Developmental Relations Between Internalising Problems and ADHD in Childhood: a Symptom Level Perspective
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Research on Child and Adolescent Psychopathology (2021) 49:1567–1579
https://doi.org/10.1007/s10802-021-00856-3
Developmental Relations Between Internalising Problems and ADHD
in Childhood: a Symptom Level Perspective
Lydia Gabriela Speyer1 · Manuel Eisner2,3 · Denis Ribeaud3 · Michelle Luciano1 · Bonnie Auyeung1,4 ·
Aja Louise Murray1,2
Accepted: 27 July 2021 / Published online: 7 August 2021
© The Author(s) 2021
Abstract
ADHD and internalising problems commonly co-occur with up to 50% of children diagnosed with ADHD also suffering
from anxiety or depression. However, their developmental relations are currently not well understood. Longitudinal symp-
tom level analyses can provide valuable insights into how difficulties in these areas of psychosocial functioning affect each
other. Using Gaussian Graphical Models and Graphical Vector Autoregression Models, this study estimated cross-sectional
and longitudinal networks of ADHD and internalising symptoms in 1387 children using parent- and teacher-reported Social
Behaviour Questionnaires (SBQ) when children were aged 7, 9 and 11. Cross-sectional and longitudinal networks suggested
that ADHD shares reciprocal relations with internalising symptoms through a number of potential bridge symptoms that
are primarily connected to anxiety symptoms. High scores on child cannot sit still, is restless, or hyperactive were found to
be the strongest bridge symptom acting as an antecedent to higher internalising symptoms whereas child is worried was the
strongest antecedent for higher ADHD symptoms. Findings of this study highlight several potential bridge symptoms that
may serve as key intervention targets and further emphasise the need for clinicians to assess children presenting with ADHD
symptoms for internalising problems and vice versa.
Keywords ADHD · Internalising problems · Longitudinal network modelling · Z-proso
Attention Deficit Hyperactivity Disorder (ADHD) is one of relations (Jarrett & Ollendick, 2008). In addition, most studies
the most common mental health issues in children, affecting investigating the co-occurrence of ADHD and internalising
around 6.5% of youths worldwide (Polanczyk et al., 2015). problems have focused on clinical samples (Jarrett &
ADHD frequently co-occurs with internalising problems, Ollendick, 2008). Since both ADHD and internalising
with prevalence estimates in children ranging from 12 to symptoms have been shown to lie on a continuum within the
50% for co-occurring depression and from 15 to 35% for general population (Lubke et al., 2009; Tebeka et al., 2018),
co-occurring anxiety (Gnanavel et al., 2019). However, these studies should be complemented with community-
relatively few studies have examined the links between ADHD based samples to provide a comprehensive picture of the links
symptoms and internalising problems longitudinally, making between ADHD and internalising problems.
it difficult to draw any conclusions on the direction of their Existing evidence on the longitudinal development of
internalising problems and ADHD in normative samples
* Lydia Gabriela Speyer suggests that they share reciprocal relations, with, for exam-
lspeyer@ed.ac.uk ple, internalising problems leading to higher ADHD symp-
tomatology and vice versa across mid- to late- adolescence
1
Department of Psychology, Univsersity of Edinburgh, (Murray et al., 2020a, b). Less is known about their relations
Edinburgh, UK
before this period, which, in the context of the co-occurrence
2
Violence Research Centre, Institute of Criminology, of ADHD and internalising symptoms, may be a particu-
University of Cambridge, Cambridge, UK
larly vulnerable period given that the median age-of-onset
3
Jacobs Center for Productive Youth Development, University of internalising problems has been found to be at around age
of Zurich, Zurich, Switzerland
11 (Kessler et al., 2005). ADHD typically manifests before
4
Autism Research Centre, Department of Psychiatry, the age of 7 but often only gets diagnosed after school entry
University of Cambridge, Cambridge, UK
13
Vol.:(0123456789)
1568 Research on Child and Adolescent Psychopathology (2021) 49:1567–1579 as difficulties become more apparent in this setting (Sax serving as a means to describe a specific symptom network. & Kautz, 2003). Hence, to understand the etiology of co- This approach also allows for a more parsimonious under- occurring ADHD and internalising problems, it is of real standing of co-occurring mental health problems given that importance to understand the temporal and concurrent rela- symptoms between mental health disorders show substantial tions of ADHD and internalising symptoms in the period overlap (e.g. concentration difficulties are not only a symp- leading up to adolescence. tom of ADHD but also of depression) (American Psychiat- To date, the mechanisms that underlie the relations ric Association, 2013). Hence, symptom networks between between ADHD and internalising symptoms are still not different disorders are likely to be connected through spe- well understood. This is also partly due to limitations in cific symptoms. These connecting symptoms are commonly the methodology for analysing longitudinal panel data. referred to as ‘bridge symptoms’ and might act as the driv- Most longitudinal studies investigating the links between ing force in the development of a co-occurring disorder by ADHD and internalising problems (e.g. Obsuth et al., 2020) activating another symptom network (Borsboom & Cramer, have used modelling techniques such as cross-lagged panel 2013). This has important implications for clinical inter- models (CLPM), which conflate between- and within-person ventions. Knowing which symptoms might underlie the effects and thus provide ambiguous results regarding the development of another disorder allows for more targeted development of co-occurring mental health issues (Berry and consequently more effective interventions. To further & Willoughby, 2017). An alternative to traditionally used maximise the impact of potential interventions, it is further statistical techniques such as CLPMs are graphical vector crucial to know how these symptom networks change over autoregression (GVAR) models (Epskamp, 2020). GVAR development. In response to the emergence of the network models allow for the separation of within- and between- approach to psychopathology, a number of studies have esti- person effects and are consequently well suited to investigate mated cross-sectional symptom level networks (e.g. Beard dynamic relations between multiple mental health domains. et al., 2016; Rouquette et al., 2018; Silk et al., 2019), some GVAR models further have the advantage that they allow also examining how these symptom networks changed over for an intuitive visualisation and interpretation of complex time (e.g. Martel et al., 2016), and providing insights into results, making it possible to not only investigate the the structure of symptoms underlying mental health. How- relations between multiple mental health domains at the ever, while cross-sectional symptom networks can highlight domain level but also at the symptom level. potential bridge symptoms, they are limited in that they do Another factor that has thus far limited our understand- not give any information on direction of effects. Understand- ing of the links between ADHD symptoms and internalising ing the direction of effects is critical as this could inform problems has been the focus on the disorder level rather the etiology of psychopathology and enables interventions to than the symptom level. There has been some evidence that target the right symptoms at the appropriate time. To date, specific symptoms of internalising problems might be more there have been very few attempts to model the temporal relevant in their association with ADHD than others and relations between symptom networks, with the few stud- vice versa (Michelini et al., 2015). In particular, symptoms ies attempting to model them longitudinally suffering from of anxiety, such as excessive worrying, have been hypoth- similar limitations as domain level analyses. Funkhouser esised to put additional drain on attentional resources, lead- et al. (2020), for instance, used cross‐lagged panel network ing to inattentive behaviour (Zainal & Newman, 2020). On analysis to analyse symptoms of internalising, externalis- the other hand, attention problems might make it more dif- ing and attention symptoms over two time points, which ficult to shift attention away from ruminative thoughts and like CLPMs, conflates within- and between-person effects. thus exacerbate internalising symptoms (Mitchell et al., Thus, there is a clear need for more appropriate modelling 2013). Thus, some symptoms might be more important in of longitudinal symptom networks. the relations between ADHD and internalising problems, An additional limitation of many studies on the devel- making them priority intervention targets. To identify these opmental relations of different mental health issues stems symptoms, symptom level analyses are needed. Indeed, from the fact that they often rely on a single informant to symptom level analyses have recently gained in popularity measure children’s socio-emotional functioning. Evidence due to a shift in the understanding of mental health disor- from cross-informant studies indicates that different inform- ders that has resulted in the development of the network ants only show small-to-moderate degrees of convergence in approach to psychopathology (Borsboom, 2008). Rather their assessment of children’s mental health, especially when than conceptualising mental health disorders as a collection these informants experience children in different contexts of symptoms caused by a unitary underlying abnormality, (e.g. home or school) (Murray et al., 2007, 2018). Conse- the network approach to psychopathology views mental quently, studies investigating children’s mental health should health disorders as dynamic networks of multiple mutually replicate their findings based on assessments from at least reinforcing symptoms with taxonomic classifications only one other informant. This is particularly relevant in the study 13
Research on Child and Adolescent Psychopathology (2021) 49:1567–1579 1569
of ADHD as, according to the DSM-5 diagnostic criteria, ADHD symptoms were available from parents and teachers.
a diagnosis is only warranted if individuals show difficul- At the age 7 wave, data was available for 1370 youths, at
ties in at least two different settings (American Psychiatric the age 9 wave for 1321 and at the age 11 wave for 1147
Association, 2013). youths. All children who had data on internalising symptoms
In the current study, we investigate the developmental and ADHD for at least one time-point from at least one
relations of internalising symptoms and ADHD symptoms informant were included in the current study, resulting in a
in a large community-based study of N = 1387 children. final sample of 1387 children (51% male).
Symptoms of anxiety, depression, inattention and hyper- The z-proso study obtained ethical approval from the
activity/impulsivity were measured at median-ages 7, 9 Ethics Committee from the Faculty of Arts and Social Sci-
and 11 using parent-reported Social Behaviour Question- ences of the University of Zurich. Parents provided active
naires (SBQ). Using Gaussian Graphical Models (GGM) informed consent for children to participate in the study. For
and Graphical Vector Autoregression Models, we estimate additional details regarding recruitment, retention, and attri-
cross-sectional as well as longitudinal symptom networks tion, see elsewhere (Eisner & Ribeaud, 2007; Eisner et al.,
of ADHD and internalising problems to gain new insights 2019) and the z-proso website (https://www.jacobscenter.
into concurrent and temporal relations of symptoms bridging uzh.ch/en/research/zproso/aboutus.html).
ADHD and internalising problems. To evaluate the stabil-
ity of our results across informants, we further replicate all
cross-sectional models using teacher-reported SBQs. As this Measures
is the first study to investigate the symptom-level relations of
ADHD symptom and internalising problems longitudinally, Symptoms of ADHD and internalising problems were
we took an exploratory approach. measured using parent- and teacher-reported versions of
the Social Behaviour Questionnaire (SBQ; Tremblay et al.,
1991). The SBQ is an omnibus measure of psychopathol-
Methods ogy and measures children’s psychosocial functioning
across five areas: ADHD, anxiety/depression, aggression,
Participants non-aggressive externalizing problems, and prosocial behav-
iour. At ages 7, 9 and 11 in the z-proso study, SBQs were
Participants in this study were part of the Zurich Project on completed by parents and teachers and included four items
Social Development from Childhood to Adulthood (z-proso), each on symptoms of inattention, hyperactivity/impulsivity,
a longitudinal study based in Zurich, Switzerland, that has and depression, as well as three items on symptoms of anxi-
been tracking the development of an initial target sample of ety. Items were rated on a 5-point Likert scale from Never
1675 children from 2004 when the children entered school at to Very Often. SBQs were administered using a German
age 7. Children were recruited based on a stratified sampling translation of the original SBQ which teachers completed
design whereby 56 public primary schools in Zurich were in the form of a paper-and-pencil questionnaire while parents
selected based on school size and location. Participants were took part in a computer-assisted personal interview that was
ethnically diverse with only 39.6% of primary caregivers available in an additional nine languages for non-German
being native speakers of the official language of Zurich, that speaking participants. For English phrasings of the items
is German, after which the most frequently spoken native used in this study see Table 1. While self-reported SBQs
languages were Serbian/Bosnian/Croatian (10%), Albanian were also available, those were not used in the current study
(9%), Portuguese (7%) and Tamil (5.3%) (Eisner et al., as they were collected in the form of an adapted computer-
2019). To maximize engagement of the non-German-native based multimedia version of the SBQ with children answer-
speakers, contact letters as well as parent interviews were ing ‘yes’ or ‘no’ to a series of questions relating to their
made available in the in the ten most commonly spoken psycho-social development. Psychometric analyses of the
languages. Of the children’s male primary caregivers who SBQ have found support for factorial validity, developmental
contributed to the first wave of data collection, 76.7% invariance and criterion validity of the SBQ items across
were in full-time employment (8.8% unemployed), with various waves of the z-proso study (Murray et al., 2017,
16% having a university-level education, 15.5% a higher 2020a, b). The SBQ has further been shown to be a reliable
vocational education 7.8% A-levels, 35.2% apprenticeship measure of moderately low to very high levels of internalis-
and 21% mandatory school or less (Murray et al., 2016). To ing and ADHD symptoms in the general population (Murray
date, there have been ten waves of data collection at ages 7 et al., 2019). Descriptive Statistics as well as correlation
to 13, 15, 17 and most recently at age 20 with data collection tables of all SBQ items included in the current study are
still ongoing. This study uses data from waves at median- available online (Table S1 in the supplementary and excel
ages 7, 9 and 11 at which the same items on internalising and files E1 and E2).
131570 Research on Child and Adolescent Psychopathology (2021) 49:1567–1579
Table 1 ADHD and Item Domain Item Content
Internalising Problems Items
02 (NER) Anxiety < CHILD > is nervous, high-strung or tense
03 (ANX) Anxiety < CHILD > is too fearful or anxious
04 (WOR) Anxiety < CHILD > is worried
05 (DEP) Depression < CHILD > seems to be unhappy, sad, or depressed
06 (NHA) Depression < CHILD > is not as happy as other children
07 (TEN) Depression < CHILD > has trouble enjoying him\herself
08 (DIS) Depression < CHILD > appears miserable, distressed, or unhappy
10 (IMP) Hyperactivity/impulsivity < CHILD > is impulsive, acts without thinking
11 (DWA) Hyperactivity/impulsivity < CHILD > has difficulty awaiting turn in games or groups
12 (RES) Hyperactivity/impulsivity < CHILD > cannot sit still, is restless, or hyperactive
13 (FID) Hyperactivity/impulsivity < CHILD > fidgets
14 (CSE) Inattention < CHILD > cannot settle to anything for more than a few moments
15 (DTB) Inattention < CHILD > is distractible, has trouble sticking to any activity
16 (CON) Inattention < CHILD > cannot concentrate, cannot pay attention for long
17 (INA) Inattention < CHILD > is inattentive
Statistical Analyses using the panelgvar() function of the R package psychon-
etrics (Epskamp, 2020). GVAR models describe variables
To improve our understanding of the concurrent relations that have been measured at several time points as a function
between symptoms of ADHD and internalising prob- of their own past values or as a combined function of their
lems, a series of cross-sectional networks was estimated own as well as other variables’ past values, allowing insights
using Gaussian Graphical Models (GGM). For each time into temporal as well as concurrent relations between several
point (ages 7, 9 and 11), separate networks for parent- and repeatedly measured variables (Wild et al., 2010). These
teacher-reported symptoms were built. GGMs use partial temporal and concurrent relations can be visualised using
correlations to intuitively visualise the complex depend- GGMs that include directed edges to visualise temporal rela-
ence structures of a system of variables. In GGMs, vari- tions and undirected edges to visualise concurrent relations.
ables are represented by nodes that are connected through If the data includes a multilevel structure, GVAR models
directed (temporal network) or undirected (contemporaneous also estimate cross-sectional between-person differences
network) edges which visualise the relations between vari- across time, which enables the separation of within- from
ables (Epskamp et al., 2018a, b). Edge weights (w) quan- between-person effects (Epskamp, 2020). This separation
tify the strength of the association in the form of partial is critical since between-person effects, which describe
correlations. Networks were estimated using the R package how someone’s average on a specific symptom compares to
qgraph (Epskamp et al., 2012) which implements graphi- someone else’s average on another symptom, act as a con-
cal LASSO (least absolute shrinkage and selection opera- found when the interest lies on investigating within-person
tor) regularization in combination with Extended Bayesian effects. Within-person effects describe individuals’ devia-
Information Criterion (EBIC) as model selection criterion tions from their own average symptom levels and can give
to estimate a sparse network structure (Epskamp & Fried, insights into whether high- or low-levels on one symptom
2018). Using the R-package bootnet (Epskamp et al., 2018a, influence that same person’s levels on another symptom.
b), 95% Confidence Intervals (CIs) for edge weights were Investigating within-person effects is critical as they can
obtained through bootstrapping routines (N = 1000). Lastly, give insights into the mechanisms that might underlie the
cross-sectional networks at different time points as well as associations between two symptoms and represent the prime
parent- and teacher-reported models were compared using target for interventions (Hamaker et al., 2015). Structurally,
permutation based Network Comparison Tests (NCT) which GVAR models are closely related to the Random-Intercept
offer information on whether networks differed in global Cross-lagged Panel Model (RI-CLPM) which separates
network strength (S: sum of all edge weights; DiffS: Differ- within- from between-person effects by partialling out sta-
ence in S between two networks) and in network structure ble-between person differences through random intercepts
(M) (Van Borkulo et al., 2015). for each repeatedly measured variable that are allowed to co-
To analyse the longitudinal relations between ADHD vary (Hamaker et al., 2015). In contrast to RI-CLPMs which
and internalising symptoms, a Graphical Vector Autore- model the within- and between-person covariance structures
gression (GVAR) model was built for parent-reported data as marginal variance–covariance matrices, GVAR models,
13Research on Child and Adolescent Psychopathology (2021) 49:1567–1579 1571
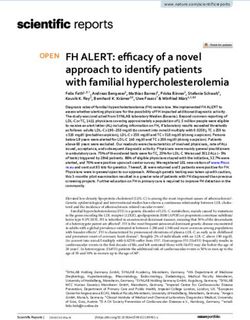
however, model these as GGMs. Also, to avoid the need to symptoms from other domains (see Fig. 1). Internalising
for estimating a variance–covariance structure for the first domains (i.e., anxiety and depression) and ADHD domains
measurement point, GVAR models assume stationary rela- (i.e., hyperactivity/impulsivity and inattention) also formed
tions, thus, unlike RI-CLPMs, they treat the first measure- distinct clusters. At every time point, these clusters were
ment wave as endogenous (Epskamp, 2020). connected through links between item 13 (FID, Child fidgets)
Before building the GVAR models, data was detrended from the hyperactivity/impulsivity domain and item 2 (NER,
for linear age-related effects and standardised across time Child is nervous, high-strung or tense) from the anxiety
points to meet the stationarity assumption of GVAR mod- domain. At age 7, item 2 further shared an edge with item 12
els. This was considered appropriate for the current analy- (RES, Child cannot sit still, is restless, or hyperactive) from
ses because only the correlational structure and not the the hyperactivity/impulsivity domain. Bridge influence indi-
mean structure was of interest. In order to appropriately ces confirmed these visual findings (see Table 2). Pairwise
account for missing data, the GVAR model was fitted using NCTs indicated that network structures and global network
Full Information Maximum Likelihood (FIML) estimation strength (S7 = 5.97, S9 = 6.06, S11 = 6.25) were invariant over
which provides unbiased estimates under the assumption time with all comparisons yielding p-values larger than 0.05
that data is missing at random (Enders, 2001). To mini- (M7vs9 = 0.10. M7vs11 = 0.12, M9vs11 = 0.10; DiffS7vs9 = 0.10,
mise the chance of finding false positives and to reduce DiffS7vs11 = 0.28, DiffS9vs11 = 0.19). Results of bootstrapping
the model’s complexity, the model was further regularised routines indicated that edges between bridge symptoms were
(i.e., constrained to only include the most important edges) moderately stable. Confidence intervals quantifying the
using Bayesian Information Criterion (BIC) as model selec- uncertainty associated with all estimated edges are presented
tion criterion. Overall model fit was judged using the fol- in the online supplementary Tables S2—S4.
lowing relative fit indexes: Comparative Fit Index (CFI),
Tucker Lewis Index (TLI) and Root Mean Square Error of Cross‑Sectional Teacher‑Reported Networks
Approximation (RMSEA) with CFI > 0.90, TLI > 0.90 and
RMSEA < 0.05 used as cut off criteria indicating reason- Networks based on teacher-reports showed similar patterns
ably good fit (Kline, 2005). Due to computational limitation, to parent-reports with symptoms from the same domains
bootstrapping routines could not be employed for the GVAR forming distinct clusters (see Fig. 1). In line with the parent-
model. Unfortunately, replicating the parent-reported GVAR reported networks, pairwise NCTs indicated that network
model using teacher-reported SBQs was also not possible structures and global network strength were invariant over
as GVAR estimations failed due to numerical optimiza- time (M7vs9 = 0.10. M7vs11 = 0.15, M9vs11 = 0.12; S7vs9 = 0.19,
tion issues likely caused by very high correlations (> 0.90) S7vs11 = 0.24, S9vs11 = 0.05). With regards to bridge symp-
between some teacher-reported SBQ items. Given the com- toms, teacher-reported networks also identified anxiety
putational complexity involved in fitting GVAR models, this item 2 (NER, Child is nervous, high-strung or tense) and
is not unexpected. ADHD items 12 (RES, Child cannot sit still, is restless, or
All estimated networks were visualised using the hyperactive) and 13 (FID, Child fidgets), as potential bridge
Fruchterman-Reingold algorithm in the qgraph package symptoms. However, they further highlighted a number of
which places nodes sharing stronger connections closer additional connections bridging the internalising and ADHD
together (Epskamp et al., 2012). For cross-sectional net- domains. In particular, item 2 (NER, Child is nervous, high-
works, the network layout was kept constant (using average strung or tense) was connected to all symptoms of the hyper-
layout of all networks) to facilitate comparisons. To iden- activity/impulsivity domain in the age 7 and age 9 networks,
tify the most influential bridge symptoms, bridge influence while only sharing edges with item 10 (IMP, Child is impul-
indices were estimated using the R package networktools, sive, acts without thinking) and 12 (RES, Child cannot sit
giving insights into the direct and indirect influence of spe- still, is restless, or hyperactive) in the age 11 network. The
cific bridge symptoms on symptoms from the other area of age 7 network further highlighted a connection between the
psychosocial functioning (Jones et al., 2019). inattention and depression domains through item 17 (INA,
Child is inattentive) and item 6 (NHA, Child is not as happy
as other children). At age 11, item 17 was connected to item
Results 8 (DIS, Child appears miserable, distressed, or unhappy)
instead of item 6. In addition, item 14 (CSE, Child cannot
Cross‑sectional Parent‑Reported Networks settle to anything for more than a few moments) shared an
edge with item 5 (DEP, Child seems to be unhappy, sad,
All parent-reported cross-sectional networks showed clus- or depressed). For bridge influence indices, see Table 2.
ters on the domain level with symptoms being more closely The higher connectivity of the teacher-reported networks
connected to other symptoms from their own domain than was also reflected in higher values for global network
131572 Research on Child and Adolescent Psychopathology (2021) 49:1567–1579
Fig. 1 Cross-sectional partial correlation networks for parent- and ous, ANX: anxious, WOR: worried; DEP: depressed, NHA: not as
teacher-reported symptoms at ages 7, 9, and 11. Green edges (solid happy as other children, TEN: trouble enjoying themselves, DIS: dis-
lines) indicate positive effects; red edges (dashed) indicate negative tressed, IMP: impulsive, DWA: difficulty awaiting turns, RES: rest-
effects. Upper row (a, b, c) represents parent-reported networks, less, FID: fidgets, CSE: cannot settle to anything, DTB: distractible,
lower row (d, e, f) represents teacher-reported networks. NER: nerv- CON: cannot concentrate, INA: inattentive
strength compared to parent-reported networks (S7=7.24, to edges bridging ADHD and internalising domains, hyper-
S9 = 7.43, S11 = 7.48). NCTs showed that these differences activity/impulsivity items 10 (IMP, Child is impulsive, acts
were significant at each time point (p < 0.001; DiffS7 = 1.27, without thinking) and 12 (RES, Child cannot sit still, is
DiffS 9 = 1.36, DiffS 11 = 1.22). Network structures were restless, or hyperactive) had positive temporal effects on
also found to be significantly different for parent- and internalising symptoms from the depression and anxiety
teacher-reported networks (p < 0.001; M7 = 0.30. M9 = 0.34, domains respectively, while items 15 (DTB, Child is dis-
M11 = 0.31). Similar to the parent-reported networks, estimates tractible, has trouble sticking to any activity) and 16 (CON,
for edges between bridge symptoms based on teacher-reports Child cannot concentrate, cannot pay attention for long)
were moderately stable. For confidence intervals, see Tables from the inattentive domain were associated with increased
S2 – S4 in supplementary materials. anxiety symptoms. Regarding the effects of internalising on
ADHD symptoms, item 4 (WOR, Child is worried) from the
Longitudinal Parent‑Reported Network anxiety domain had positive temporal effects on inattentive
ADHD symptoms and items 6 (NHA, Child is not as happy
The saturated parent-reported GVAR model showed good fit as other children), and 8 (DIS, Child appears miserable,
(CFI = 0.96, TLI = 0.95, RMSEA = 0.028 with 90% CI: 0.026 distressed, or unhappy) from the depression domain were
to 0.030). The regularised model performed slightly bet- associated with increased hyperactivity/impulsivity ADHD
ter than the saturated model (∆BIC = 1696.74; CFI = 0.94, symptoms. Interestingly, except for one direct link between
TLI = 0.93, RMSEA = 0.032 with 90% CI: 0.030 to 0.034). ADHD symptom 10 (IMP, Child is impulsive, acts without
Overall, the temporal network indicated that, at the within- thinking) and depression item 8 (DIS, Child appears mis-
person level, most symptoms affected other symptoms over erable, distressed, or unhappy), ADHD symptoms mostly
time, though symptoms shared more and stronger connec- had positive directional effects on anxiety items. These
tions with symptoms from the same domain. With regards in turn shared directional links with depression items,
13Research on Child and Adolescent Psychopathology (2021) 49:1567–1579 1573
Table 2 Bridge Influence Indices for Cross-Sectional Networks
Parent-Report: Age 7 Parent-Report: Age 9 Parent-Report: Age 11
Item Direct Influence Indirect Influence Direct Influence Indirect Influence Direct Influence Indirect Influence
02 0.21 0.33 0.09 0.15 0.13 0.20
03 - 0.03 - 0.01 - 0.02
04 - 0.04 - 0.02 - 0.03
05 - - - - - -
06 - - - - - -
07 - - - - - -
08 - - - 0.01 - 0.01
10 - - - 0.01 - 0.02
11 - - - - - -
12 0.11 0.20 - 0.04 - 0.06
13 0.09 0.18 0.09 0.13 0.13 0.18
14 - - - - - -
15 - 0.01 - 0.01 - -
16 - 0.01 - - - -
17 - - - - - -
Teacher-Report: Age 7 Teacher-Report: Age 9 Teacher-Report: Age 11
Item Direct Influence Indirect Influence Direct Influence Indirect Influence Direct Influence Indirect Influence
02 0.33 0.59 0.32 0.55 0.23 0.43
03 - 0.05 - 0.05 - 0.04
04 -.04 0.01 - 0.10 - 0.09
05 - 0.03 - - 0.04 0.09
06 0.05 0.08 - - - 0.02
07 - 0.02 - - - 0.01
08 - 0.01 - - 0.05 0.10
10 0.11 0.20 0.10 0.19 0.14 0.22
11 0.06 0.15 0.10 0.20 - 0.09
12 0.09 0.10 0.04 0.15 0.09 0.15
13 0.11 0.17 0.09 0.14 - 0.06
14 - 0.01 - 0.01 0.04 0.10
15 - 0.01 - 0.01 - 0.03
16 - 0.02 - - - 0.03
17 0.05 0.12 - 0.01 0.05 0.10
Bridge influence indices were derived from edge weights (partial correlations) in the respective cross-sectional network model. Direct influence:
sum of all edge weights that exist between a node X and all nodes that are not part of the same cluster as node X (i.e. either ADHD or internalis-
ing). Indirect influence: direct influence plus indirect effects of Node X through other nodes (e.g. indirect effect on node Z as in X—Y—Z)
indicating that anxiety symptoms potentially mediate the indicated that anxiety item 4 (WOR, Child is worried)
relations between ADHD and depression symptoms. Out of shared particularly many relations with items from both
all symptoms, bridge influence indices (Table 3) indicated ADHD domains, thus, suggesting that at the within-person
that ADHD item 12 (RES, Child cannot sit still, is restless, levels, children with higher symptoms of worrying also tend
or hyperactive) from the hyperactivity/impulsivity domain to have higher ADHD symptoms at the same time-point.
had the strongest direct influence on internalising symptoms, The between-person network (visualised in Figure S2, avail-
mainly from the anxiety domain, and internalising item 4 able online) indicated that children who have high scores
(WOR, Child is worried) from the anxiety domain had the on anxiety item 2 (NER, Child is nervous, high-strung or
strongest direct influence on ADHD symptoms, mainly from tense), tended to also have higher scores on hyperactive/
the inattention domain. The temporal within-person net- impulsive ADHD symptoms compared to children who had
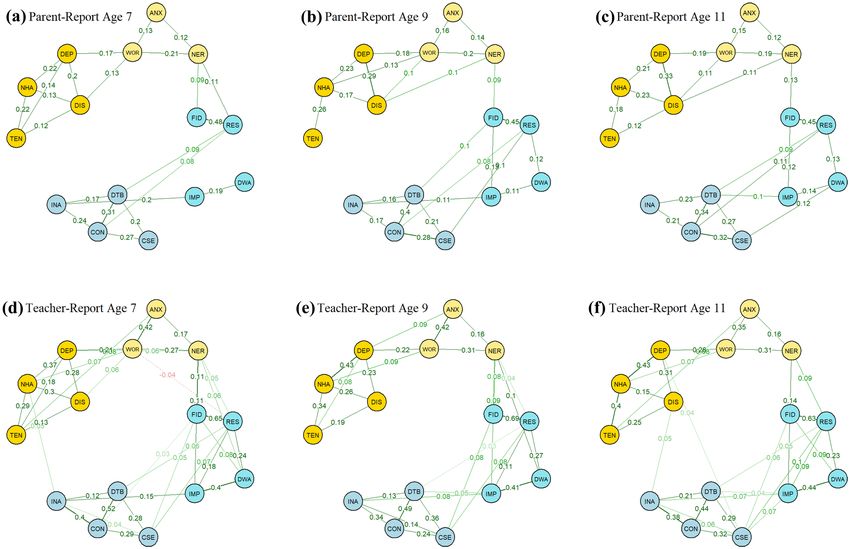
work is visualised in Fig. 2. The contemporaneous network, lower scores on item 2 (NER, Child is nervous, high-strung
which is visualised in Figure S1 in the online supplementary, or tense). Overall, the between-person network showed
131574 Research on Child and Adolescent Psychopathology (2021) 49:1567–1579
Table 3 Bridge Influence Indices for the Parent-Reported Temporal high-strung or tense’ from the anxiety domain. On the
GVAR Network temporal level, anxiety item ‘Child is worried’ was the
Item Out-Strength In-Strength Direct Influence Indirect strongest direct antecedent of higher ADHD symptoms
Influence and item ‘Child cannot sit still, is restless, or hyperactive’
was the strongest direct antecedent of higher internalising
02 - 0.10 - 0.03
symptoms.
03 - 0.06 - 0.02
In line with previous studies using cross-sectional
04 0.13 - 0.13 0.17
symptom networks (Beard et al., 2016; Silk et al., 2019),
05 0.04 - 0.04 0.09
our results indicated that items from the same domain (i.e.
06 0.09 - 0.09 0.12
anxiety, depression, hyperactivity/impulsivity, inattention)
07 - - - 0.01
formed relatively distinct clusters with internalising domains
08 0.06 0.05 0.06 0.07
and ADHD domains clustering more closely together. Nev-
10 0.06 - 0.05 0.07
ertheless, all cross-sectional networks highlighted that these
11 - - - -
internalising and ADHD symptom clusters are connected to
12 0.06 0.09 0.06 0.08
each other through items from the anxiety and the hyperac-
13 - 0.06 - 0.02
tivity/impulsivity domain, supporting the conceptualisation
14 - 0.06 - 0.01
of co-occurring psychopathology as connected networks of
15 0.05 - 0.05 0.11
symptoms. In particular, ADHD symptoms formed a bridge
16 0.05 0.07 0.05 0.08
to internalising symptoms through an association with how
17 - 0.04 - 0.01
often a child was nervous. Higher scores on items relating to
Bridge influence indices were derived from edge weights (partial cor- restlessness and fidgeting were associated with higher scores
relations) in the temporal GVAR model. Out-Strength: Sum of the on the nervousness item. Nervousness often goes hand in
absolute values of out-degree edge weights (i.e. edges with a direc-
tional arrow from node X to another node). In-Strength: Sum of the hand with restlessness, making it a plausible bridge symp-
absolute edge weights of in-degree edges (i.e. edges with a direc- tom between anxiety and ADHD. Also, the fact that restless-
tional arrow from another node to node X). Direct influence: sum of ness was part of the bridge to internalising problems is in
all edge weights that exist between a node X and all nodes that are line with DSM-5 diagnostic criteria which lists restlessness
not part of the same cluster as node X (i.e. either ADHD or inter-
nalising). Indirect influence: direct influence plus indirect effects as a symptom of both ADHD and anxiety disorders (Ameri-
of Node X through other nodes (e.g. indirect effect on node Z as in can Psychiatric Association, 2013).
X—> Y—> Z). Since, these networks are directed, influence meas- Whereas cross-sectional models revealed bridges between
ures only include out-degree edges symptom networks of ADHD and internalising problems,
longitudinal models allowed insights into directional within-
relatively little similarity with the within-person contempo- person relations between these symptoms over time. ‘Child
raneous and temporal network, highlighting the necessity cannot sit still, is restless, or hyperactive’ was found to
of appropriately disentangling within- from between-person have the strongest direct temporal influence on internalis-
effects when within-person effects are of primary interest as ing symptoms overall, with higher scores preceding an
in the context of mental health interventions. increase in the anxiety item ‘Child is too fearful or anx-
ious’ while some items from the inattentive ADHD domain
(‘Child is distractible, has trouble sticking to any activity’
Discussion and ‘Child cannot concentrate, cannot pay attention for
long’) preceded higher scores on the anxiety item ‘Child
In this study, we used graphical vector autoregression is nervous, high-strung or tense’. This suggests that, at the
models to investigate the development of ADHD and inter- within-person level, anxiety symptoms may be exacerbated
nalising symptom networks over time. This approach pro- by ADHD symptoms. Previous research has suggested that
vides an important advance over cross-sectional symptom the development of co-occurring anxiety could be related to
level networks as it allows for the estimation of directional the secondary effects of psychosocial difficulties associated
relations that can improve our understanding of the devel- with ADHD such as low educational achievement and social
opment of psychopathology and inform interventions. Our functioning deficits (Galéra et al., 2009). Consistent expo-
results highlighted a number of potential bridge symptoms sure to such difficulties has wide ranging negative effects and
between these areas of psychosocial functioning. On the has also been found to increase the risk of developing anxi-
cross-sectional level, ADHD and internalising symptoms were ety problems (Bishop et al., 2019; Mazzone et al., 2007).
primarily connected through item ‘Child cannot sit still, is Another contributing factor to the observed association of
restless, or hyperactive’ and item ‘Child fidgets’ from the restlessness preceding anxiety could be that restlessness is in
hyperactivity/inattention domain and ‘Child is nervous, fact an early sign of anxiety rather than an ADHD symptom
13Research on Child and Adolescent Psychopathology (2021) 49:1567–1579 1575
Fig. 2 Temporal network for parent-reported symptoms standard- enjoying themselves, DIS: distressed, IMP: impulsive, DWA: difficulty
ised to directed partial correlations. Green edges (solid lines) indi- awaiting turns, RES: restless, FID: fidgets, CSE: cannot settle to any-
cate positive effects. NER: nervous, ANX: anxious, WOR: worried; thing, DTB: distractible, CON: cannot concentrate, INA: inattentive
DEP: depressed, NHA: not as happy as other children, TEN: trouble
per se. Further research is needed to illuminate the reasons b). These findings are also consistent with the hypothesis
for these associations. that one reason why some individuals only develop ADHD
Examining the within-person longitudinal effects of inter- symptoms later in life is that these individuals have not been
nalising symptoms on ADHD symptoms, results suggested exposed to the same environmental risk load as those who
that the anxiety item ‘Child is worried, high-strung or tense’ develop symptoms early in life (Lunsford‐Avery & Kollins,
showed directional relations with inattentive symptoms. This 2018). These individuals showing increased ADHD symp-
indicates that internalising symptoms potentially aggravate tom following anxiety symptoms may already be at risk of
ADHD symptoms in middle childhood, adding to emerg- ADHD symptoms with anxiety acting as a triggering fac-
ing evidence that ADHD and internalising problems share tor. Another potential mechanism underlying the observed
reciprocal within-person relations (Murray et al., 2020a, temporal association of anxiety symptoms with inattentive
131576 Research on Child and Adolescent Psychopathology (2021) 49:1567–1579 symptoms is that anxiety inhibits the appropriate allocation Findings of the current study support current clinical best of working memory resources, negatively impacting execu- practice. In particular, results highlight the need for screen- tive functioning, and in turn leading to increased inattentive ing children who show high ADHD symptomatology also behaviour (Eysenck et al., 2007; Zainal & Newman, 2020). for internalising problems and vice versa, especially if they Similarly, the observed directional association may capture show symptoms of anxiety and for paying particular atten- the fact that worrying interferes with an individual’s concen- tion to the presence of bridge symptoms that may put a child tration, manifesting as inattention symptoms. at risk of the development or escalation of co-occurring Temporal within-person networks also highlighted rela- issues. Interventions such as Cognitive Behavioural Therapy tions between symptoms of depression and hyperactivity/ (CBT) may be particularly beneficial for children suffering impulsivity. In particular, over time, ‘Child is not as happy from both ADHD and internalising symptoms as symptoms as other children’ or ‘Child appears miserable, distressed, such as worrying, which was found to bridge these two men- or unhappy’ was associated with increases in symptoms tal health domains, have been found to respond very well to relating to restlessness and fidgeting. This finding is con- CBT (Barrett et al., 2001). Intervention studies have further sistent with the exacerbation hypothesis which proposes shown that targeting anxiety symptoms with CBT also leads that children high on ADHD and internalising symptoms, to a reduction in ADHD symptoms (Gould et al., 2018), thus usually anxiety, display more severe behavioural symptoms showing promise for reducing the co-occurrence of ADHD due to the combined effect of impairments in inhibitory con- and internalising problems. trol associated with both difficulties (Becker et al., 2012). Alternatively, the observed associations could also simply reflect the fact that depression is sometimes accompanied Limitations and Future Directions by a state of agitation which manifests in symptoms such as restlessness (Winstanley et al., 2006). Our results fur- The main limitation of this study is that our measure of ther suggest that within-person links between depression ADHD and internalising problems relied on relatively few items and ADHD are mostly mediated through difficulties items, allowing only limited inference on bridge symptoms in the anxiety domain as, apart from impulsivity showing an between these areas of psychosocial functioning. Future stud- association with increased distress, ADHD symptoms only ies should use a broader range of symptoms and ideally the had indirect temporal effects on depression through anxiety full set of DSM-5 symptoms for ADHD and internalising symptoms. This is in line with previous research on the rela- disorders to investigate the development of their symptom tions between depression and ADHD which has found that networks over time. Also, results of the current study are their relation is often mediated through anxiety and disrup- based on a community sample and consequently might not tive behaviour disorders (Roy et al., 2014). generalise to clinical populations. While using community Finally, the longitudinal within-person network also high- samples has some important advantages, such as minimis- lighted some potentially revealing relations between differ- ing the risk for Berkson’s bias (i.e. the overestimation of ent ADHD symptoms. In particular, the two impulsivity symptom co-occurrence; Berkson, 1946), future studies have items, ‘Child is impulsive, acts without thinking’ and ‘Child to be conducted to investigate whether the observed rela- has difficulty awaiting turn in games or groups’, were only tions would unfold differently for children at the clinical indirectly connected through the item ‘Child is distractible, end of the spectrum. Further, the current study relied on has trouble sticking to any activity’. Considering that the estimating associations between individual symptoms meas- GVAR model is based on partial correlations, this indicates ured by single-items, which means that measurement error that any relation between the two impulsivity items may be was likely greater than when using a composite of multiple better explained by their shared relation with distractibility. items. Future research should investigate the reliability of Specifically, the directional effects suggest that increased these single-item measurements and ideally use a multi-item impulsivity may lead to higher distractibility symptoms measure of individual symptoms. In addition, some meth- which might subsequently increase difficulties with awaiting odological considerations need to be addressed in future turns. Another reason why the impulsivity items were not research. While we were able to show that cross-sectional directly connected could be that impulsivity is multi-faceted networks were fairly similar between parent- and teacher- and these two items may capture different forms of impul- reports, we were not able to replicate the longitudinal symp- sivity that are based on distinct underlying deficits. Difficul- tom network using the teacher-reported data as the high col- ties awaiting turns is likely closely related to delay aversion linearity between some of the SBQ items led to estimation which has been associated with temporal processing deficits difficulties. Further, the GVAR model was exploratory in in ADHD whereas the more general ‘Child is impulsive, acts nature and will need to be replicated in independent data. without thinking’ item might capture more fundamental dif- The development of confirmatory longitudinal network mod- ficulties with inhibitory control (Winstanley et al., 2006). els will be important to enable testing of the replicability of 13
Research on Child and Adolescent Psychopathology (2021) 49:1567–1579 1577
longitudinal networks because concerns have been raised Acknowledgements The authors are grateful to the children, parents
regarding their stability (Jordan et al., 2020). and teachers who provided data for the z-proso study and the research
assistants involved in its collection.
In terms of other future directions, it will be valuable to
extend the symptom networks to range from childhood to Authors’ Contributions LGS conceptualized and designed the study,
adolescence and into adulthood in order to provide a compre- conducted analyses, drafted the initial manuscript, and reviewed and
hensive picture of ADHD and internalising symptom rela- revised the manuscript. ME and DR made substantial contributions
tions over the lifespan. In addition, future studies should also to the conception and design of the study and to the acquisition of
data and critically reviewed the manuscript for important intellectual
include features associated with a broader ADHD phenotype content. ALM, ML, and BA made substantial contributions to the
in their analyses. In particular, emotional dysregulation and conception and design of the study and critically reviewed the manu-
sluggish cognitive tempo have been identified as potential script for important intellectual content. All authors approved the final
mediators between symptoms of ADHD and internalising manuscript as submitted and agree to be accountable for all aspects
of the work.
problems (Anastopoulos et al., 2011; Sevincok et al., 2020).
Due to sample size constraints, the current study did not Funding The Zurich Project on Social Development from Childhood
investigate whether factors such as child gender, ADHD to Adulthood is supported by the Jacobs Foundation and the Swiss
subtype or symptom severity might lead to symptom net- National Science Foundation. This work was further supported by
works unfolding differently concurrently and temporally. the University of Edinburgh (LGS, Principal’s Careers Development
Scholarship); the European Union’s Horizon 2020 research and inno-
This would be valuable to explore in future research using vation programme (BA, Marie Skłodowska-Curie grant agreement
methods such as moderated network analyses (Haslbeck No.813546); the Baily Thomas Charitable Fund (BA, TRUST/VC/AC/
et al., 2019). Finally, future research should also investi- SG/469207686); and the UK Economic and Social Research Council
gate whether psychological or pharmacological treatments (BA, ES/N018877/1).
for ADHD or internalising symptoms have an effect on the
Availability of Data and Material Data available upon request.
overall network structure and especially on edges between
ADHD and internalising symptoms. Some evidence from Code Availability Code available upon request.
intervention studies suggests that treatment of anxiety and
ADHD leads to a greater reduction in symptoms for concur- Declarations
rent anxiety and hyperactive/impulsive symptoms than for
concurrent anxiety and inattentive symptoms (Jarrett, 2013). Ethical Approval The authors assert that all procedures contributing
This is in line with results from our cross-sectional networks to this work comply with the ethical standards of the relevant national
which suggest that anxiety shares closer links with hyper- and institutional committees on human experimentation and with the
Helsinki Declaration of 1975, as revised in 2008.
activity/impulsivity symptoms than inattentive symptoms.
Thus, these preliminary results highlight that investigating
Conflicts of Interest The authors have no conflicts of interest relevant
the effects of treatments on symptom networks could pave to this article to disclose.
the way for developing interventions that reduce the chances
of developing co-occurring symptoms of ADHD or inter- Informed Consent Parents provided active informed consent for chil-
nalising problems by targeting specific bridge symptoms. dren to participate in the study.
Open Access This article is licensed under a Creative Commons Attri-
bution 4.0 International License, which permits use, sharing, adapta-
Conclusion tion, distribution and reproduction in any medium or format, as long
as you give appropriate credit to the original author(s) and the source,
This study offered unique insights into the developmental provide a link to the Creative Commons licence, and indicate if changes
were made. The images or other third party material in this article are
relations of internalising and ADHD symptoms. Results included in the article’s Creative Commons licence, unless indicated
of cross-sectional and within-person longitudinal analy- otherwise in a credit line to the material. If material is not included in
ses highlight that ADHD shares reciprocal relations with the article’s Creative Commons licence and your intended use is not
internalising symptoms through a number of potential permitted by statutory regulation or exceeds the permitted use, you will
need to obtain permission directly from the copyright holder. To view a
bridge symptoms that are primarily connected to symp- copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
toms from the anxiety domain. Future studies are needed
to better understand the mechanisms through which ADHD
and internalising symptoms affect each other and to evalu-
ate the feasibility of targeting specific bridge symptoms in References
interventions.
American Psychiatric Association. (2013). Diagnostic and Statistical
Supplementary Information The online version contains supplemen- Manual of Mental Disorders. American Psychiatric Association.
tary material available at https://d oi.o rg/1 0.1 007/s 10802-0 21-0 0856-3. https://doi.org/10.1176/appi.books.9780890425596
131578 Research on Child and Adolescent Psychopathology (2021) 49:1567–1579
Anastopoulos, A. D., Smith, T. F., Garrett, M. E., Morrissey-Kane, Epskamp, S., Waldorp, L. J., Mõttus, R., & Borsboom, D. (2018b). The
E., Schatz, N. K., Sommer, J. L., et al. (2011). Self-regulation of Gaussian Graphical Model in Cross-Sectional and Time-Series
emotion, functional impairment, and comorbidity among children Data. Multivariate Behavioral Research, 53(4), 453–480. https://
with AD/HD. Journal of Attention Disorders, 15(7), 583–592. doi.org/10.1080/00273171.2018.1454823
https://doi.org/10.1177/1087054710370567 Eysenck, M. W., Derakshan, N., Santos, R., & Calvo, M. G. (2007,
Barrett, P. M., Duffy, A. L., Dadds, M. R., & Rapee, R. M. (2001). May). Anxiety and cognitive performance: Attentional control
Cognitive-behavioral treatment of anxiety disorders in children: theory. Emotion. https://doi.org/10.1037/1528-3542.7.2.336
Long-term (6-year) follow-up. Journal of Consulting and Clinical Funkhouser, C. J., Chacko, A. A., Correa, K. A., Kaiser, A. J. E.,
Psychology, 69(1), 135–141. https://doi.org/10.1037/0022-006X. & Shankman, S. A. (2020). Unique longitudinal relationships
69.1.135 between symptoms of psychopathology in youth: A cross‐lagged
Beard, C., Millner, A. J., Forgeard, M. J. C., Fried, E. I., Hsu, K. J., panel network analysis in the ABCD study. Journal of Child Psy-
Treadway, M. T., et al. (2016). Network analysis of depression chology and Psychiatry, jcpp.13256. https://d oi.o rg/1 0.1 111/j cpp.
and anxiety symptom relationships in a psychiatric sample. Psy- 13256
chological Medicine, 46(16), 3359–3369. https://d oi.o rg/1 0.1 017/ Galéra, C., Melchior, M., Chastang, J. F., Bouvard, M. P., & Fombonne,
S0033291716002300 E. (2009). Childhood and adolescent hyperactivity-inattention
Becker, S. P., Luebbe, A. M., Stoppelbein, L., Greening, L., & Fite, symptoms and academic achievement 8 years later: The GAZEL
P. J. (2012). Aggression among children with ADHD, anxiety, Youth study. Psychological Medicine, 39(11), 1895–1906. https://
or co-occurring symptoms: Competing exacerbation and attenu- doi.org/10.1017/S0033291709005510
ation hypotheses. Journal of Abnormal Child Psychology, 40(4), Gnanavel, S., Sharma, P., Kaushal, P., & Hussain, S. (2019, Septem-
527–542. https://doi.org/10.1007/s10802-011-9590-7 ber 1). Attention deficit hyperactivity disorder and comorbid-
Berkson, J. (1946). Limitations of the Application of Fourfold Table ity: A review of literature. World Journal of Clinical Cases.
Analysis to Hospital Data. Biometrics Bulletin, 2(3), 47. https:// Baishideng Publishing Group Co. https://d oi.o rg/1 0.1 2998/
doi.org/10.2307/3002000 wjcc.v7.i17.2420
Berry, D., & Willoughby, M. T. (2017, July 1). On the Practical Inter- Gould, K. L., Porter, M., Lyneham, H. J., & Hudson, J. L. (2018).
pretability of Cross-Lagged Panel Models: Rethinking a Devel- Cognitive-behavioral therapy for children with anxiety and comor-
opmental Workhorse. Child Development. Blackwell Publishing bid attention-deficit/hyperactivity disorder. Journal of the Ameri-
Inc. https://doi.org/10.1111/cdev.12660 can Academy of Child and Adolescent Psychiatry, 57(7), 481-490.
Bishop, C., Mulraney, M., Rinehart, N., & Sciberras, E. (2019, March e2. https://doi.org/10.1016/j.jaac.2018.03.021
1). An examination of the association between anxiety and social Hamaker, E. L., Kuiper, R. M., & Grasman, R. P. P. P. (2015). A cri-
functioning in youth with ADHD: A systematic review. Psychiatry tique of the cross-lagged panel model. Psychological Methods,
Research. Elsevier Ireland Ltd. https://d oi.o rg/1 0.1 016/j.p sychr es. 20(1), 102–116. https://doi.org/10.1037/a0038889
2019.01.039 Haslbeck, J. M. B., Borsboom, D., Waldorp, L. J. (2019). Moderated
Borsboom, D. (2008). Psychometric perspectives on diagnostic sys- Network Models Multivariate Behavioral Research 1–32 https://
tems. Journal of Clinical Psychology, 64(9), 1089–1108. https:// doi.org/10.1080/00273171.2019.1677207
doi.org/10.1002/jclp.20503 Jarrett, M. A. (2013). Treatment of comorbid attention-deficit/hyper-
Borsboom, D., & Cramer, A. O. J. (2013, March 28). Network analy- activity disorder and anxiety in children: Processes of change.
sis: An integrative approach to the structure of psychopathology. Psychological Assessment, 25(2), 545–555. https://doi.org/10.
Annual Review of Clinical Psychology. Annual Reviews. https:// 1037/a0031749
doi.org/10.1146/annurev-clinpsy-050212-185608 Jarrett, M. A., & Ollendick, T. H. (2008, October 1). A conceptual
Eisner, M., & Ribeaud, D. (2007). Conducting a Criminological Survey review of the comorbidity of attention-deficit/hyperactivity dis-
in a Culturally Diverse Context. European Journal of Criminol- order and anxiety: Implications for future research and practice.
ogy, 4(3), 271–298. https://doi.org/10.1177/1477370807077183 Clinical Psychology Review. Pergamon. https://d oi.o rg/1 0.1 016/j.
Eisner, N. L., Murray, A. L., Eisner, M., & Ribeaud, D. (2019). A cpr.2008.05.004
practical guide to the analysis of non-response and attrition in lon- Jones, P. J., Ma, R., McNally R. J. (2019). Bridge Centrality: A
gitudinal research using a real data example. International Journal Network Approach to Understanding Comorbidity Multivariate
of Behavioral Development, 43(1), 24–34. https://d oi.o rg/1 0.1 177/ Behavioral Research 1–15. https://doi.org/10.1080/00273171.
0165025418797004 2019.1614898
Enders, C. K. (2001). The performance of the full information maxi- Jordan, D. G., Winer, E. S., & Salem, T. (2020). The current status
mum likelihood estimator in multiple regression models with of temporal network analysis for clinical science: Considerations
missing data. Educational and Psychological Measurement, as the paradigm shifts? Journal of Clinical Psychology, 76(9),
61(5), 713–740. https://doi.org/10.1177/00131640121971482 1591–1612. https://doi.org/10.1002/jclp.22957
Epskamp, S. (2020). Psychometric network models from time-series Kessler, R. C., Berglund, P., Demler, O., Jin, R., Merikangas, K. R., &
and panel data. Psychometrika, 85(1), 206–231. https://doi.org/ Walters, E. E. (2005, June 1). Lifetime prevalence and age-of-onset
10.1007/s11336-020-09697-3 distributions of DSM-IV disorders in the national comorbidity sur-
Epskamp, S., Borsboom, D., & Fried, E. I. (2018a). Estimating psy- vey replication. Archives of General Psychiatry. American Medical
chological networks and their accuracy: A tutorial paper. Behav- Association. https://doi.org/10.1001/archpsyc.62.6.593
ior Research Methods, 50(1), 195–212. https://doi.org/10.3758/ Kline, R. B. (2005). Principles and Practice of Structural Equation
s13428-017-0862-1 Modeling, Second Edition. Guilford Publications. https://books.
Epskamp, S., Cramer, A. O. J., Waldorp, L. J., Schmittmann, V. D., & google.at/books?id=EkMVZUxZrgIC
Borsboom, D. (2012). Qgraph: Network visualizations of relation- Lubke, G. H., Hudziak, J. J., Derks, E. M., van Bijsterveldt, T. C. E.
ships in psychometric data. Journal of Statistical Software, 48(4), M., & Boomsma, D. I. (2009). Maternal Ratings of Attention
1–18. https://doi.org/10.18637/jss.v048.i04 Problems in ADHD: Evidence for the Existence of a Contin-
Epskamp, S., & Fried, E. I. (2018). A tutorial on regularized partial uum. Journal of the American Academy of Child and Adolescent
correlation networks. Psychological Methods, 23(4), 617–634. Psychiatry, 48(11), 1085–1093. https://doi.org/10.1097/CHI.
https://doi.org/10.1037/met0000167 0b013e3181ba3dbb
13You can also read