoma. Several
different systems have been used to classify these types.
Non-Hodgkin lymphoma can be classified as slow growing
(low grade) or fast growing (high-grade). See pages 21–22.
More recent systems consider the type of cell affected
(B-cells or T-cells), the genetic make-up of the cells
(DNA chromosomes) and if certain proteins are
present. B-cell lymphomas make up about 85% of all
non-Hodgkin lymphomas.
8 Cancer CouncilB-cell types of lymphoma
diffuse large B-cell starts as a fast-growing lymph node tumour
cells tend to grow in circular groups of cells,
follicular
called follicles, in the lymph nodes
a slow-growing disease similar to chronic
small lymphocytic
lymphocytic leukaemia
affects the outer edge of B-cells in the lymph
mantle cell B-cell
node follicle, can grow quickly (aggressive)
T-cell types of lymphoma
often occur as widespread, enlarged, painless
peripheral T-cell
lymph nodes in the neck, armpit or groin
precursor can grow rapidly and interfere with breathing,
T-lymphoblastic so it needs to be diagnosed and treated quickly
Q: What are the causes?
A: In most cases, the cause of non-Hodgkin lymphoma is
unknown. Risk factors for developing the disease may include:
• immune system deficiency – caused by infection
such as human immunodeficiency virus (HIV), human
T-lymphotrophic virus (HTLV-1), herpes virus 8 or
Helicobacter pylori (H. pylori)
• autoimmune diseases – such as rheumatoid arthritis
• taking drugs that affect the immune system – some
people take immuno-suppressant drugs after an organ
transplant, for HIV or for an autoimmune disease.
Key questions 9Q: What are the symptoms?
A: Non-Hodgkin lymphoma may cause different symptoms
depending on where it is located in the body. These
symptoms may include:
• painless swelling of a lymph node (e.g. in the neck,
underarm or groin)
• unexplained and regular fevers
• excessive sweating, particularly at night
• unintentional weight loss
• persistent tiredness and lethargy
• itchy skin.
Sometimes lymphoma starts in lymph nodes in deeper parts
of the body, such as the abdomen (causing bloating) or the
chest (causing coughing, discomfort and difficulty breathing).
Symptoms of non-Hodgkin lymphoma are common to many
illnesses, such as the flu or a virus. If you are concerned,
make an appointment with your general practitioner (GP).
Q: How common is it?
A: About 4000 Australians are diagnosed with non-Hodgkin
lymphoma each year.
Most cases of non-Hodgkin lymphoma occur in adults aged
65 years and older. The risk of developing it increases as
you get older. However, it can also occur in children and
young adults.
10 Cancer CouncilDiagnosis
If your doctor suspects that you have lymphoma, you will have
a physical examination to check your lymph nodes for swelling.
Your doctor will examine your throat, tonsils, neck, abdomen,
underarms and groin. Most people also have a biopsy, blood count
and CT scan.
Biopsy
A diagnosis of lymphoma is made by removing the enlarged lymph
node, or part of it, and examining the cells under a microscope.
This is called a biopsy. It can be done in different ways:
• Excision biopsy – You will be given a local or general
anaesthetic, depending on the location of the lymph node. The
doctor will cut through the skin to remove the whole node, then
close the wound with temporary stitches. This is usually done
as an outpatient procedure. However, if the nodes are deep,
for example in the abdomen or chest, you may have to stay in
hospital longer, usually for a few days.
• Needle core biopsy – A needle is used to remove tissue
from the lymph node. You will be given a local anaesthetic
to numb the area. This procedure usually takes 30–60 minutes.
• Fine needle biopsy – A thin needle is inserted to remove a
small amount of tissue or fluid from the affected area/node in
your body. This type of biopsy is uncommon because it doesn’t
usually provide enough tissue for a full diagnosis. However, it
may help to determine if you need another type of biopsy.
Diagnosis 11Further tests
If the biopsy shows that you have non-Hodgkin lymphoma, you will
then usually have a few of the tests described on the following pages.
These tests will show whether cancer has spread to other parts of
your body. This is called staging – see page 17.
Blood tests
Your doctor will take a sample of your blood to check how your
kidney and liver are functioning. These organs may not work
properly if you have lymphoma.
Blood samples are also taken regularly during treatment to check
your blood counts, which is a measure of the different levels of
red blood cells, white blood cells and platelets. Low blood counts
may indicate the non-Hodgkin lymphoma has spread to the
bone marrow.
Blood cell levels and symptoms
can cause anaemia, which may
Low levels of
make you feel tired, breathless,
red blood cells
dizzy, and you may look pale
may make you more likely to get
Low levels of
infections and may make it more
white blood cells
difficult to get rid of infections
can cause you to bruise easily,
Low platelet levels get frequent nosebleeds or have
prolonged bleeding from cuts
12 Cancer CouncilBone marrow biopsy
This type of biopsy can show if there are any lymphoma cells in the
bone marrow. Your doctor will give you a local anaesthetic then
insert a needle into your pelvic bone to remove a small piece of bone
marrow. The needle is only inserted for a few seconds, but this may
be painful. Ask your doctor for pain-relief or sedation before the
procedure if it isn’t offered. The procedure takes about 30 minutes.
CT scan
The CT (computerised tomography) scan is a procedure that uses
x-ray beams to take pictures of the inside of your body. Unlike
a standard x-ray, which takes a single picture, a CT scan uses a
computer to compile pictures of different areas throughout your body.
This dye will make the scan pictures clearer, but it may make you
feel flushed or hot for a few minutes. Rarely, more serious reactions
occur, such as breathing difficulties or low blood pressure. Your
doctor will take the necessary measures to manage any side effects.
You need to lie still on a table while the large, round CT scanner
slowly rotates around you. You may be asked to hold your breath
for a few seconds or change position during the scan to help get
better pictures. This painless scan takes about 10–15 minutes, and
most people can go home as soon as it is finished.
The dye that is injected into your veins before a CT scan is called a
contrast solution and may contain iodine. If you are allergic to iodine,
fish or dyes, let the person performing the scan know in advance.
Diagnosis 13MRI scan
MRI (magnetic resonance imaging) is a less common scan used to
detect lymphoma. The MRI scan uses magnetism and radio waves
to create detailed cross-section pictures of the body. This scan
generally takes 30–60 minutes. If you have a pacemaker or another
type of metal object in your body, you cannot have an MRI scan.
You will lie in a narrow metal cylinder that is open at both ends. If
confined spaces make you feel claustrophobic or anxious, speak to
your health care team before the scan. They may give you a mild
sedative or arrange for you to speak through an intercom to the
person operating the machine during the procedure. The machine
is noisy during the scan.
PET scan
A positron emission tomography (PET) scan is a specialised
imaging test that is only available at some hospitals. PET scans
are only useful for some forms of lymphoma.
Before the scan, you will be injected with a radioactive glucose
(sugar) solution. You will be sedated or asked to sit quietly for
30–90 minutes while the glucose moves through your body. Your
body will then be scanned for high levels of radioactive glucose.
Active cells, such as cancer cells, have an increased uptake of this
solution and are highlighted in the scan.
It will take several hours to prepare for the scan and have it.
You may want to take a book to read or bring a friend for
company and support.
14 Cancer CouncilHeart scans
You might have one of the following scans to show how well your
heart pumps blood. This may be done before, during or after
chemotherapy treatment (see page 23).
• Echocardiogram – This is known as a cardiac ECHO or
cardiac ultrasound. A few small, sticky patches called electrodes
are placed on your chest, and gel is spread over the area. The
person performing the scan will use a small, paddle-shaped
device to create pictures of your heart. You may be asked to hold
your breath at times. This painless test can take up to an hour.
• Gated heart pool scan – A small amount of blood is taken,
mixed with radioactive material and re-injected into you. As
the radioactive material is pumped through your heart, it can
be seen on a computer screen. The scan takes about 45 minutes.
The radiation will leave your body within a few hours. Talk to
your doctor if you are concerned.
Tell your doctor if you are pregnant or breastfeeding. You may not
be able to have a gated heart pool scan.
Gallium scan
A gallium scan is an uncommon type of diagnostic test. A weak
radioactive substance (gallium) is injected into a vein in your
arm. Over 2–3 days, the gallium accumulates in areas of enlarged,
abnormal lymph nodes, showing where lymphoma has spread.
Diagnosis 15Lumbar puncture (spinal tap)
A lumbar puncture allows the doctor to examine the spinal fluid
to determine if the cancer has affected your central nervous
system. You will be given a local anaesthetic and a thin needle
will be inserted into your lower back to remove some fluid. This
may be done under x-ray guidance for people with spinal disease
or arthritis.
The lumbar puncture may be uncomfortable or painful. Tell
your doctor how you are feeling. Common side effects include
headaches and nausea, but these usually ease within a few hours.
Some people also have a chest x-ray to check for enlarged lymph
nodes in the chest. This is a painless scan.
Prognosis
Prognosis means the expected outcome of a disease. You may wish
to discuss your prognosis and treatment options with your doctor,
but it is not possible for any doctor to predict the exact course of
your disease. Instead, your doctor can advise you on common
issues that people with the same type of lymphoma experience.
While some people may be cured of non-Hodgkin lymphoma
after initial treatment, other people experience multiple episodes
(often called relapses) of the disease, going in and out of remission
(absence of disease symptoms) over several years.
16 Cancer CouncilStages of non-Hodgkin lymphoma
Staging describes how far the lymphoma has spread. Each stage is
also assigned a letter – for example, ‘A’ means you have no symptoms;
‘B’ means you have symptoms (e.g. fevers, night sweats).
Diaphragm Affected lymph Diaphragm
nodes
Stage 1 – One lymph node area Stage 2 – Two or more lymph node
is affected. This is either above or areas are affected, either above or
below the diaphragm muscle. below the diaphragm.
Diaphragm Lungs Diaphragm
Bone
Stage 3 – Lymph node areas Stage 4 – Lymphoma is in the
on both sides of the diaphragm lymph nodes and has also spread to
are affected. organs (e.g. liver, lungs) or to bones.
Diagnosis 17Which health professionals will I see?
Your GP may arrange the first tests to assess your symptoms.
If these tests do not rule out cancer, you will usually be referred
to a haematologist who will arrange further tests and advise you
about treatment options.
I trust my haematologist, she is very honest with me and it
makes me feel secure in my choices. Andrea
Specialist health professionals
specialises in diagnosing and treating
haematologist diseases of the blood, the lymphatic system
and bone marrow
prescribes and coordinates the course
radiation oncologist
of radiotherapy
prescribes and coordinates the course
medical oncologist
of chemotherapy
help administer drugs, including chemotherapy,
nurses and provide care, information and support
throughout your treatment
18 Cancer CouncilA haematologist typically diagnoses and treats the lymphoma,
often with chemotherapy and biological therapy. However,
sometimes a medical oncologist may oversee your treatment
for lymphoma.
You will probably be cared for by a range of health professionals
who specialise in different aspects of your treatment. This
multidisciplinary (MDT) team may include:
a nurse who supports patients and
cancer care coordinator families throughout treatment and
liaises with other staff
recommends an eating plan for you
dietitian to follow while you are in treatment
and recovery
dispenses medications and can give
pharmacist you advice about drugs, dosage and
side effects
social worker, physiotherapist, link you to support services and help
clinical psychologist and you with any emotional, physical or
occupational therapist practical problems
Diagnosis 19Key points
• Your GP will carry out a • Other diagnostic tests may
physical examination if include CT, MRI and PET scans.
lymphoma is suspected. Most
people will then have a biopsy, • A gated heart pool scan or
blood count and CT scan to echocardiogram may be done
confirm the diagnosis. to find out how well your heart
is working.
• A biopsy is done by removing
the affected lymph node, or • The doctor may also
part of it, and examining it recommend a lumbar puncture
under a microscope. to check if the cancer has
affected your central nervous
• After the diagnosis is system. This may be painful.
confirmed, you will have
further tests to work out how • Your GP will refer you to a
far the lymphoma has spread. haematologist who can tell you
how far the cancer has spread.
• Blood tests can check how This is called staging.
your liver and kidneys are
working. These may also • Your doctor may talk with you
involve checking the number about your prognosis. This is a
of red blood cells, white blood general prediction of what may
cells and platelets. happen to you.
• You may need a bone marrow • Some people with non-Hodgkin
biopsy. This is when a needle lymphoma are cured after
is inserted into the bone and initial treatment, but others
marrow is withdrawn. This can experience multiple episodes
be painful. during their lifetime.
20 Cancer CouncilTreatment
Treatment options for people with non-Hodgkin lymphoma vary.
When planning your treatment, your doctor will look at a number
of factors. This includes:
• the type of lymphoma you have (e.g. low-grade lymphoma or
aggressive lymphoma)
• which parts of your body are affected
• your age and general health.
The aim of treatment is to control the lymphoma so that you go
into remission. This is when the symptoms and signs of cancer
reduce or disappear, and tests become normal or near normal.
Remission may last for a long period of time, until the lymphoma
becomes active again and treatment is required. This pattern of
remission and relapse may repeat several times.
Low-grade (indolent) lymphoma
Some lymphoma, called low-grade or indolent lymphoma, grows
very slowly and causes few problems. This is because there is little
change in the disease over time.
Your doctor may decide that you don’t need treatment initially, but
will monitor your health with regular check-ups and blood tests.
This is called watchful waiting or watch and wait.
If there is a change or growth in the lymphoma that causes
symptoms, and other warning signs appear, your doctor will
recommend treatment. The treatment is usually chemotherapy but
can include radiotherapy and biological therapies.
Treatment 21Understanding watchful waiting
You may not have treatment Treating the lymphoma earlier
straightaway, but instead have than necessary can cause
regular check-ups to monitor unpleasant side effects. It can
the cancer, known as watchful also make your body resistant
waiting. Some people find this to treatment, so if you need it
approach difficult to accept. later, it may not work as well.
You might prefer to have
treatment right away. If you feel uncomfortable with
this watch and wait approach,
Although many people who speak with your medical team.
have other types of cancer Many people with untreated
have immediate treatment, low-grade lymphoma continue
doctors recommend watchful their usual daily activities for
waiting for low-grade many years. Your doctor may
lymphoma. Results from clinical be able to put you in touch with
studies have proven that there another patient who has had
is no advantage to giving a similar experience and can
treatment at an early stage. explain how they’ve coped.
High-grade (aggressive) lymphoma
High-grade or aggressive lymphoma grows much faster than
low-grade lymphoma and needs treatment as soon as possible.
The aim is to stop the active disease and cause remission.
Chemotherapy is the main treatment for high-grade lymphoma.
You may be given chemotherapy initially, then also have one or
more other types of treatment. This may include radiotherapy,
a stem cell transplant or biological therapies.
22 Cancer CouncilChemotherapy
Chemotherapy is the use of drugs to kill or slow the growth
of cancer cells. Treatment is usually given as a combination of
drugs. Chemotherapy is often combined with other treatments,
such as monoclonal antibodies or steroid therapy (see pages 26–29),
or given as a palliative treatment (see page 35).
Chemotherapy can be given in tablet form or injected into your
veins (intravenously). Intravenous treatment can be given through
a drip or a device called a tube or a line.
Types of intravenous lines
A thin tube that can stay in place for a
PICC (Peripherally
long period of time, inserted into one of
inserted central catheter)
the main veins in your arm.
A thin tube with a dome-shaped opening
(port) that is surgically inserted into a
vein in your chest or arm. Needles are
Port-a-cath (port)
used to access the port-a-cath when it is
required for treatment. It must be flushed
regularly when not in use.
A thin tube with several openings
Central line (Central
(lumens) that is inserted into a vein in
venous catheter or CVC)
your neck or chest.
A small hollow plastic tube put into your
Cannula
hand or arm.
Treatment 23Occasionally, a small amount of chemotherapy is given via a
lumbar puncture (see page 16). This is called intrathecal
chemotherapy, and it is done to prevent or treat lymphoma in
the brain or spinal cord.
Many people have chemotherapy as an outpatient, although at
times you may need a short stay in hospital. You will be closely
monitored by your doctor after each course of treatment, and have
further tests to see how the drugs have affected the lymphoma.
Chemotherapy treatment may be repeated several times until the
lymphoma goes into remission.
Side effects
Chemotherapy drugs can harm healthy, fast-growing cells, such as
the cells in your hair, mouth and blood. This can cause side effects
such as hair loss, mouth sores, nausea and tiredness.
Side effects can make it hard for you to function as usual. Although
many people continue to work and carry out their daily activities
while having chemotherapy, you may need extra rest when you feel
tired. Discuss any side effects you experience with your doctor or
nurses. Most side effects are temporary, and your medical team
can give you medication to help relieve symptoms.
Tell your doctor about any medicines, herbal remedies, antioxidants
or nutritional supplements you’re taking, as these may affect how
chemotherapy works in your body.
24 Cancer CouncilTaking care with infections
People being treated for Contact your doctor or go to
lymphoma are more prone to the nearest hospital emergency
infections, particularly when department immediately if you
they are having chemotherapy. experience:
This is because chemotherapy • a fever over 38ºC (keep a
reduces your white blood cell thermometer handy to check
levels, making it harder for your temperature)
your body to fight infections.
Colds and flu may linger,
• chills or constant shivering
and scratches and cuts may • sweating, especially at night
become infected easily.
• a burning feeling when
urinating
Some people try to avoid
crowded public places where • a severe cough or
they could catch a cold or flu. sore throat
Ask relatives or friends with
a cold or the flu to wait until
• vomiting that lasts more than
a few hours
they are well before visiting.
Naturally, this is not practical • unusual bruising or bleeding,
for the people you live with, such as nosebleeds, blood
so use your common sense in your urine or black
and try to avoid close contact bowel motions
if they are ill.
• infections at the site of
your injections
See your doctor if you are
unwell during chemotherapy, • prolonged faintness
particularly if you have a cold, or dizziness and a
as this can become a serious rapid heartbeat.
health problem.
Treatment 25Biological therapies
Biological therapies (also called biotherapies) include a range of
treatments derived from natural substances in the body, usually
proteins. They are converted for use as medications. The therapies
work in different ways to help the body fight cancer:
Monoclonal antibodies – These are man-made versions
of immune system proteins called antibodies. They work by
targeting diseased cells, attaching to them and then helping the
body’s immune system destroy them. This medication is given
intravenously, and is used alone or with other treatments.
Monoclonal antibodies available in Australia for lymphoma
include rituximab (Mabthera®) and alemtuzumab (Campath®).
One of these drugs may be used as a first treatment or combined
with chemotherapy (see page 23).
Immunotherapy – Strengthens the immune system so that it is
able to find and attack cancer cells more effectively. One treatment
is interferon, a hormone-like protein made by white blood cells
that is injected under the skin. Vaccines can also be given to make
your body produce antibodies to fight the lymphoma.
Some types of immunotherapy are used to make the main
treatment more effective. This is called adjuvant therapy.
Granulocyte-colony stimulating factor (G-CSF) – Helps white
blood cells recover faster following chemotherapy. This is given as
an injection under the skin (subcutaneously).
26 Cancer CouncilG-CSF is also sometimes used in stem cell transplants to help
blood stem cells multiply quickly (see page 30). It can also be
given after chemotherapy has finished.
Side effects
Side effects are specific to the medication used. They are very
uncommon with some types of medication (e.g. G-CSF) but more
common with others (e.g. interferon). Talk to your doctor about
what may occur.
Arrange to go to the hospital with a relative or friend if you can.
You may feel unwell and weak following treatment, so it is helpful if
someone can take you home.
Radiotherapy
Radiotherapy uses x-rays to kill cancer cells or harm them so
they cannot multiply. It is generally used for stage 1 or stage 2
lymphoma when there are lymphoma cells in one or two areas
of lymph nodes in a part of the body. If the lymphoma is more
advanced or high-grade, you may have radiotherapy combined
with chemotherapy (chemoradiotherapy).
A course of radiotherapy is usually given daily over several weeks.
Each session lasts for a few minutes, but it can take longer to
wait for your appointment and set up the equipment. The overall
course of treatment will depend on the type of non-Hodgkin
lymphoma you have and your general health.
Treatment 27Radiotherapy is painless and you should not feel any discomfort
during each session. While you are being treated, you will lie alone
in a room under a large machine that delivers x-ray beams to the
treatment area. You will be able to talk to the radiation therapist
through an intercom.
Radioimmunotherapy
This is a type of high-power This treatment may cause
targeted radiotherapy that side effects such as nausea or
uses monoclonal antibodies tiredness. It is not commonly
(see page 26) to deliver used in Australia and is only
radiation to cancer cells. It available at a limited number
is also known as radioactive of treatment centres.
antibody treatment.
Side effects
Radiotherapy often causes side effects, such as tiredness and local
skin irritation. Most side effects are temporary and your doctor
can prescribe medication to reduce any discomfort.
Other side effects depend on the part of your body being treated.
For example, radiotherapy to the abdomen may cause an upset
stomach, nausea, diarrhoea and infertility.
Radiotherapy to the neck can affect your sense of taste and make
your mouth sore and dry. For more details on what side effects
you may experience, talk with your doctor or call Cancer Council
Helpline 13 11 20 for a free copy of Understanding Radiotherapy.
28 Cancer CouncilSteroid therapy
Steroids are made naturally in the body, but they can also be
produced artificially and used as drugs.
Corticosteroids are a type of steroid often given with
chemotherapy to make the treatment more effective.
Side effects
People having steroid therapy may have various side effects,
depending on the dose and how long they have treatment. Most
side effects are temporary and will gradually disappear after you
stop taking the medication.
If you have steroids for a short amount of time, your symptoms
may include:
• an increased appetite
• feelings of restlessness
• insomnia
• weight gain.
If taken for several months, steroids can also cause fluid retention,
high blood pressure, high blood glucose levels and diabetes. You
will be more likely to get infections and, over time, your skin,
muscles and bones may weaken.
Your medical team will monitor you during steroid treatment.
Tell your doctor or nurse if you have any uncomfortable or
unpleasant side effects. There are ways to reduce the side effects
you experience.
Treatment 29Peripheral blood stem cell transplant
A peripheral blood stem cell transplant may be an option if
the lymphoma returns (relapses) or does not respond to
standard therapy.
Stem cells are immature cells from which blood cells develop.
Most stem cells are found in the bone marrow, but a small
number are also found in your blood. These are called peripheral
blood stem cells.
The general transplant process is described here, but procedures
vary from person to person based on their circumstances. Talk to
your health care team about what to expect, including how long you
will be in hospital. There are two types of transplants you may have:
• autologous transplant – your own stem cells are extracted
from your body, frozen and injected back into your body after
further chemotherapy
• allogeneic transplant – stem cells are collected from another
person – a matched donor, usually a family member or a volunteer
donor – and injected into your body after chemotherapy.
For detailed information about transplants, contact the Leukaemia
Foundation on 1800 620 420 or www.leukaemia.org.au. For
more information about stem cell harvesting, visit the Lymphoma
Australia website at www.lymphoma.org.au.
30 Cancer CouncilIt is important to have a dental check-up and have any problems
fixed before a transplant, as the mouth is a major source of
bacteria. If left untreated, mouth problems can cause infections
after the transplant.
If your own stem cells are used (autologous transplant), you will
usually be given granulocyte-colony stimulating factor (G-CSF)
before the transplant to help the stem cells multiply as quickly as
possible. These stem cells are released from the bone marrow into
the blood.
Once there are enough stem cells in your bloodstream they will
be collected in a cell separating machine. This process is called
apheresis. The patient usually has two needles inserted, one in
each arm. One needle is used to draw the cells away into the
machine and the other needle is used to return the blood cells
to the body. The machine separates the blood into different
components. The stem-cell rich white blood cell layer is collected
while the other blood cells are returned to the patient.
Apheresis is a continuous process and can take several hours. Once
there are enough stem cells collected, they are frozen and stored
until needed. This process is referred to as a stem cell harvest.
Sometime after your stem cells have been collected, you will be
given high-dose chemotherapy to kill any remaining lymphoma
cells. The drugs will also destroy your own blood-forming cells in
the bone marrow, which can cause side effects (see page 24).
Treatment 31A day or so after the high-dose chemotherapy, your stem cells will
be thawed and returned to you intravenously (see page 23). These
healthy stem cells help to restore your bone marrow. You may
have blood and platelet transfusions in the lead up to and during
your transplant.
Side effects
High-dose chemotherapy, and the transplant itself, can cause
serious, life-threatening side effects. Your doctor will talk to
you about this before the transplant. You may also have some
temporary side effects, including:
• fatigue
• nausea, vomiting and diarrhoea
• mouth ulcers
• hair loss
• low blood counts (e.g. increased risk of infections).
After the transplant, you will probably continue to have side effects
caused by chemotherapy, including fatigue. Your blood counts may
remain low for a while. Over time, these symptoms will go away.
For more information about coping with side effects, call Cancer
Council Helpline 13 11 20.
Some people have their stem cells collected directly from the bone
marrow by suction (aspiration) under general anaesthetic. This is
called a bone marrow harvest. This is not as common as peripheral
blood stem cell harvesting.
32 Cancer CouncilRecycling stem cells
1. First, a drug
helps the stem cells
2. Several days
multiply and release
later, some blood
into the blood.
is taken out.
This cycle occurs over a few
months and with breaks.
6. The stem 3. The stem
cells are cells are
N
thawed and separated
returned via using a
a vein. machine.
4. They are then
5. High-dose processed
chemotherapy is and frozen.
given to the patient.
This is a simplified overview of the transplant process. Your case may be different.
Treatment 33Graft-versus-host disease
If you have had an allogeneic This can cause problems in
transplant, you may develop many of your organs, such as
graft-versus-host disease your liver and lungs. After the
(GVHD). In GVHD, the donor’s transplant, your doctor will
cells in the transplanted tissue monitor you for GVHD, and if it
(the graft) attack your own occurs, prescribe medications
body tissue (the host). to control it.
Recovery after a transplant
When your blood counts have risen and your general health
improves, you can go home, but you will need regular follow-up
care, such as blood tests, to check your progress. You may still
need to have blood or platelet transfusions. These tests are usually
done as an outpatient.
While your immunity is low, you may have to regularly take
medications to reduce the risk of infection. It is not uncommon to
become unwell after treatment and have to go back into hospital.
Before leaving the hospital, ask your doctor if there is a contact
number you can have in case you become unwell.
The time it takes to recover varies depending on your situation.
Your health care team, including your doctor, nurses and
pharmacist, will all be able to discuss with you what you might
expect while you recuperate. You can also call the Helpline for
support and advice.
34 Cancer CouncilPalliative treatment
Palliative treatment helps to improve a person’s quality of life by
alleviating symptoms of cancer without trying to cure the disease.
It is particularly important for people with advanced cancer.
However, it is not just for end-of-life care and it can be used at
different stages of cancer.
Often treatment is focused on pain relief, but it can involve
the management of other physical and emotional symptoms.
Treatment may include radiotherapy, chemotherapy, blood
transfusions and medication.
Call Cancer Council Helpline 13 11 20 for more information on
palliative treatment and advanced cancer.
Mum has called her treatments palliative from day
one because they give her relief from the pain and stress
of having a serious illness. Her palliative care team provide
that extra layer of support. Jackie
Treatment 35Key points
• Your doctor will recommend • Chemotherapy side effects,
your treatment after such as hair loss, mouth sores,
considering the type of nausea and tiredness, can be
lymphoma you have, which managed. Talk to your doctor
parts of your body are and nurses.
affected, your age and health.
• Radiotherapy uses x-rays to
• Low-grade (indolent) kill cancer cells or injure them
lymphoma grows very slowly so they cannot multiply. Side
and causes few symptoms. effects depend on the area of
Most people with this type your body that is treated.
of lymphoma do not have
treatment right away. This is • Biological therapies and
called watchful waiting. steroid therapies often
complement other treatments,
• High-grade (aggressive) such as chemotherapy.
lymphoma grows quickly and
needs immediate treatment. • A peripheral blood stem cell
transplant may be an option
• The main treatment for if the lymphoma returns or
high-grade lymphoma is does not respond to usual
chemotherapy. The aim is to treatment. A transplant and
stop the active disease and chemotherapy can cause
cause remission. serious side effects.
• Chemotherapy (drug • Palliative treatment may be
treatment) can be given in given to relieve the symptoms
different forms, including of lymphoma without trying to
a tablet or injection into your cure the disease.
veins (intravenously).
36 Cancer CouncilMaking treatment
decisions
Sometimes it is difficult to decide on the right treatment. You may
feel that everything is happening so fast you don’t have time to
think things through. If you are feeling unsure about your options,
check with your doctor how soon your treatment should start, and
take as much time as you can before making a decision.
Understanding details about the disease, the available treatments
and their possible side effects will help you make a well-informed
decision. This decision will also take into account your personal
values and the things that are important to you and your family.
It is common to feel overwhelmed by information so it may help if
you read and talk about the cancer gradually.
• Weigh up the advantages and disadvantages of different
treatments, including the impact of any side effects.
• If only one type of treatment is recommended, ask your doctor
why other choices have not been offered.
• If you have a partner, you may want to discuss the treatment
options together. You can also talk to friends and family.
You have the right to accept or refuse any treatment offered by
your doctors and other health care professionals. Some people
with advanced cancer choose treatment even if it only offers a
small benefit for a short period of time. Others want to make sure
the benefits outweigh the side effects so that they have the best
possible quality of life. Some people choose options that focus on
reducing symptoms and make them feel as well as possible.
Making treatment decisions 37Talking with doctors
When your doctor first tells you that you have lymphoma you may
not remember all the details about what you are told. You may
want to see the doctor again before deciding on treatment. Ask for
the time and support to make your decision.
If you have questions, it may help to write them down before you
see the doctor. You can also check the list of suggested questions
on page 53. Taking notes or recording the discussion can help too.
Many people like to have a family member or friend go with them
to take part in the discussion, take notes or simply listen.
If your doctor uses medical terms you don’t understand, ask for
an explanation in everyday language. You can also check a word’s
meaning in the glossary (see page 54).
If you have several questions for your doctor, ask if it is possible to
book a longer appointment.
A second opinion
Getting a second opinion from another specialist may be a
valuable part of your decision-making process. It can confirm or
clarify your doctor’s recommendations and reassure you that you
have explored all of your options.
Some people feel uncomfortable asking their doctor for a second
opinion, but specialists are used to people doing this.
38 Cancer CouncilYour doctor can refer you to another specialist and send your
initial results to that person. You can get a second opinion even
if you have started treatment or still want to be treated by your
first doctor. Alternatively, you may decide you would prefer to be
treated by the doctor who provided the second opinion.
Taking part in a clinical trial
Your doctor may suggest you consider taking part in a clinical
trial. Doctors run clinical trials to test new or modified treatments
and ways of diagnosing disease to see if they are better than
current methods. Over the years, trials have improved treatments
and led to better outcomes for people diagnosed with cancer.
If you join what is called a randomised trial for a new treatment,
you will be chosen at random to receive either the best existing
treatment or the promising new treatment.
To help you decide whether or not to participate, you can talk to
your specialist or the clinical trials nurse. If you’re still unsure, you
can also ask for a second opinion from an independent specialist.
If you do decide to take part, you have the right to withdraw from
the trial at any time; doing so will not jeopardise your ongoing
treatment for cancer.
For more information about clinical trials and other research,
including questions to ask your doctor and how to find a suitable
study, call Cancer Council Helpline 13 11 20. You can also find
trials on the website, www.australiancancertrials.gov.au.
Making treatment decisions 39Looking after yourself
Cancer can cause physical and emotional strain. It can also impact
on your body image, relationships and outlook for the future.
It’s important to take time to look after yourself by eating well,
exercising, reducing stress and improving your wellbeing.
Healthy eating
Eating nutritious food will help you keep as well as possible and
cope with cancer and treatment side effects. Depending on your
treatment, you may have special dietary needs. A hospital dietitian
can help you manage any eating difficulties and choose the best
foods and meals for your situation. Cancer Council Helpline can
send you free information about nutrition and cancer.
Being active
Research shows it is helpful to stay active and exercise regularly
if you can. Physical activity, even if gentle or for a short duration,
helps to improve circulation, reduce tiredness and elevate mood.
The amount and type of exercise you do will depend on what you
are used to, how well you feel and what your doctor advises. If you
aren’t used to exercise or haven’t exercised for a while, make small
changes to your daily activities. You could walk to the shops, take
the stairs, do some gardening or join a gentle exercise class.
If you want to do more vigorous or weight-bearing exercise, ask
your medical team what is best for you. Cancer Council Helpline
can send you free information about exercise and cancer.
40 Cancer CouncilComplementary therapies
Complementary therapies are treatments that may help you cope
better with side effects such as pain. They may also increase your
sense of control over what is happening to you, decrease your
stress and anxiety, and improve your mood.
There are many types of complementary therapies, such as herbal
medicine, acupuncture, massage, relaxation and meditation. Some
treatment centres offer these therapies as part of their services,
but you may have to go to a private practitioner. Self-help CDs or
DVDs can also guide you through different techniques.
Let your doctor know about any complementary therapies you
are using or thinking about trying. Some therapies may not be
appropriate, depending on your medical treatment. For example,
herbs and nutritional supplements may interact with your
medication or surgery, resulting in harmful side effects. Massage,
acupuncture and exercise therapies should also be modified if you
have lowered immunity, low platelets or fragile bones.
Call the Helpline on 13 11 20 for more information and resources
about complementary therapies.
Alternative therapies are commonly defined as those used instead
of conventional treatments. These therapies may be harmful if
people with cancer delay or stop using conventional treatment in
favour of them. Examples are coffee enemas and magnet therapy.
Looking after yourself 41Relationships with others
For many people, the experience of having cancer and any
ongoing challenges causes them to make some changes in their
life. You may also have a new outlook on your values, priorities,
or life in general. Some people find that these changes can affect
their relationships. However, sharing your thoughts and feelings
with family, friends and colleagues may help to strengthen your
relationships with them.
If you feel uncomfortable talking about your feelings, take your
time and approach others when you are ready. People usually
appreciate insight into how you are feeling and guidance on
providing support during and after treatment. Calling Cancer
Council Helpline may help you build your confidence to discuss
your feelings with others.
Give yourself time to adjust to your cancer diagnosis, and do the
same for friends and family. People often react in different ways,
for example being overly positive, playing down fears, or keeping a
distance. They are also dealing with the diagnosis and the changes.
If someone’s behaviour upsets you, it might help to discuss how
you both feel about the situation.
The whole time I was on chemotherapy and radiotherapy,
my friend called me every day between 8am and 9am. She
could hear if I was well by my voice. There aren’t many friends
like that around. Meg
42 Cancer CouncilSexuality, intimacy and cancer
Having cancer can affect your sexuality in physical and emotional
ways. The impact of these changes depends on many factors,
such as treatment and side effects, the way you and your partner
communicate, and your self-confidence. Knowing the potential
challenges and addressing them will help you adjust to these changes.
Some people with cancer have the support of a partner, while others
do not. If you meet a new partner during or after treatment, it can be
difficult to talk about your experiences, particularly if the cancer has
had an impact on your sexuality.
Sexual intercourse may not always be possible during and
immediately after treatment, but closeness and sharing are vital to a
healthy relationship. Call Cancer Council Helpline 13 11 20 for more
information on sexuality and cancer.
Some treatments may affect your fertility permanently or
temporarily. If having children is important to you, talk to your
doctor before you start treatment.
Contraception
Depending on the type of cancer and treatment you have, your
doctors may advise you to use certain types of contraception, such
as condoms, during and after treatment. This is to protect your
partner and also to avoid pregnancy, as some treatments, such as
chemotherapy, can be harmful to your partner and can harm a
developing baby. Ask your doctors what precautions to take.
Looking after yourself 43You can also read