Focal Laser Ablation for Localized Prostate Cancer
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
JOURNAL OF ENDOUROLOGY
Volume 24, Number 5, May 2010
ª Mary Ann Liebert, Inc.
Pp. 791–797
DOI: 10.1089=end.2009.0440
Focal Laser Ablation for Localized Prostate Cancer
Uri Lindner, M.D., Nathan Lawrentschuk, M.D., and John Trachtenberg, M.D.
Abstract
Throughout history, medicine has witnessed paradigm shifts that significantly change patient treatment. In
surgical oncology, the introduction of lumpectomy revolutionized breast cancer treatment while partial ne-
phrectomy has altered the management of kidney cancer. In both cases, organ preservation is combined with
efficacious management of the cancer via a less invasive approach. Within urology, prostate cancer (PCa) may be
the next to benefit from such a treatment paradigm. Current management of PCa involves either whole organ
treatment, with the inherent side effects, while selected patients are eligible for active surveillance. Focal therapy
offers a middle ground for low-risk patients with PCa, again using the principles of a minimally invasive
treatment of the cancer, in this case using an energy source with few side effects, combined with maximal organ
preservation. Because focal therapy for PCa is still in evolution, there is no consensus on the ideal energy source
that should be used to ablate the PCa, imaging to monitor the tissue destruction in real time, how many
treatments may be offered, and the ideal follow-up regimen. Long-term follow-up of patients is needed before it
is recommended as a first-line treatment. Nevertheless, evidence is accumulating that radically treating PCa
holds survival benefit for patients; however, the number of men needed to treat is considerable, with significant
side effects; thus, more centers are investigating focal therapy as an option. This review focuses on the use of the
laser as the energy source for focal ablation, while bringing historically relevant information regarding laser
energy and highlighting the perceived advantageous of focal laser ablation.
Focal Therapy as a Treatment Strategy and an increase in survival without metastasis (76.9% vs
in Prostate Cancer 54.4%)7,12 The European Randomized Study of Screening for
Prostate Cancer has also demonstrated a 20% reduction in
P rostate cancer (PCa) is the most common, non-
cutaneous human malignancy with almost 200,000 new
cases diagnosed in 2008 in the United States.1 Autopsy studies
PCa disease-specific mortality for patients who were screened
and treated with whole-gland radical therapies.13 All avail-
able whole-gland treatments, however, exert a significant
have demonstrated PCa in 40% of men aged 60 years, in- negative impact on patient health-related quality of life
creasing up to 70% by age 80 years. The lifetime risk of clin- (QoL).14,15
ically significant and fatal prostate cancer of a 50-year-old To combat potential overtreatment of clinically insignificant
man, however, is estimated to be only 9.5% and 2.9%, re- cancer, active surveillance (AS) has emerged as an alternative
spectively.2 management strategy.16 Patients who are suspected of having
With current trends of prostate-specific antigen (PSA) insignificant PCa based on physical examination, PSA levels,
screening and the lowered PSA threshold for biopsy, 45% to and transrectal ultrasonographic-guided biopsy (TRUS-BX)
85% of patients fall under the category of low-risk prostate results are actively monitored, with radical treatment offered
cancer (PSA < 10 ng=mL, Gleason 3 þ 3, clinical T1c–T2a).3–5 It when suspicion of progressive or life-threatening clinically
is estimated that 25% to 84% of patients with PCa who are significant disease emerges. Such information is based on re-
currently being treated will not succumb to their disease peated physical examinations, PSA (rise or kinetics), and
should they be left untreated; thus, this is known as insig- TRUS-BX. Thus AS offers curative treatment to patients who
nificant disease.6–11 we suspect ultimately need it while it avoids inflicting un-
Although we risk overtreating a large subset of patients, wanted side affects in patients who do not need treatment
proponents for active treatment have evidence from the because of insignificant disease.16
Scandinavian trial. This demonstrated a decrease in cancer- Although AS is theoretically appealing, data are emerging
specific mortality for patients who underwent radical pros- that suggest a considerable proportion of patients offered AS
tatectomy (RP) rather than watchful waiting (12.5% vs 17.9%) may indeed be harboring significant PCa. In a series of men
Department of Surgical Oncology, Princess Margaret Hospital, University Health Network, University of Toronto, Toronto, Canada.
791792 LINDNER ET AL.
who were offered AS with selective delayed therapy, a large focused light beams. The first principle of quantum theory
number of those patients who ultimately underwent RP were postulates that light travels in packets of energy known as
found to have advanced disease. Extraprostatic extension photons. The second principle postulates that most atoms or
occurred in 58% while 8% had nodal disease.17 molecules exist in a low-energy-state. It is possible to add
Individual risk of disease progression is difficult to assign, energy to atoms in the ground state to convert the majority of
so of concern is a small but real possibility of progression to low energy atoms to higher energy levels. The energy then is
death in the AS population because of the loss of opportunity released spontaneously in the form of photons or electro-
for cure during the surveillance period. Further, although AS magnetic waves to return to the ground state. Einstein also
may appear to have no morbidity, several studies have shown postulated that when a photon of light energy of the same
deterioration of QoL18–20 and even deterioration in sexual wavelength strikes an excited atom, that photon and the pho-
function.21,22 Finally, although AS has gained popularity, it is ton of light that is released are discharged simultaneously
still infrequently used. In the United States, approximately and therefore will be identical in frequency and phase. This is
10% of eligible men are put on AS protocols,23 and even in the concept of stimulated emission used in the creation of a
countries where AS is largely accepted, only 30% of eligible laser.
men are on AS.24 Patients and=or their physicians appear to The physical aspects of a laser system are dictated by its
want to treat the PCa once diagnosed. wavelength, and the wavelength of the laser is dictated by the
Currently, the accepted options for treating patients with source that is being excited. The first commercial laser built in
low-risk PCa lie between radical whole-gland treatment 1960 by Maiman31 used a synthetic ruby as a source of exci-
(surgery, external-beam radiation, or brachytherapy) and AS. tation. The first generations of lasers used various forms of gas
Each has merits and disadvantages. Focal therapy is different as excitation mediums such as N2–CO2 and helium-neon. The
and may be likened to a lumpectomy in breast cancer where second generation of lasers used liquid materials as forms of
only the diseased part of the organ is targeted with minimal excitation and are called dye lasers because they use an or-
impact on the surrounding normal organ. Hence, Onik25 ganic dye as the excitation medium, usually as a liquid solu-
coined the term ‘‘male lumpectomy’’ for focal ablation of tion. Compared with gases and most solid state lasing media,
PCa. a dye can usually be used for a much wider range of wave-
Certainly, one may consider focal therapy as a logical ex- lengths. The wide bandwidth makes them particularly suit-
tension of the AS concept; it has a low risk for lifestyle-altering able for tunable lasers and pulsed lasers. Moreover, the dye
complications associated with whole-gland treatment but also can be replaced by another type to generate different wave-
aims to achieve cancer control at the outset. This is possible lengths with the same laser, making dye lasers very versatile.
because PCa, although multifocal in a majority of cases, is In addition to their recognized wavelength agility these lasers
considered to have an index cancer,26 which is the one most can offer large pulsed energies or very high average powers.32
likely to cause extraprostatic extension and ultimately disease In 1970, the first continuous-wave dye laser, being argon
spread. Focal therapy relies on imaging to identify such a pumped, was developed. The output of a laser may be a
clinically threatening index cancer and treat it, and in doing so continuous constant-amplitude output (continuous wave) or
minimize the risk of progression associated with expectant pulsed, In the pulsed mode of operation, the output of a laser
management in AS patients. varies with respect to time, typically taking the form of al-
At present, three major energy sources have been used in ternating ‘‘on’’ and ‘‘off’’ periods. This application facilitates
focal therapy: Cryoablation,25,27,28 high-intensity focused ul- the depositing of as much energy as possible at a given place
trasound (HIFU),29 and laser ablation.30 We will now outline in as short a time as possible.
the physiology behind laser ablation and emphasize the ad- The medical field was quick to realize the possibilities in
vantages and disadvantages in using laser energy to perform laser energy; only 3 years after the first commercial laser was
focal therapy for PCa. built, McGuff and associates33 reported on the effect of a ruby
laser on melanoma cells transplanted in hamsters. Many more
studies that examined the use of laser energy for treating
History of the Laser
patients with cancer soon followed.34–38 Laser energy was
Laser is an acronym for Light Amplification by Stimulated quickly adapted for tissue welding, coagulation, and impor-
Emission of Radiation and was under legal dispute as to its tantly, tissue ablation.39–41
origins, but Gordon Gould in 1957 is now credited. The basic
process involves exciting a particular material by an external
Focal Laser Ablation
source (light, electricity, chemical reaction). The material is
placed between two mirrors that act as an optical resonator, The term laser ablation refers to the thermal destruction of
which intensifies the interaction between the electromagnetic tissue by laser. There are differing names for laser ablation,
field and the excited material (amplification). Making one of including photothermal therapy, laser interstitial tumor
the mirrors partly transparent allows the resulting laser beam therapy, and laser interstitial photocoagulation.42 The term
to exit the resonator. Depending on the material used, a dif- interstitial laser ablation reflects the fact that the laser fiber is
ferent wavelength will be generated. inserted into the tissue as opposed to ablating tissue with a
Laser radiation has three important characteristics: It is laser while maintaining a buffer medium between the fiber
coherent (the wave trains are exactly in phase), it is collimated emitting the energy and the tissue being ablated (eg, air for
(the beam is parallel), and it is monochromatic (all the photons cutaneous application, saline when applying laser energy in the
have the same wavelength, frequency, and energy). Albert bladder=ureter). We prefer the term focal laser ablation (FLA)
Einstein theorized about a laser in a 1917 publication on when referring to the treatment of PCa as it describes the
quantum theory that postulated the phenomenon of extremely intention and the treatment.FOCAL LASER ABLATION OF PROSTATE CANCER 793
to a very efficient energy transfer and heating of the tissue when
irradiated with lasers of these wavelengths (eg, CO2 laser).
Evidence is accumulating that laser energy penetrates
tumor cells better than normal tissue44 and thus enables larger
coagulation zones in tumors. The laser most commonly used
for FLA is the Nd-YAG laser, with a wavelength of 1064 nm,
but it is being replaced by more compact and less expensive
infrared (800–980 nm) diode lasers. The delivered photons
induce an increase in temperature. Local tissue temperatures
above 608C cause rapid coagulative necrosis and instant cell
death, but irreversible cell death can also be achieved at lower
hyperthermic temperatures (>428C), although longer dura-
tions are necessary.45,46 Temperatures above 1008C will cause
FIG. 1. Contrast enhanced ultrasonographic image shows vaporization of cellular protoplasm, followed by desicca-
an ablation real time. tion and shrinkage of the tissue; afterward, any additional
laser energy causes a quick temperature rise, and tempera-
tures above 3008C cause the tissue to burn and carbonization
Interstitial laser ablation was first described by Bown in occurs.
1983.43 He inserted a 400 mm glass fiber into a metastatic skin Since the first deployment of interstitial FLA in 1983 by
lesion and, using an neodymium:yttrium-aluminum-garnet Bown,43 many modifications have been made. The applica-
(Nd:YAG) laser system and deploying a bare fiber, caused tion of the laser beam via flexible quartz fibers of diameters
local necrosis in the treated area The basic principles behind from 250 to 1000 mm allows FLA through flexible fiberoptic
laser ablation are the conversion of laser light into heat by devices and through thin needles.
tissue. The optical and thermal properties of the tissue as well The use of specially designed interstitial fiberrs, which are
as the parameters of the laser beam influence the extent of the quartz fibers that have flat or cylindrical diffusing tips and are
thermal ablation. The optical and thermal properties of the 10 to 40 mm long, provide a much larger ablative area of up to
tissue are determined by the structure, water content ,and 50 mm.
blood circulation. The key concepts are absorption, scattering, Increasing laser power output in newer lasers allows for
reflection, thermal conductivity, and heat capacity. better light transmission and larger ablative zones. It also
The prostate as a tissue is suited for FLA because of its causes increased local temperature rise close to the laser fiber,
optical absorption rate without excess vascularity, which however, risking overheating and carbonization of the adja-
causes heat conduction and limits the ablation size when cent tissue. Carbonization of tissue decreases optical pene-
performing FLA in highly vascularized tissues such as liver. tration and heat conduction and limits the size of the lesion
The laser beam properties are governed by the wavelength, produced.
power, and density. The main absorption of biologic molecules To limit such events and to prevent overheating close to the
occurs within the range of a wavelength shorter than about fiber tip, water-cooled laser application sheaths are being
280 nm (ultraviolet). The penetration of light is optimal at used. They allow for higher laser power output (up to 50 W
wavelengths longer than 1 mm (the near-infrared range of the compared with 5 W) while preventing carbonization.47,48
spectrum). The high water content (60%–80%) of most tissue Thus, the use of multiple water-cooled higher power fibers
leads to an extensive absorption of infrared radiation and thus allows ablative zones of up 80 mm in diameter.
Table 1. Laser Ablation for Nonprostate Cancer Tumors
Author Organ Tumor n Imaging modality Complete ablation
Pacella52 Liver HCC 432 US 78.2%
Vogl50 Liver Met. colorectal cancer 603 Insertion CT Monitoring 96.3%–98.8%
MRI
Puls59 Liver Met. colorectal cancer 87 Insertion CT Monitoring 85.6%
MR
Schwarzmaier60 Brain Glioblastoma 16 MRI N=A
Leonardi61 Brain Glioma 24 MRI N=A
Carpentier62 Brain Met. 4 MRI N=A
Papini63 Thyroid ‘‘Cold’’ nodule 62 US 33% strict criteria
Amabile64 Thyroid ‘‘Cold’’ nodule 23 US 91%
Mack65 Abdomen Met. 11 MRI 71%
Rosenberg66 Lung Met 64 CT 78%
Gangi67 Bone Osteoid osteoma 114 CT 98%
Streitparth68 Bone Osteoid osteoma 1 MRI 100%
Dick69 Kidney RCC 9 MRI N=A
Van Esser70 Breast Invasive breast cancer 14 US 57%
HCC ¼ hepatocellular carcinoma; US ¼ ultrasonography; Met. ¼ metastases; CT ¼ computed tomography; MRI ¼ magnetic resonance
imaging; N=A ¼ not available; RCC ¼ renal-cell carcinoma.794 LINDNER ET AL.
Perhaps the most exciting innovation is the ability to nearby vital structures. CEUS is well suited for FLA as well;
monitor in real time the lesion created by the laser using im- because the thermal effects created by the ablation reduce
aging techniques, such as magnetic resonance (MR) ther- blood perfusion significantly, there is no uptake of micro-
mometry and contrast-enhanced ultrasonogrphy (CEUS). bubbles in the ablated area. Thus, the treatment effect in tissue
Because FLA is highly compatible with MR and does not is evident by the absence of CEUS signal, with obvious de-
cause any electromechanical disturbances, the use of MR lineation between viable and nonviable tissue (Fig. 1).49
thermometry allows for real-time monitoring of lesion size
and allows for individually adjusted heat dosing application Focal Laser Ablation for Tumors Other
ensuring adequate tumor ablation while avoiding damage to than the Prostate
Ever since the advent of FLA in 1983 by Bown,43 there have
been numerous studies regarding the effectiveness of FLA for
tumors (eg, unresectable liver metastasis and inoperable he-
patocellular carcinoma [HCC] treatment). In a large non-
randomized study, Vogl and colleagues50 treated 1801
colorectal cancer liver metastasis in 603 patients with MR
image-guided FLA. Local tumor control rates of above 96% at
6 months based on MR imaging were achieved, with an
overall complication rate of 1.5% and a 30-day mortality of
0.1%. No tumor seeding was noted, and a median survival of
4.4 years after diagnosis of metastases was achieved, being
superior to the 17.4 months median survival after receiving
chemotherapy alone.
Several contemporary studies of outcomes of FLA for in-
operable HCC have achieved acceptable complete ablation
rates of 82% to 97.5% with tumors smaller than 3 cm, and from
60% to 82% in tumors 3 to 4 cm.51,52 Mortality is very low
considering the patient population at 0.1% to 0.2% and major
complications around 1.5%.51,52 When compared with radio-
frequency ablation and HIFU, FLA was shown to be equiva-
lent and less morbid.53
In summary, FLA has been performed on a variety of dif-
ferent tumors with encouraging results (Table 1) and is
gaining popularity as an image-guided, MR-controlled lo-
calized tumor ablation modality.
Focal Laser Ablation for Low-Risk Prostate Cancer
Currently, all the studies being published in focal therapy
for low-risk PCa are nonrandomized, small cohorts, and
phase I clinical trials. Focal therapy for PCa, however, appears
to be gaining acceptance and holds promise for a better bal-
ance between cancer control and morbidity.
In a recent phase I clinical trial by our group,30 we per-
formed image-guided FLA for patients with low-risk PCa.
The enabling technology for targeted FLA as opposed to
hemiablation or subtotal gland ablation is accurate imaging.
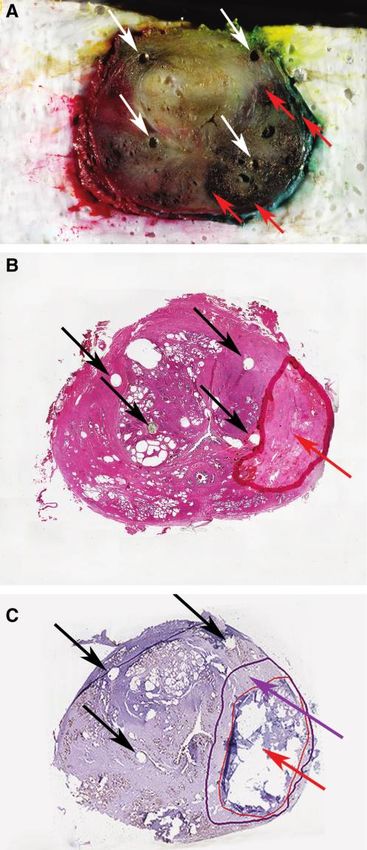
FIG. 2. Pathologic confirmation of ablation. (A) Gross pa-
thology view. Prostate colored red on the right side, green on
the left, and yellow anterior. White arrows indicate fiducial
markers that were placed ex-vivo to correlate pathology and
imaging. Red arrows indicate the borders of the visible ab-
lated area. (B) Hematoxylin and eosin stain of the prostate.
Black arrows indicate fiducial markers that were placed ex-
vivo to correlate pathology and imaging. Red arrow and red
line indicate border of ablated area. (C) Vital staining using
CAM-5.2 immunostain shows devitalized tissue inside the
ablated area. Black arrows indicate fiducial markers that
were placed ex-vivo to correlate pathology and imaging. Red
arrow and line indicate the necrotic ablated tissue. Purple
arrow and line indicate the devitalized but structurally intact
ablated area.FOCAL LASER ABLATION OF PROSTATE CANCER 795
The ability to visualize the target, navigate an ablation tool to Focal ablation of the prostate using energy modalities other
that target, and monitor the ablation process all in real time is than laser under MR guidance with real-time monitoring is
crucial to perform truly focal therapy and minimize the being investigated but needs the development of new
morbidity. equipment and techniques,56–58 which adds further unneces-
PCa lesions were targeted based on multiparametric MR sary complexity and cost to a highly technical field.
scans. The MR imaging served to target the tumor once di- Another important or even crucial aspect of focal therapy is
agnosis was established with standard TRUS-BX. When the the ability to cause a confluent cellular ablation in the target
location is depicted by biopsy and the tumor is visualized by area. In an ongoing study, Trachtenberg and coworkers per-
MR scanning, it accurately denotes the specific location 83% of formed FLA followed by RP 1 week after the FLA procedure;
the time in the peripheral zone for tumors larger than 4 mm in using a two-fiber configuration and creating three different
diameter.54 The tumor coordinates and contours thus ob- ablation sites, they managed to create a uniform ablated zone
tained were then used to guide laser fiber placement by using that was verified by rigorous pathologic whole-mount sec-
3-dimensional ultrasonographic guidance. CEUS with real- tioning every 3 mm and using both hematoxylin and eosin
time monitoring of lesion size development increases the staining and vital staining (Fig. 2). The absence of any viable
likelihood of tumor destruction (Fig. 1). Using this technique, living cells in the ablated area lends to the scientific validity of
0.25 cm3 of PCa was targeted, creating a 2.2 cm3 well-defined FLA, which will again need to be confirmed with longer fol-
region of decreased enhancement or ablated zone. low-up.
The postprocedure and morbidity were negligible. Self-
limited perineal discomfort was the most common (25%) side Conclusion
effect and mild hematuria that did not warrant medical at- Focal therapy as a paradigm for treating patients with PCa
tention the most severe (16%). No significant drop in Inter- is still in evolution, but initial evidence suggests an advantage
national Index of Erectile Function-5 scores was noted up to 6 over whole-gland radical treatments in two elements of the
months postprocedure. There was no worsening of urinary trinity—potency and continence. Oncologic efficacy needs
symptoms as assessed by the International Prostate Symptom considerable follow-up for PCa patients and in a large number
Score and no incontinence using the strict criteria of no pads of patients for focal therapy to be accepted as a first-line op-
worn. tion in patients with low-risk PCa. So, there is much scientific
The short-term oncologic results seem promising, with no work ahead of us to further evaluate focal therapy, including
evidence of disease seen on results of postprocedure biopsy in evaluating what is the preferred imaging modality to be de-
50% of patients and 67% free of tumor at the ablated zone. So, ployed and what source of ablation energy to use.
RP attempts to achieve the ‘‘trinity’’ of cancer control, conti- FLA appears a promising energy modality, because lasers
nence, and maintenance of erectile function, but even in expert are readily available, relatively inexpensive, create confluent
hands, side effects remain significant. These data on FLA ablation zones, and can be easily monitored by both real-time
suggest that there were no cases of erectile function or conti- MR imaging and CEUS. We believe that all these attributes
nence compromise and that only longer-term data in larger will make FLA into a popular utility for focally ablating PCa.
series for follow-up of cancer control are needed before the
trinity is achieved for FLA. Disclosure Statement
Laser physics is a well-studied science. It is accurate, pre-
dictable, and reproducible and induces minimal damage No competing financial interests exist.
outside the targeted ablation zone. It has been demonstrated
References
to be a simple and effective means of prostate tissue de-
struction when used as a therapy for benign prostatic hy- 1. Jemal A, Siegel R, Ward E, et al. Cancer statistics, 2008. CA
perplasia55 and effective means of tumor ablation for a variety Cancer J Clin 2008;58:71–96.
of different tumors (Table 1). One of the main advantages in 2. Whitmore WF Jr. Localised prostatic cancer: Management
using FLA in general and for PCa treatment is that lasers are and detection issues. Lancet 1994;343:1263–1267.
highly MR compatible. MR imaging with its superb soft-tissue 3. Thompson IM, Pauler DK, Goodman PJ, et al. Prevalence of
contrast and its multiplanar capabilities has the best visuali- prostate cancer among men with a prostate-specific antigen
zation of the prostate and its surrounding anatomy. MR is level796 LINDNER ET AL.
Importance of methods and context. J Natl Cancer Inst 2009; 26. Ohori M, Eastham JA, Koh H, et al. Is focal therapy rea-
101:374–383. sonable in patients with early stage prostate cancer (CaP)—
9. Schröder FH. Screening for prostate cancer (PC)—an update an analysis of radical prostatectomy (RP) specimens. J Urol
on recent findings of the European Randomized Study of 2006;175(suppl):507–507.
Screening for Prostate Cancer (ERSPC). Urol Oncol 2008; 27. Onik G. Rationale for a "male lumpectomy," a prostate
26:533–541. cancer targeted approach using cryoablation: Results in 21
10. Draisma G, Boer R, Otto SJ, et al. Lead times and over- patients with at least 2 years of follow-up. Cardiovasc In-
detection due to prostate-specific antigen screening: Esti- tervent Radiol 2008;31:98–106.
mates from the European Randomized Study of Screening or 28. Ellis DS, Manny TB Jr, Rewcastle JC. Focal cryosurgery fol-
Prostate Cancer. J Natl Cancer Inst 2003;95:868–878. lowed by penile rehabilitation as primary treatment for lo-
11. Tsodikov A, Szabo A, Wegelin J. A population model of calized prostate cancer: Initial results. Urology 2007;70(suppl
prostate cancer incidence. Stat Med 2006;25:2846–2866. 6):9–15.
12. Bill-Axelson A, Holmberg L, Filén F, et al. Radical prosta- 29. Muto S, Yoshii T, Saito K, et al. Focal therapy with high-
tectomy versus watchful waiting in localized prostate can- intensity–focused ultrasound in the treatment of localized
cer: The Scandinavian prostate cancer group-4 randomized prostate cancer. Jpn J Clin Oncol 2008;38:192–199.
trial. J Natl Cancer Inst 2008;100:1144–1154. 30. Lindner U, Weersink RA, Haider MA, et al. Image guided
13. Schröder FH, Hugosson J, Roobol MJ, et al. Screening and photothermal focal therapy for localized prostate cancer:
prostate-cancer mortality in a randomized European study. Phase I trial. J Urol 2009;182:1371–1377.
N Engl J Med 2009;360:1320–1328. 31. Maiman TH. Stimulated optical radiation in ruby. Nature
14. Wei JT, Dunn RL, Sandler HM, et al. Comprehensive com- (Lond) 1960;187.
parison of health-related quality of life after contemporary 32. Knappe V, Frank F, Rohde E. Principles of lasers and bio-
therapies for localized prostate cancer. J Clin Oncol 2002; photonic effects. Photomed Laser Surg 2004;22:411–417.
20:557–566. 33. McGuff PE, Bushnell D, Soroff HS, Deterling RA Jr. Studies
15. Sanda MG, Dunn RL, Michalski J, et al. Quality of life and of the surgical applications of laser (light amplification by
satisfaction with outcome among prostate-cancer survivors. stimulated emission of radiation). Surg Forum 1963;14:143–
N Engl J Med 2008;358:1250–1261. 145.
16. Choo R, Klotz L, Danjoux C, et al. Feasibility study: 34. McGuff PE, Deterling RA Jr, Gottlieb LS, et al. Laser surgery
Watchful waiting for localized low to intermediate grade of malignant tumors. Dis Chest 1965;48:130–139.
prostate carcinoma with selective delayed intervention 35. McGuff PE, Deterling RA Jr, Gottlieb LS, et al. The laser
based on prostate specific antigen, histological and=or clin- treatment of experimental malignant tumours. Can Med
ical progression. J Urol 2002;167:1664–1669. Assoc J 1964;91:1089–1095.
17. Klotz L. Active surveillance with selective delayed inter- 36. Helsper JT, Sharp GS, Williams HF, Fister HW. The biolog-
vention for favorable risk prostate cancer. Urol Oncol ical effect of laser energy on human melanoma. Cancer
2006;24:46–50. 1964;17:1299–1304.
18. Bacon CG, Giovannucci E, Testa M, Kawachi I. The impact 37. Johnson FM, Olson R, Rounds DE. Effects of high-power
of cancer treatment on quality of life outcomes for patients green laser radiation on cells in tissue culture. Nature
with localized prostate cancer. J Urol 2001;166:1804–1810. 1965;205:721–722.
19. Galbraith ME, Ramirez JM, Pedro LW. Quality of life, health 38. Saks NM, Zuzolo RC, Kopac MJ. Microsurgery of living cells
outcomes, and identity for patients with prostate cancer in by ruby laser irradiation. Ann N Y Acad Sci 1965;122:695–712.
five different treatment groups. Oncol Nurs Forum 39. Tengroth B. The laser and its use in retinal surgery. Acta
2001;28:551–560. Ophthalmol (Copenh) 1966:suppl 84:135þ.
20. Litwin MS, Lubeck DP, Spitalny GM, et al. Mental health in 40. Tengroth B. Laser coagulation risks and advantages. Trans
men treated for early stage prostate carcinoma: A post- Ophthalmol Soc U K. 1966;86:55–61.
treatment, longitudinal quality of life analysis from the 41. Ingram HV. The laser ophthalmoscope coagulator. A pre-
Cancer of the Prostate Strategic Urologic Research Endeavor. liminary report. Trans Ophthalmol Soc U K 1964;84:453–467.
Cancer 2002;95:54–60. 42. Goldberg SN, Grassi CJ, Cardella JF, et al. Image-guided
21. Arredondo SA, Downs TM, Lubeck DP, et al. Watchful tumor ablation: Standardization of terminology and report-
waiting and health related quality of life for patients with ing criteria. Radiology 2005;235:728–739.
localized prostate cancer: Data from CaPSURE. J Urol 43. Bown SG. Phototherapy in tumors. World J Surg 1983;7:700–
2004;172:1830–1834. 709.
22. Steineck G, Helgesen F, Adolfsson J, et al. Quality of life after 44. Germer CT, Roggan A, Ritz JP, et al. Optical properties of
radical prostatectomy or watchful waiting. N Engl J Med native and coagulated human liver tissue and liver metas-
2002;347:790–796. tases in the near infrared range. Lasers Surg Med 1998;
23. Barocas DA, Cowan JE, Smith JA Jr, Carroll PR. What per- 23:194–203.
centage of patients with newly diagnosed carcinoma of the 45. Sapareto SA, Dewey WC. Thermal dose determination in
prostate are candidates for surveillance? An analysis of the cancer therapy. Int J Radiat Oncol Biol Phys 1984;10:787–800.
CaPSURE database. J Urol 2008;180:1330–1335. 46. Dewey WC. Arrhenius relationships from the molecule and
24. van den Bergh RC, Roemeling S, Roobol MJ, et al. Outcomes cell to the clinic. Int J Hyperthermia 2009;25:3–20.
of men with screen-detected prostate cancer eligible for ac- 47. McNichols RJ, Gowda A, Kangasniemi M, et al. MR ther-
tive surveillance who were managed expectantly. Eur Urol mometry-based feedback control of laser interstitial thermal
2008. Epub ahead of print. therapy at 980 nm. Lasers Surg Med. 2004;34:48–55.
25. Onik G, Narayan P, Vaughan D, et al. Focal "nerve-sparing" 48. Vogl TJ, Straub R, Zangos S, et al. MR-guided laser-induced
cryosurgery for treatment of primary prostate cancer: A new thermotherapy (LITT) of liver tumours: Experimental and
approach to preserving potency. Urology 2002;60:109–114. clinical data. Int J Hyperthermia 2004;20:713–724.FOCAL LASER ABLATION OF PROSTATE CANCER 797
49. Atri M, Gertner MR, Haider MA, et al. Contrast-enhanced 63. Papini E, Guglielmi R, Bizzarri G, et al. Treatment of benign
ultrasonography for real-time monitoring of interstitial laser cold thyroid nodules: A randomized clinical trial of per-
thermal therapy in the focal treatment of prostate cancer. cutaneous laser ablation versus levothyroxine therapy or
Can Urol Assoc J 2009;3:125–130. follow-up. Thyroid 2007;17:229–235.
50. Vogl TJ, Straub R, Eichler K, et al. Colorectal carcinoma 64. Amabile G, Rotondi M, De Chiara G, et al. Low-energy in-
metastases in liver: Laser-induced interstitial thermo- terstitial laser photocoagulation for treatment of nonfunc-
therapy—local tumor control rate and survival data. Radi- tioning thyroid nodules: Therapeutic outcome in relation to
ology 2004;230:450–458. pretreatment and treatment parameters. Thyroid 2006;16:
51. Gough-Palmer AL, Gedroyc WM. Laser ablation of hepato- 749–755.
cellular carcinoma—a review. World J Gastroenterol 65. Mack MG, Straub R, Eichler K, et al. MR-guided laser-
2008;14:7170–7174. induced thermotherapy in recurrent extrahepatic abdominal
52. Pacella CM, Francica G, Di Lascio FM, et al. Long-term tumors. Eur Radiol 2001;11:2041–2046.
outcome of cirrhotic patients with early hepatocellular car- 66. Rosenberg C, Puls R, Hegenscheid K, et al. Laser ablation of
cinoma treated with ultrasound-guided percutaneous laser metastatic lesions of the lung: Long-term outcome. AJR Am J
ablation: A retrospective analysis. J Clin Oncol 2009;27:2615– Roentgenol 2009;192:785–792.
2621. 67. Gangi A, Alizadeh H, Wong L, et al. Osteoid osteoma:
53. Ferrari FS, Stella A, Pasquinucci P, et al. Treatment of small Percutaneous laser ablation and follow-up in 114 patients.
hepatocellular carcinoma: A comparison of techniques and Radiology 2007;242:293–301.
long-term results. Eur J Gastroenterol Hepatol 2006;18:659– 68. Streitparth F, Gebauer B, Melcher I, et al. MR-guided laser
672. ablation of osteoid osteoma in an open high-field system (1.0
54. Haider MA, van der Kwast TH, Tanguay J, et al. Combined T). Cardiovasc Intervent Radiol 2009;32:320–325.
T2-weighted and diffusion-weighted MRI for localization of 69. Dick EA, Joarder R, De Jode MG, et al. Magnetic resonance
prostate cancer. AJR Am J Roentgenol 2007;189:323–328. imaging-guided laser thermal ablation of renal tumours. BJU
55. Kuntz RM. Current role of lasers in the treatment of benign Int 2002;90:814–822.
prostatic hyperplasia (BPH). Eur Urol 2006;49:961–969. 70. van Esser S, Stapper G, van Diest PJ, et al. Ultrasound-
56. de Senneville BD, Mougenot C, Moonen CT. Real-time guided laser-induced thermal therapy for small palpable
adaptive methods for treatment of mobile organs by MRI- invasive breast carcinomas: A feasibility study. Ann Surg
controlled high-intensity focused ultrasound. Magn Reson Oncol 2009;16:2259–2263.
Med 2007;57:319–330.
57. de Senneville BD, Mougenot C, Quesson B, et al. MR ther- Address correspondence to:
mometry for monitoring tumor ablation. Eur Radiol Uri Lindner, M.D.
2007;17:2401–2410. 610 University Ave.,
58. Mougenot C, Quesson B, de Senneville BD, et al. Three- Toronto, ON, M5G 2M9
dimensional spatial and temporal temperature control with Canada
MR thermometry-guided focused ultrasound (MRgHIFU).
Magn Reson Med 2009;61:603–614. E-mail: lindneruri@gmail.com
59. Puls R, Langner S, Rosenberg C, et al. Laser ablation of liver
metastases from colorectal cancer with MR thermometry: 5- Abbreviations Used
year survival. J Vasc Interv Radiol 2009;20:225–234. AS ¼ active surveillance
60. Schwarzmaier HJ, Eickmeyer F, von Tempelhoff W, et al. CEUS ¼ contrast-enhanced ultrasonography
MR-guided laser-induced interstitial thermotherapy of re- FLA ¼ focal laser ablation
current glioblastoma multiforme: Preliminary results in 16 HCC ¼ hepatocellular carcinoma
patients. Eur J Radiol 2006;59:208–215. HIFU ¼ high-intensity focused ultrasound
61. Leonardi MA, Lumenta CB, Gumprecht HK, et al. Stereo- MR ¼ magnetic resonance
tactic guided laser-induced interstitial thermotherapy Nd:YAG ¼ neodymium:yttrium-aluminum-garnet
(SLITT) in gliomas with intraoperative morphologic moni- PCa ¼ prostate cancer
toring in an open MR-unit. Minim Invasive Neurosurg PSA ¼ prostate-specific antigen
2001;44:37–42. QoL ¼ quality of life
62. Carpentier A, McNichols RJ, Stafford RJ, et al. Real-time mag- RP ¼ radical prostatectomy
netic resonance-guided laser thermal therapy for focal meta- TRUS-BX ¼ transrectal ultrasonographic biopsy
static brain tumors. Neurosurgery 2008;63(suppl 1):ONS21-29.This article has been cited by: 1. Brent Weinberg, Jinming GaoPolymer Implants for Intratumoral Drug Delivery and Cancer Therapy 221-244. [CrossRef] 2. Joyce G. R. Bomers, J. P. Michiel Sedelaar, Jelle O. Barentsz, Jurgen J. Fütterer. 2012. MRI-Guided Interventions for the Treatment of Prostate Cancer. American Journal of Roentgenology 199:4, 714-720. [CrossRef] 3. Yipeng Hu, Hashim Uddin Ahmed, Zeike Taylor, Clare Allen, Mark Emberton, David Hawkes, Dean Barratt. 2012. MR to ultrasound registration for image-guided prostate interventions. Medical Image Analysis 16:3, 687-703. [CrossRef] 4. Pierre Colin, Serge Mordon, Pierre Nevoux, Mohammed Feras Marqa, Adil Ouzzane, Philippe Puech, Gregory Bozzini, Bertrand Leroux, Arnauld Villers, Nacim Betrouni. 2012. Focal Laser Ablation of Prostate Cancer: Definition, Needs, and Future. Advances in Urology 2012, 1-10. [CrossRef] 5. Mohamad-Feras Marqa, Pierre Colin, Pierre Nevoux, Serge R Mordon, Nacim Betrouni. 2011. Focal Laser Ablation of Prostate Cancer: Numerical Simulation of Temperature and Damage Distribution. BioMedical Engineering OnLine 10:1, 45. [CrossRef]
You can also read

















































