Role of microRNAs in fluoropyrimidine-related toxicity: what we know
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
European Review for Medical and Pharmacological Sciences 2021; 25: 3306-3315
Role of microRNAs in fluoropyrimidine-related
toxicity: what we know
A.L. DEAC1, C.C. BURZ1,2, C. MILITARU3, I.C. BOCȘAN3, R.M. POP3,
P. ACHIMAȘ-CADARIU1,4, A.D. BUZOIANU3
1
“Prof. Dr. Ion Chiricuţă” Oncology Institute, Cluj-Napoca, Romania
2
Department of Immunology and Allergology, Faculty of Medicine, “Iuliu Haţieganu” University of
Medicine and Pharmacy, Cluj-Napoca, Romania
3
Department of Pharmacology, Toxicology and Clinical Pharmacology, Faculty of Medicine, “Iuliu
Hațieganu” University of Medicine and Pharmacy, Cluj-Napoca, Romania
4
Department of Surgery, Faculty of Medicine, “Iuliu Haţieganu” University of Medicine and
Pharmacy, Cluj-Napoca, Romania
Abstract. – Although more than half a cen- used in Asia, and TAS-102 is used in subsequent
tury has passed since the discovery of fluoro- treatment lines upon the failure of classical fluo-
pyrimidines, they are still used in the treatment ropyrimidines and targeted therapy.
of many types of cancer, and it is estimated that
annually two million patients undergo fluoropy-
The prodrugs Capecitabine, TAS-102, S-1, and
rimidine-based chemotherapy. The toxicity re- Tegafur are converted to 5-FU, which is sub-
sulting from the use of fluoropyrimidines affects sequently activated in several steps to FdUMP
about 30-40% of patients, which in some cases (fluorodeoxyuridine monophosphate), which is an
may prove to be lethal. The key player in fluoro- inhibitor of TS (thymidylate synthase)1,2. TS inhi-
pyrimidine toxicity is DPD activity, and patients bition leads to the depletion of dTMP (deoxythy-
with deficits are more likely to develop signifi-
midine monophosphate) but an accumulation of
cant adverse events. In addition to genotyping
DPYD variants associated with DPD deficiency, dUMP (deoxyuridine monophosphate). FdUMP
overexpression of miR-27 has also been shown and dUMP can be phosphorylated to FdUTP
to be a predictive factor for fluoropyrimidine tox- (fluorodeoxyuridine triphosphate) and dUTP (de-
icity. This review aims to relate what we know so oxyuridine triphosphate), respectively, and incor-
far about the involvement of miRNA in fluoropy- porated into DNA1,2. TAS-102 is the combination
rimidine toxicity and to open new perspectives of TFT (trifluridine) and TPI (tipiracil hydrochlo-
in this field.
ride). TFT can be phosphorylated to TF-thymine,
Key Words: which can be inhibited by TPI. TFT is phosphor-
Fluoropyrimidine, Chemotherapy, Toxicity, Pharma- ylated to TFT-MP (trifluridine-monophosphate),
cogenetics. which is a reversible inhibitor of TS, while upon
phosphorylation to TFT-TP (trifluridine-triphos-
phate), it can also be incorporated into DNA.
Substitution of dTTP (deoxythymidine triphos-
Introduction phate) by either TFT-TP or dUTP or FdUTP leads
to DNA damage and cell death3.
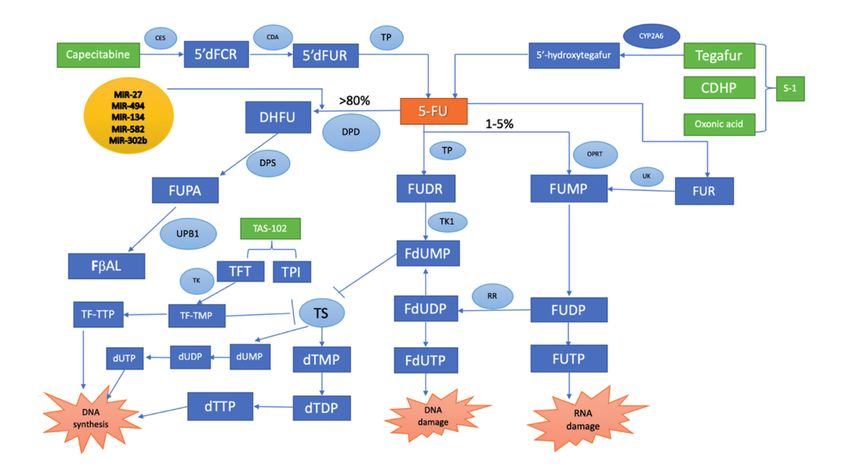
Fluoropyrimidines are antimetabolite drugs Capecitabine and Tegafur are converted to
widely used in the treatment of head and neck 5-FU by thymidine-phosphorylase (TP) and
cancer, breast cancer, esophageal cancer, gastric CYP2A6. 1-5% of 5-FU is transformed into
cancer, pancreatic cancer, hepatobiliary cancer, cytotoxic metabolites FdUMP, FdUDP (fluoro-
colorectal cancer, anal cancer, and vulvar cancer1. deoxyuridine diphosphate), FdUTP and FUTP
The fluoropyrimidines used in clinical practice (fluorouridine triphosphate)1,2. 5-FU is directly
are 5-fluorouracil (5-FU), Capecitabine, Tega- transformed to FUMP (fluoridine monophos-
fur, S-1 (tegafur/gimeracil/oteracil), and TAS-102 phate) by OPRT (orotate phosphoribosyltrans-
(trifluridine/tipiracil). 5-FU and its oral prod- ferase) or indirectly through FUR (fluorouri-
rug, Capecitabine, are the most commonly used dine) by UP (uridine phosphorylase) and UK
fluoropyrimidines, Tegafur and S-1 are mostly (uridine kinase). FUMP is then phosphorylated
3306 Corresponding Author: Andrada Larisa Deac, MD; e-mail: andrada.deac@gmail.comRole of microRNAs in fluoropyrimidine-related toxicity: what we know
to FUDP (fluorouridine diphosphate), which is variants in the gene encoding DPD (DPYD) are
phosphorylated to FUTP. FUDP can also be known to be related to severe and lethal fluoropy-
converted to FdUDP by ribonucleotide reduc- rimidine toxicity5.
tase (RR)1,2. In an alternative activation path- Not all severe fluoropyrimidine adverse events
way, 5-FU is converted to FUDR (fluorodeoxy- can be explained by DPYD variants; sometimes,
uridine) by thymidine phosphorylase. FUDR carriers of a DPYD variant associated with an
is converted through thymidine phosphate in increased risk of severe adverse events may toler-
FdUMP, which is phosphorylated to FdUDP, ate well the treatment with fluoropyrimidine and
which is phosphorylated to FdUTP. Eighty per- may not experience major toxicity6. As such, the
cent of the 5-FU is catabolized by dihydropy- intervention of other factors capable of affecting
rimidine dehydrogenase into the non-cytotoxic DPYD expression may influence fluoropyrimi-
metabolites DHFU (5-fluoro-5,6-dihydroura- dine metabolism in patients both with and with-
cil), which is then converted to FUPA (flu- out DPYD variants.
oro-beta-ureidopropionate) and FUBA (fluo- MicroRNAs (miRNAs) are endogenous, short
ro-beta-alanine), which are eliminated through non-coding RNA molecules, about 20-22 nucleo-
urine. To modulate the activity of fluoropyrim- tides in length, which are found in all eukaryotic
idines, inhibitors of DPD can be administrat- cells and assist in regulating post-transcription-
ed, which slow the degradation of 5-FU and al gene expression by binding to 3’untranslated
improve the response rate1,2 (Figure 1). regions or 5’untranslated regions of target mes-
The rate-limiting enzyme of 5-FU catabo- senger RNAs. This also leads to the inhibition
lism is dihydropyrimidine dehydrogenase (DPD), of translation of messenger RNA degradation7,8.
which metabolizes almost 80% of the dose of Almost 30% of human genome proteins are regu-
5-FU and Capecitabine4. DPD is the essential en- lated by miRNAs, with half of these genes being
zyme for the 5-fluorouracil catabolism, and there- associated with cancer7,8. MicroRNAs regulate
fore the amount of 5-FU converted in cytotoxic the gene expression involved in essential biolog-
metabolites depends on the systemic activity of ical processes such as cell proliferation, cell dif-
DPD4. Some of the severe side effects that occur ferentiation, apoptosis, metastasis, and immune
during fluoropyrimidine treatment are due to response9-11. Many studies have tried to prove that
metabolism through the DPD. Deleterious genetic miRNAs can be used as diagnostic tools, predic-
Figure 1. Fluoropyrimidine metabolic pathways
3307A.L. Deac, C.C. Burz, C. Militaru, I.C. Bocșan, R.M. Pop, P. Achimaș-Cadariu, A.D. Buzoianu
tive biomarkers of disease progression, prognos- elosuppression, severe diarrhea, and rare events
tic biomarkers, survival rate, progression-free such as acute cardiac ischemia following the first
survival, treatment responsiveness, and chemo- or second cycle of 5-FU, hepatitis, and encepha-
therapy-related toxicity12-14. The importance of lopathy22.
microRNAs regarding chemotherapy toxicity is DPD expression varies from tissue to tissue
less well known. and exerts its activity predominantly in the liver,
In our review, we summarize the role of miR- peripheral blood mononuclear cells, and inflam-
NAs in fluoropyrimidine toxicity, the relation matory and tumor tissues.
with DPD, and how miRNAs may be a tool in The DPD activity is also influenced by the
selecting patients who will benefit from the ef- circadian rhythm, which DPD activity follows:
ficacy of fluoropyrimidines without developing DPD activity peaks near midnight, and through
major toxicities. DPD activity in the early afternoon; this was dis-
covered during the administration of continuous
Fluoropyrimidine-Related Toxicity 5-FU infusions23.
Severe toxicity in chemotherapy is usually as- The activity of DPD has high interindividual
sociated with interruption or treatment discontin- variability, but the most important are variants of
uation and often requires hospitalization. Fluoro- the DPYD gene, the gene that encodes the DPD
pyrimidine-related toxicity is a well-recognized enzyme24.
clinical problem that impacts patients’ quality of The DPYD gene allelic variants most fre-
life and, in some cases, can be life-threatening. quently associated with toxicity during the
5-FU and Capecitabine can induce grade 3 or treatment with fluoropyrimidine are DPY-
4 toxicity in 10-30% of patients and fatal tox- D*2A (IVS14+1G>A, c.1905+1G>A), DPYD*9B
icity in 0.3-2% of patients15. When we compare (c.2846A>T), DPYD*13 (c.1679T>G), HapB3
5-FU to Capecitabine, data from the Adverse (c.1129-5923C>G)24-28.
Event Reporting System (AERS) of the Food In addition to DPYD gene polymorphisms,
and Drug Administration (FDA) have shown polymorphisms of other genes such as thymi-
that certain side effects are more common for dylate synthase (TYMS), methylenetetrahydro-
one or the other, such as myelosuppression has folate reductase (MHTFR), enolase superfami-
been shown to be more common in patients ly member 1 (ENOSF1), ATP-binding cassette
receiving 5-FU and diarrhea or hand-foot syn- subfamily B member 1 (ABCB1), and cytidine
drome in patients receiving Capecitabine16. The deaminase (CDA) appear to be involved in fluo-
lower prevalence of adverse effects of S-1 and ropyrimidine toxicity29-34.
TAS-102, compared to 5-FU and Capecitabine, Fluoropyrimidine toxicity, especially of 5-flu-
is due to them carrying a DPD inhibitor in their orouracil, can be manifested through hemato-
composition, which increases the bioavailabil- logical non-cumulative toxicity most common in
ity of 5-FU3. bolus infusion (neutropenia, thrombocytopenia,
5-FU has a narrow therapeutic index; there- anemia), immediate digestive toxicity (nausea,
fore, there is a small limitation between efficacy vomiting, diarrhea, stomatitis, ileitis), alopecia
and toxicity17. Adverse events are likely the re- in case of continuous perfusion, thrombophlebi-
sults of genetic variation, especially ones such tis and photosensitivity along the vein pathway,
as DPD. Decreased DPD activity implies a de- neurological toxicity from high doses (cerebellar
creased clearance and an increased half-time of ataxia), ophthalmological toxicity through tear
5-FU, resulting in an increased risk of toxicity18,19. excretion (conjunctivitis, tear hypersecretion),
More than 80% of the 5-FU dose is converted skin toxicity usually aggravated by sun exposure
to inactive metabolite 5-fluoro-5,6-dihydrouracil (hand-foot syndrome, hyperpigmentation, rash,
by DPD19. DPD deficiency accounts for 20-60% hives) and reversible cardiac toxicity caused by
of fluoropyrimidine-related severe toxicity, and continuous perfusion (angina, myocardial infarc-
20-30% can be explained by DPYD deleterious tion, myocardial necrosis, coronary dissection,
variants19,20. It is estimated that 3-5% of Cauca- heart failure, arrhythmia, cardiogenic shock, car-
sians are carriers of a partial DPD deficiency diac arrest, and sudden cardiac death)35-38. Se-
and that 0.1-0.3% present complete deficiency20. vere adverse events may appear within the first
Overall, 5% of the general population present a chemotherapy cycle – a fact that supports the
DPD deficiency21. This pharmacogenetic “DPD importance of treatment personalization before
syndrome” manifests as mucositis/stomatitis, my- treatment initiation37.
3308Role of microRNAs in fluoropyrimidine-related toxicity: what we know
Fluoropyrimidine cardiotoxicity represents cardiac tissue, and (4) TAS-102 is not catabolized
one of the most severe fluoropyrimidine-induced by DPD, which consequently means a reduced
toxicities. The incidence ranges from 1% to 18%, formation of FBAL and a lower risk of cardio-
and chest pain is the most frequent symptom36,37. toxicity due to FBAL accumulation39. A reduced
The incidence variability is due to various man- level of cardiotoxic metabolites also explains the
ifestations of cardiotoxicity, but the risk is in- lack of cardiac toxicity of S-1 due to the presence
fluenced by the schedule and route of admin- in its composition of gimeracil, a DPD-inhibitor.
istration of 5-FU, the use of concurrent chest
radiotherapy or anthracycline administration, How to Assess Fluoropyrimidine Toxicity?
underlying coronary artery disease, and how fre- Over time, many studies have focused on
quently the patients were monitored36,37. Several studying the mechanisms involved in fluoropy-
mechanisms for fluoropyrimidine cardiotoxicity rimidine toxicity. Most strategies have tried to de-
have been proposed, such as (1) vasoconstric- termine the DPD deficiency through genotyping
tion, (2) direct myocardial injury with systolic and phenotyping method (Table I).
dysfunction, (3) accumulation of alpha-fluoro-be- The fact that DPD activity can affect 5-FU
ta-alanine (FBAL), a metabolite of 5-FU, which efficacy through the development of important
is first converted to fluoroacetate and later to adverse events was demonstrated in many stud-
fluorocitrate leading to citrate accumulation and ies, and therefore an upfront screening for func-
downstream depletion of ATP resulting in isch- tionally relevant DPYD genes and treatment ad-
emia, (4) dysfunction of vascular endothelium, justment in patients with related toxicity allelic
(5) hypercoagulable status leading to thrombosis, variants to avoid severe toxicity is justified. The
(5) changes in the shape of erythrocyte mem- first functional mutation related to fluoropyrim-
brane leading to increased blood viscosity and idine toxicity was DPYD*2A. Deenen et al40
decreased ability to carry and release oxygen, demonstrated in a prospective study the clinical
and (6) an acute coronary syndrome caused by validity and utility of DPYD*2A genotype-guid-
an allergic reaction also known as Kounis syn- ed dosing40. However, due to the low frequency
drome3. 5-FU and Capecitabine have the same of DPYD*2A, less than 1% in Caucasian patients,
frequency of cardiac adverse events, while on attention was focused on identifying other DPYD
the other hand, TAS-102 is considered to be a variants associated with DPD deficiency41. Until
“cardio-gentle” fluoropyrimidine. The following now, four variants have demonstrated their utility
mechanism seems to be responsible for the lack and clinical validity based on high-level evidence
of TAS-102 cardiotoxicity: (1) trifluorothymidine from meta-analyses42.
(TFT), an analogue of thymidine and one of the There are situations in which the DPD defi-
components of TAS-102, induces a higher level ciency is not explained by the presence of DPYD
of cell death and does not obtain an autophagic variants or by phenotypic methods. These cases
survival response in cancer cell lines, (2) a dif- are in part explained by a variability in the reg-
ferent oncological target – DNA synthesis, (3) ulation of DPD at the post-transcriptional lev-
the incorporation of the molecule into the DNA el by microRNA. The 3’-untranslated region of
of tumor tissues is higher than the incorporation DPYD is directly targeted by mir-27a, miR-27b,
into DNA of normal tissues, thereby sparing the miR-134, miR-494, miR-582-5p, and in the cod-
Table I. Available methods to identify patients at risk for severe fluoropyrimidine toxicity24-28,42-44,48-53.
Stategies Methods Evidence
Phenotyping methods DPD activity in PBM’s Clinical validity established
Clinical utility in research
Endogenous uracil serum concentration Clinical validity and utility established
2-13C uracil breath test Clinical validity and utility in research
Uracil dose test Clinical validity and utility in research
Genotyping methods DPYD mutation Clinical validity and utility for
DPYD*2A, 13, 9B and HapB3
miRNA mutation Clinical validity and utility in research
DPD – dihydrodioyrimidine dehydrogenase, DPYD – dihydrodioyrimidine dehydrogenase gene, miRNA – microRNA.
3309A.L. Deac, C.C. Burz, C. Militaru, I.C. Bocșan, R.M. Pop, P. Achimaș-Cadariu, A.D. Buzoianu ing sequence by hsa-miR-302b-3p40-43. Of these, 5-fluorouracil, SW480, and SW480/5-FU cells45. miR-27-a and miR-27-b have been shown to So be these meanings, DPYD expression was downregulate DPD expression by targeting an under the control of miR-494, and 5-fluorouracil RNA-induced silencing complex (RISC) protein resistance and toxicity can be associated with to DPYD43. Moreover, miR-27-a functions as an abnormal downregulation of miR-49447. oncogene, and its overexpression has been asso- The gene encoding for thymidylate synthase ciated with poor prognostics, increased risk of (TYMS) has been investigated to highlight the metastasis and disease progression, and chemo- possible role as a biomarker for fluoropyrimidine therapy resistance43. toxicity and effectiveness. Sinicrope et al46 re- The clinical relevance of miR-27a polymor- vealed that the overexpression of TS in colorectal phism has been demonstrated in three studies cancer was related to poor response to 5-flu- on patients undergoing fluoropyrimidine-based orouracil, chemoresistance, and toxicity47. The chemotherapy. Amstutz et al42 showed, in a study TYMS variants associated with fluoropyrimidine with 514 patients who presented fluoropyrimi- toxicity involve tandem repeats of a 28-base- dine-related toxicity after the first two cycles, an pair sequence instead of three in the 5’-untrans- association between rs895819 variant G allele of lated region or a 6-base-pair variation in the miR-27a and increased early-onset toxicity and 3’-untranslated region of TYMS, also known as also the fact that this association is dependent TYMS enhancer region (TSER)47,48. The activity on the DPYD variant related to DPD deficien- of TYMS can also be controlled by microR- cy42. In the same study, another polymorphism, NA. Increased expression of miR-218 suppresses rs11671784, was analyzed, but no association with TYMS-enhanced fluoropyrimidine toxicity and fluoropyrimidine toxicity was observed and no is associated with progression-free survival and significant relation with DPYD mutated variants overall survival in colorectal cancer48. was detected42. Meulendiks et al43 confirmed the Regarding phenotyping methods, the main above information in a study including 1592 pa- methods related to fluoropyrimidine treatment tients in treatment with fluoropyrimidine43. They are the determination of DPD activity in periph- showed that rs895819 polymorphism is mod- eral blood mononuclear cells (PBM), uracil dose erately associated with toxicity, but those who test, pretreatment determination of the endoge- have DPYD mutation also have a significantly nous concentration of dihydrouracil and uracil increased risk grade 3 or 4 toxicity, these facts in plasma, urine, and saliva (UH2/Ura ratio), suggesting the additional role and importance 2-13C uracil breath test49-54. Among all phenotyp- of miR-27-a polymorphism43. The carriers of ic methods, the highest accuracy is assigned to rs11671784 polymorphism showed no significant- pretreatment serum uracil determination54. ly increased risk of toxicity regarding the DPYD status43. In a small study of 64 patients, Falvella et al44 showed in both univariate and multivariate Discussion analysis the association between rs895819 and grade 3 or 4 adverse events44. Side effects are one of the factors that limit Another miRNA that shows promising results the efficacity of chemotherapy, and they usually based on in vitro studies is miR-494. This miR- require either dose reduction or delayed adminis- NA, located in chromosome 14q32.31, works as tration of treatment until remission. an oncogene in breast cancer metastasis and is Due to the multiple indications that fluoro- overexpressed in hepatocellular carcinoma cells, pyrimidines have, they are probably the most although some studies also suggest its tumor sup- commonly used chemotherapeutic agents, and pressor role by repressing the proliferation, mi- therefore it is essential to find ways to prevent gration, and invasion of prostate cancer cells by toxicities that can decrease the efficacity or in- suppression of C-X- C chemokine receptor 4 (CX- terrupt the treatment, or which endanger the CR4) gene, and of gastric cancer cells by target- patient’s life. ing c-myc45,46. Chai et al45 showed in their study Many detection methods are available now- that miR-494 has tumor suppressor function and adays, phenotypic or genotypic, and we know can sensitize colon cancer cells to 5-fluoroura- that the onset of toxicity is influenced by DPD cil by binding to the 3’-untranslated region of activity. At the present time, four variants of DPYD and negatively regulate DPYD expression DPYD have proven their clinical utility and their in modified colon cancer cell lines sensitive to influence on DPD deficiency, but due to the low 3310
Role of microRNAs in fluoropyrimidine-related toxicity: what we know
frequency and the multitude of mutant variants, for colorectal cancer was updated in September
their routine testing has not yet progressed into 2017 and recommended DPYD genotyping in all
clinical practice. It is estimated that almost 3-15% patients before initiating treatment with fluoropy-
of patients present a partial DPD deficiency and rimidine58,59.
0.1-5% a complete deficiency54. On 13 March 2020, the European Medicines
The Group of Clinical Pharmacology in Oncol- Agency’s (EMA) Pharmacovigilance Risk As-
ogy (GPCO)-UNICANCER and the French Net- sessment Committee (PRAC) has recommended
work of Pharmacogenetics (RNPGx) recommend testing for DPD deficiency before initiation of
the following regarding the treatment with fluoro- fluoropyrimidine-based chemotherapy; patients
pyrimidine: (1) the screening of DPD deficiency with complete DPD deficiency should not receive
before starting treatment with 5-fluorouracil or any type of fluoropyrimidine, and those with a
Capecitabine, (2) performing DPD phenotyping partial deficiency can receive fluoropyrimidine
by determination of plasma uracil concentra- treatment with a reduced dose and later in the
tions and DPD genotyping (variants DPYD*2A, course of the treatment adjustment of the dose
DPYD*13, DPYD*9, and Haplotype B3), (3) re- depending on the toxicities associated60.
ducing the first cycle dose of fluoropyrimidine ac- In 2015, uridine triacetate (UT, Vistogard) was
cording to DPD status and later in the treatment approved by FDA as an antidote in case of se-
to consider increasing the dose according to each vere fluoropyrimidine toxicities, with a survival
tolerance55. benefit in 96% of cases, based on two open-label,
The Clinical Pharmacogenetics Implementa- single-arm trials61,62. Vistogard can be used in
tion Consortium (CPIC) has formulated a guide- the first 96 hours after the last dose of 5-FU or
line for better interpretation of clinical DPD Capecitabine for life-threatening toxicities such
genotyping tests and how to adjust the treatment. as severe neutropenia, diarrhea, or cardiotoxicity
Based on DPYD genotype and phenotype they unresponsive to drug cessation and antianginal
calculated DPYD activity score (DPYD-AS) and therapy63.
made the following recommendations: (1) in pa- In recent years, miRs are involved and control
tients who are DPYD normal metabolisers with many of the processes involved in cancer, but also
activity score of 2 (AS) and two normal func- in efficacy, resistance, and toxicity to treatment.
tional alleles a dose modification is not recom- So far, in terms of fluoropyrimidine toxicity, only
mended, (2) in DPYD intermediate metabolisers, mir-27 has proven its potential role as a predic-
meaning decreased DPD activity and increased tive factor. Previous studies45-47 have illustrated
risk of toxicity with AS 1 or 1.5, and one normal that the presence of rs895819A>G presents only
functional plus one non-functional allele, or two a moderate risk of toxicity, but the association of
decreased functional alleles, a reduction of 25 rs895819A>G and a DPYD variant are associated
to 50% is recommended (the percentage of dose with an increased risk of early-onset severe fluo-
reduction depends on activity score) and (3) in ropyrimidine toxicity. This fact highlights the im-
DPYD poor metabolisers with complete DPD portant role that microRNAs could play in DPYD
deficiency and very increased risk of toxicity, genotyping and, subsequently, in providing an
with AS 0 or 0.5 and two non-functional alleles or appropriate treatment with limited side effects.
one non-functional plus one decreased functional As mentioned previously, CPIC recommends the
allele, it is recommended to avoid the use of flu- association of phenotyping and genotyping for
oropyrimidine treatment; if AS 0.5 and there is the screening of DPD deficiency, but the com-
no other therapeutic option, 5-fluorouracil should bined determination between polymorphism on
be administered with a significant dose reduction DPYD gene and microRNA can be a method
and under therapeutic drug monitoring56. with greater accuracy and could help us detect
Another working group, the Dutch Pharmaco- more patients who may be suffering from major
genetics Working Group (DPWG), offers some toxicities.
recommendations regarding fluoropyrimidine
treatment. In contrast to the CPIC guideline, DP-
WG also includes Tegafur in their guideline, not Conclusions
only 5-fluorouracil and Capecitabine; they also
recommend patients with AS 0 or 0.5 using a phe- Even today, when target therapy and immuno-
notyping method to initiate the treatment with a therapy, alone or combined with chemotherapy,
fluoropyrimidine57. The Dutch National guideline tend to become the first-line treatment in many
3311A.L. Deac, C.C. Burz, C. Militaru, I.C. Bocșan, R.M. Pop, P. Achimaș-Cadariu, A.D. Buzoianu
types of cancer, fluoropyrimidine is still the cor- 5) Froehlich TK, Amstutz U, Aebi S, Joerger M, Lar-
nerstone in the treatment of many types of cancer giadèr CR. Clinical importance of risk variants in
the dihydropyrimidine dehydrogenase gene for
and represents one of the most used chemother- the prediction of early-onset fluoropyrimidine tox-
apies worldwide. DPD deficiency and its impli- icity. Int J Cancer 2015; 136: 730-739.
cations in fluoropyrimidine toxicity have been 6) Schwab M, Zanger UM, Marx C, Schaeffeler E,
extensively studied over time, and as a result of Klein K, Dippon J, Kerb R, Blievernicht J, Fischer
these studies, the determination of DPD activity J, Hofmann U, Bokemeyer C, Eichelbaum M. Role
before treatment is recommended or even imple- of genetic and nongenetic factors for fluorouracil
mented; an example would be the Netherlands treatment-related severe toxicity: a prospective
clinical trial by the German 5-FU Toxicity Study
and some of the centres in France. EMA rein- Group. J Clin Oncol 2008; 26: 2131-2138.
forces the studies and recommends testing DPD 7) Almeida MI, Reis RM, Calin GA. MicroRNA histo-
deficiency before starting treatment and adjusting ry: discovery, recent applications, and next fron-
the dose according to the degree of the deficiency. tiers. Mutat Res 2011; 17: 1-8.
The role of miRNA in fluoropyrimidine tox- 8) Acunzo M, Romano G, Wernicke D, Croce CM.
icity is still unclear. On the one hand, we need MicroRNA and cancer – A brief overview. Adv Bi-
several studies that will confirm the clinical ol Regul 2015; 57: 1-9.
utility of miRNAs that are known to be involved, 9) Van Roosbroeck K, Calin GA. Cancer hallmarks
such as miR-27 or miR-494; on the other, we need and microRNAs: the therapeutic connection. Adv
Cancer Res 2017; 135: 119-149.
studies to identify other new miRNAs to help us
easily identify patients who are more likely to 10) Nahand JS, Moghoofei M, Salmaninejad A, Bah-
manpour Z, Karimzadeh M, Nasiri M, Mirzaei HR,
suffer more severe adverse effects. Possible direc- Pourhanifeh MH, Bokharaei-Salim F, Mirzaei H,
tions of research are finding circulating miRNAs Hamblin MR. Pathogenic role of exosomes and
independent of DPD variants or demonstrating microRNAs in HPV-mediated inflammation and
possible correlations between the concentration cervical cancer: a review. Int J Cancer 2020; 146:
of 5-FU or their metabolites and the expression 305-320.
of miRNAs. 11) Si W, Shen J, Zheng H, Fan W. The role and
mechanism of action of microRNAs in cancer
drug resistance. Clin Epigenetics 2019; 25.
12) Nahand SJ, Taghizadeh-Boroujeni S, Karimza-
deh M, Borran S, Pourhanifeh MH, Moghoofei M,
Conflict of Interest Bokharaei-Salim F, Karampoor S, Jafari A, Ase-
The Authors declare that they have no conflict of interests. mi Z, Tbibzadeh A, Namdar A, Mirzaei H. microR-
NAs: New prognostic, diagnostic, and therapeu-
tic biomarkers in cervical cancer. J Cell Physiol
References 2019; 234: 170642-17099.
13) Aghdam AM, Amiri A, Salarinia R, Masoudifar A,
1) Deac AL, Burz CC, Bocșe HF, Bocșan IC, Buzoia- Ghasemi F, Mirzaei H. MicroRNAs as diagnostic,
nu AD. A systematic review on the importance of prognostic, and therapeutic biomarkers in pros-
genotyping and phenotyping in fluoropyrimidine tate cancer. Crist Rev Eukaryot Gene Exor 2019;
treatment. Med Pharm Rep 2020; 93: 223-230. 29: 127-139.
2) Thorn CF, Marsh S, Carillo MW, McLeod HL, 14) Hayes J, Peruzzi PP, Lawler S. MicroRNAs in can-
Klein TE, Altman RB. PharmGKB summary: fluo- cer: biomarkers, functions, and therapy. Trends
ropyrimidine pathways. Pharmacogenet Genom- Mol Med 2014; 20: 460–469.
ics 2011; 21: 237-242. 15) Thomas F, Hennebelle I, Delmas C, Lochon I, Dhel-
3) Lenz HJ, Stintzing S, Loupakis F. TAS-102, a nov- ens C, Garnier Tixidre C, Bonadona A, Penel N,
el antitumor agent: a review of the mechanism of Goncalves A, Delord JP, Toulas C, Chatelut E. Ge-
action. Cancer Treat Rev 2015; 41: 777-783. notyping of a family with a novel deleterious DPYD
mutation supports the pretherapeutic screening of
4) Del Re M, Cinieri S, Michelucci A, Salvadori S, DPD deficiency with dihydrouracil/uracil ratio. Clin
Loupakis F, Schirripa M, Cremolini C, Crucitta S, Pharmacol Ther 2016; 99: 235-242.
Barbara C, Di Leo A, Latiano TP, Pietrantonio F,
Di Donato S, Simi P, Passardi A, De Braud F, Al- 16) Kadoyama K, Miki I, Tamura T, Brown JB, Sakae-
tavilla G, Zamagni C, Bordonaro R, Butera A, da T, Okuno Y. Adverse event profiles of 5-Fluo-
Maiello E, Pinto C, Falcone A, Mazzotti V, Mor- rouracil and Capecitabine data mining of the pub-
ganti R, Danesi R. DPYD*6 plays an important lic version of the FDA Adverse Event Reporting
role in fluoropyrimidine toxicity in addition to DPY- System, AERS, and reproducibility of clinical ob-
D*2A and c.2846A>T: a comprehensive analysis servations. Int J Med Sci 2012; 9: 33-39.
in 1254 patients. Pharmacogenomics J 2019; 19: 17) Pinheiro LC, Durand J, Dogne JM. An application
556-563. of machine learning in pharmacovigilance: esti-
3312Role of microRNAs in fluoropyrimidine-related toxicity: what we know
mating likely patient genotype form phenotypical c.1679T>G, c.1236G>A/HapB3, and c.1601G>A
manifestations of fluoropyrimidine toxicity. Clin as predictors of severe fluoropyrimidine-associ-
Pharmacol Ther. 2020; 107: 944-947. ated toxicity: a systematic review and meta-anal-
18) Henricks LM, Opdam FL, Beijnen JH, Cats A, ysis of individual patient data. Lancet Oncol 2015;
Schellens JHM. DPYD genotype-guided dose in- 16: 1639-1650.
dividualization to improve patient safety of fluoro- 29) Abbasian MH, Ansarinejad N, Abbasi B, Iravani
pyrimidine therapy: call for a drug label update. M, Ramim T, Hamedi F, Ardekani AM. The role
Ann Oncol 2017; 28: 2915-2922. of dihydropyrimidine dehydrogenase and thymi-
19) Hamzic S, Amstutz U, Largiadèr CR. Come a long dylate synthase polymorphisms in fluoropyrimi-
way, still a way to go: from predicting and prevent- dine-based cancer chemotherapy in an Iranian
ing fluoropyrimidine toxicity to increased effica- population. Avicenna J Med Biotechnol 2020; 12:
cy? Pharmacogenomics 2018; 19: 689-692. 157-164.
20) Barin-Le Guellec C, Lafay-Chebassier C, Ingrand 30) Hamzic S, Kummer D, Froehlich TK, Joerger M,
I, Tournamille JF, Boudet A, Lanoue MC, De- Aebi S, Palles C, Thomlinson I, Meulendijks D,
fossez G, Ingrand P, Perault-Pochat MC, Eti- Schellens JHM, Garcia-Gonzalez X, Lopez-Fer-
enne-Grimaildi MC. Toxicities associated with nandez LA, Amstutz U, Largiader CR. Evaluat-
chemotherapy regimens containing a fluoropy- ing the role of ENOSF1 and TYMS variants as
rimidine: a real-life evaluation in France. Eur J predictors in fluoropyrimidine-related toxicities:
Cancer 2020; 124: 37-46. an IPD meta-analysis. Pharmacol Res 2020; 152:
104594.
21) Tsutsui M, Yamamoto S, Yoshikawa Y, Nakan-
ishi R, Takano K, Osumi K, Akatsu T, Yoneya- 31) Rosmarin D, Palles C, Pagnamenta A, Kaur K,
ma K, Nakagawa M, Kanai T. Severe adverse Pita G, Martin M, Domingo E, Jones A, How-
events due to dihydropyrimidine dehydrogenase arth K, Freeman-Mills L, Johnstone E, Wang H,
deficiency in a Japanese patient with colon can- Love S, Scudder C, Julier P, Fernandez-Rozadil-
cer taking capecitabine: a case report. Int Cancer la C, Ruiz-Ponte C, Carracedo A, Castellvi-Bel
Conf J 2018; 15: 125-129. S, Castells A, Gonzalez-Neira A, Taylor J, Kerr
R, Kerr D, Tomlinson I. A candidate gene study
22) Saif MW, Hachem H, Purvey S, Hamal R, Zhang of capecitabine-related toxicity in colorectal can-
L, Siddiqui NS, Godara A, Diasio RB. pharmaco- cer identifies new toxicity variants at DPYD and a
genetic variants in the DPYD and TYMS genes putative role for ENOSF1 rather than TYMS. Gut
are clinically significant predictors of fluoropyrim- 2015; 64: 111-120.
idine toxicity: are we ready for use in our clinical
practice. Arch Pharmacol Ther 2020; 2: 6-8. 32) Jiang H, Shen Y. Methylene tetrahydrofolate re-
ductase (MTHFR) gene rs1801133 C> T poly-
23) Wigle TJ, Tsvetkova EV, Welch SA, Kim RB. morphisms and response to 5-FU based chemo-
DPYD and Fluorouracil-based chemothera- therapy in patients with colorectal cancer: a me-
py: mini review and case report. Pharmaceutics ta-analysis. Pteridines 2019; 30: 126-132.
2019; 11: 1-17.
33) Chen J, Ying X, Zhang L, Xiang X, Xiong J. Influ-
24) Lam SW, Guchelaar HJ, Boven E. The role of ence of TS and ABCB1 gene polymorphisms on
pharmacogenetics in capecitabine efficacy and survival outcomes of 5-FU-based chemotherapy
toxicity. Cancer Treat Rev 2016; 50: 9-22. in a Chinese population of advanced gastric can-
25) Mercier C, Ciccolini J. Profiling dihydropyrimidine cer patients. Wien Klin Wochenschr 2017; 129:
dehydrogenase deficiency in patients with can- 420-426.
cer undergoing 5-fluorouracil/capecitabine thera- 34) Liu D, Li X, Li X, Zhang M, Zhang J, Hou D, Tong
py. Clin Colorectal Cancer 2006; 6: 288-296. Z, Dong M. CDA and MTHFR polymorphisms are
26) Terrazzino S, Cargnin S, Del Re M, Danesi R, Ca- associated with clinical outcomes in gastroenteric
nonico PL, Genazzani AA. DPYD IVS14+1G>A cancer patients treated with capecitabine-based
and 2846A>T genotyping for the prediction of chemotherapy. Cancer Chemother Pharmacol
severe fluoropyrimidine-related toxicity: a me- 2019; 83: 939-949.
ta-analysis. Pharmacogenomics 2013; 14: 1255- 35) Chu E, DeVita Jr. VT. Physicians’ Cancer Chemo-
1272. therapy Drug Manual. Jones and Barlett, 2020.
27) Offer SM, Fossum CC, Wegner NJ, Stuflesser AJ, 36) Kanduri J, More LA, Godishala A, Asnani A. Flu-
Butterfield GL, Diasio RB. Comparative functional oropyrimidine-associated cardiotoxicity. Cardiol
analysis of DPYD variants of potential clinical rel- Clin 2019; 37: 399-405.
evance to dihydropyrimidine dehydrogenase ac-
tivity. Cancer Res 2014; 74: 2545-2554. 37) Deac AL, Burz CC, Bocsan IC, Buzoianu AD. Flu-
oropyrimidine-induced cardiotoxicity. World J Clin
28) Meulendiks D, Henricks LM, Sonke GS, Deenen Oncol 2020; 11: 1008-1017.
MJ, Froelich TJ, Amstutz U, Largiader CR, Jen-
nings BA, Marinaki AM, Sanderson JD, Kleibl 38) Shiga T, Hiraide M. Cardiotoxicities of 5-fluoro-
Z, Kleibova P, Schwab M, Zanger UM, Paller C, uracil and other fluoropyrimidines. Curr Treat Op-
Tomlinson I, Gross E, van Kuilenburg ABP, Punt tions Oncol 2020; 21: 27.
CJA, Koopman M, Beijnen JH, Cats A, Schel- 39) Petrelli F, Barni S, Betocchi P, Zaniboni A. TAS-
lens JHM. Clinical relevance of DPYD variants 102, the first “cardio-gentle” fluoropyrimidine in
3313A.L. Deac, C.C. Burz, C. Militaru, I.C. Bocșan, R.M. Pop, P. Achimaș-Cadariu, A.D. Buzoianu
the colorectal cancer landscape? BMC Cancer 49) Kristensen MH, Pedersen P, Mejer J. The value
2016; 16: 386. of dihydrouracil/uracil plasma ratios in predicting
40) Deenen MJ, Meulendijks D, Cats A, Sechterberg- 5-fluorouracil-related toxicity in colorectal cancer
er MK, Severens JL, Boot H, Smits PH, Rosing H, patients. J Int Med Res 2010; 38: 1313-1323.
Mandigers CMPW, Soesan M, Beijnen JH, Schel- 50) Mattison LK, Ezzeldin H, Carpenter M, Modak A,
lens JHM. Upfront genotyping of DPYD⁄2A to in- Johson MR, Diasio RB. Rapid identification of di-
dividualize fluoropyrimidine therapy: a safety and hydropyrimidine dehydrogenase deficiency by us-
cost analysis. J Clin Oncol 2016; 34: 227-234. ing a novel 2-13C-uracil breath test. Clin Cancer
41) Meulendijks D, Cats A, Beijnen JH, Schellens JHM. Res 2004; 10: 2652-2658.
Improving safety of fluoropyrimidine chemothera- 51) Cunha-Junior GF, De Marco L, Bastos-Rodrigues
py by individualizing treatment based on dihydropy- L, Bolina MB, Martins FL, Pianetti GA, Cesar IC,
rimidine dehydrogenase activity--Ready for clinical Coelho LG. (13)C-uracil breath test to predict
practice?. Cancer Treat Rev 2016; 50: 23-34. 5-fluorouracil toxicity in gastrointestinal cancer
42) Amstutz U, Offer SM, Sistonen J, Joeger M, Di- patients. Cancer Chemother Pharmacol 2013; 72:
asio RB, Largiader CR. Polymorphism in mi- 1273-1282.
R27A associated with early-onset toxicity in fluo- 52) Carlsson G, Odin E, Gustavsson B, Wettergen
ropyrimidine-based chemotherapy. Clin Can Res Y. Pretherapeutic uracil and dihydrouracil lev-
2015; 21: 2038-2044. els in saliva of colorectal cancer patients are as-
43) Meulendijks D, Henricks LM, Amstutz U, Froe- sociated with toxicity during adjuvant 5-fluoro-
lich TK, Largiarder CR, Beijnen JH, de Boer A, uracil-based chemotherapy. Cancer Chemother
Deenen MJ, Cats A, Schellens HM. Rs895819 in Pharmacol 2014; 74: 757-763.
MIR27A improves the predictive value of DPYD 53) Hayashi K, Kidouchi K, Sumi S, Mizokami M, Ori-
variants to identify patients at risk of severe flu- to E, Kumada K, Ueda R, Wada Y. Possible pre-
oropyrimidine-associated toxicity. Int J Cancer diction of adverse reactions to pyrimidine chemo-
2016; 138: 2752-2761. therapy from urinary pyrimidine levels and a case
44) Falvella FS, Cheli S, Martinetti A, Mazzali C, Ia- of asymptomatic adult dihydropyrimidinuria. Clin
covelli R, Maggi C, Gariboldi M, Pierotti MA, Cancer Res 1996; 2: 1937-1941.
DIBartolomeo M, Sottotetti E, Mennitto R, Bossi I, 54) Boisdron-Celle M, Capitain O, Faroux R, Borg C,
de Braud F, Clementi E, Pietrantonio F. DPD and Metges JP, Galais MP, Kaassis M, Bennouna J,
UGT1A1 deficiency in colorectal cancer patients Bouhier-Leporrier K, Francois E, Baumgaertner I,
receiving triplet chemotherapy with fluoropyrimi- Guerin-Becuwe C, Cojocarasu O, Roemer-Becu-
dines, oxaliplatin and irinotecan. Br J Clin Phar- we C, Stampfli C, Rosenfeld L, Lecompte T, Berg-
macol 2015; 80: 581-588. er V, Morel A, Gamelin E. Prevention of 5-fluoro-
45) Chai J, Dong W, Xie C, Wang L, Han DL, Wang uracil-induced early severe toxicity by pre-ther-
S, Guo HL, Zhang ZL. MicroRNA-494 sensitizes apeutic dihydropyrimidine dehydrogenase defi-
colon cancer cells to fluorouracil through regula- ciency screening: assessment of a multiparamet-
tion of DPYD. IUBMB Life 2015; 67: 191-201. ric approach. Semin Oncol 2017; 44: 13-23.
46) Marjaneh RM, Khazaei M, Ferns GA, Avan A, 55) Loriot MA, Ciccolini J, Thomas F, Barin-Le-Guel-
Aghaee-Bakhiatiari SH. The role of microRNA in lec C, Royer B, Milano G, Picard N, Becquemont
5-FU Resistance of colorectal: possible mecha- L, Verstuyft C, Narjoz C, Schmitt A, Bobin-Du-
nism. J Cell Physiol 2019; 234: 2306-2316. bigeon C, Harle A, Paci A, Poinsignon V, Quar-
anta S, Evrard A, Hennart B, Broly F, Fonrose
47) Sinicrope FA, Foster NR, Thibodeau SN, Marsoni
X, Lafay-Chebassier C, Wozny AS, Masskouri F,
S, Monges G, Labianca R, Sargent DJ. DNA mis-
Boyer JC, Etienne-Grimaldi MC. Dihydropyrimi-
match repair status and colon cancer recurrence
dine déhydrogenase (DPD) deficiency screening
and survival in clinical trials of 5‐fluorouracil‐
and securing of fluoropyrimidine-based chemo-
based adjuvant therapy. J Natl Cancer Inst 2011;
therapies: update and recommendations of the
103: 863-875.
French GPCO-Unicancer and RNPGx Network.
48) Rosmarin D, Palles C, Church D, Domingo E, Bull Cancer 2018; 105: 397-407.
Jones A, Johnstone E, Wang H, Love S, Julier P,
56) Amstutz U, Henricks LM, Offer SM, Barbarino J,
Scudder C, Nicholson G, Gonzalez-Neira A, Mar-
Schellens JHM, Swen JJ, Klein TE, McLeod HL,
tin M, Sargent D, Green D, McLeod H, Zanger
Caudle KE, Diasio RB, Schwab M. Clinical Phar-
UM, Schwab M, Braun M, Seymour M, Thompson
macogenetics Implementation (CPIC) guideline
L, Lacas B, Boige V, RIbelles N, Afzal S, Enghu-
for dihydropyrimidine dehydorgenase genotype
sen H, Jensen SA, Etienne-Grimaldi MC, Milano
and fluoropyrimidine dosing: 2017 Update. Clin
G, Wandelius M, Glimelius B, Garmo H, Gusella
Pharmacol Ther 2018; 103: 210-216.
M, Lecomte T, Laurent-Puig P, Martinez-Balibrea
E, Sharma R, Garcia-Foncillas J, Kleibl Z, Morel 57) Lunenburg CATC, van der Wouden C, Nijenhu-
A, Pignon JP, Midgley R, Kerr D, Tomlinson I. Ge- is M, Crommentuijn-van Rhenen MH, de Bo-
netic markers of toxicity from Capecitabine and er-Veger NJ, Buunk AM, Houwink EJF, Mulder H,
other fluorouracil-based regimens: investigation Rongen GA, van Schaik RHN, van der Weide J,
in the QUASAR2 study, systemic review, and me- Wilffert B, Deneer VHM, Swen JJ, Guchelaar HJ.
ta-analysis. J Clin Oncol 2014; 32: 1031-1039. Dutch Pharmacogenetics Working Group (DP-
3314Role of microRNAs in fluoropyrimidine-related toxicity: what we know
WG) guideline for the gene-drug interaction of 61) Ma WW, Saif MW, El-Rayes BF, Fakih MG, Cart-
DPYD and fluoropyrimidine. Eur J Hum Genet wright TH, Posey JA, King TR, von Borstel RW,
2020; 28: 508-517. Bamat MK. Emergency use of uridine triacetate
for the prevention and treatment of life-threaten-
58) NVMO (2017). Update richtlijn colorectaal car- ing 5- fluorouracil and capecitabine toxicity. Can-
cinoom Medische Oncologie 2017 (21-9-2017.) cer 2017; 123: 345-356.
[Available from: https://www.nvmo.org/wp-con-
tent/uploads/2018/07/Update_richtlijn_CRC_ 62) Ison G, Beaver JA, McGuinn WD Jr, Palmby TR,
sept_2017.pdf. Dinin J, Charlab R, Marathe A, Jin R, Liu Q, Chen
XH, Ysern X, Stephens O, Bai G, Wang Y, Dorff
59) Martens FK, Huntjens DW, Rigter T, Bartels M, SE, Cheng J, Tang S, Sridhara R, Pierce W, McK-
Bet PM, Cornel MC. DPD Testing before treat- ee AE, Ibrahim A, Kim G, Pazdur R. FDA approv-
ment with fluoropyrimidines in the Amsterdam al: uridine triacetate for the treatment of patients
UMCs: an evaluation of current pharmacogenetic following fluorouracil or capecitabine overdose or
practice. Front Pharmacol 2020; 10: 1609. exhibiting early-onset severe toxicities following
60) European Medicines Agency. New testing and treat- administration of these drugs. Clin Cancer Res
ment recommendations for fluorouracil, capecit- 2016; 22: 4545-4549.
abine, tegafur and flucytosine. Available from: 63) Depetris I, Marino D, Bonzano A, Cagnazzo
https://www.ema.europa.eu/en/documents/refer- C, Filippi R, Aglietta M, Leone F. Fluoropyrimi-
ral/fluorouracil-fluorouracil-related-substances-arti- dine-induced cardiotoxicity. Crit Rev Oncol He-
cle-31-referral-new-testing-treatment_en.pdf. matol 2018; 124: 1-10.
3315You can also read

















































