MEDULLOBLASTOMA (PNET-Mb): Atypical clinical presentation
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
1
MEDULLOBLASTOMA (PNET-Mb):
Atypical clinical presentation
González Inés, Arburúas Macarena, Sgarbi Nicolás
Departament of Clinical Radiology
Hospital de Clínicas
ABSTRACT
Medulloblastoma is the most frequent primary brain tumor in children. It is located
in the posterior fossa and has a very unfavorable prognosis.
It is an aggressive tumor that seeds via CSF. It has both high dissemination rate
and high recurrence rate.
An early diagnosis is necessary in order to carry out an effective treatment that
can improve survival, although the survival rate itself is relatively poor
Magnetic resonance is the method of choice for diagnosis and follow-up, with an
excellent overall performance even if atypical clinical presentations do exist.
It is basic to remember a group of less frequent clinical features in these tumors:
location at the cerebellar hemispheres, superficial or even extra-axial topography,
signal of heterogeneous intensity in T1- and T2-weighted sequences, lack of
diffusion restriction and poor contrast enhancement or no enhancement.
Knowing these atypical clinical presentations is essential for early diagnosis, with
all it implies for the patient regarding treatment and prognosis.
The objective of this study is to review a group of 5 patients with a confirmed final
diagnosis of medulloblastoma whose MRI appearance on imaging studies
performed at our center was atypical.
KEY WORDS: brain tumors, medulloblastoma, PNET-MB, magnetic resonance.
INTRODUCTION the incidence rates peak between the
second and the fourth decades [2].
Histological and molecular variety for
Medulloblastoma (PNET-Mb) is the this tumor is of such magnitude that
most common malignant tumor of the even if all PNET-Mb types belong to
central nervous system (CNS) in grade IV of the WHO classification,
childhood, the second most frequent risk and prognosis vary considerably
of all cancers in this age group and according to type.
also the most common posterior It is an aggressive tumor that shows
fossa tumor in children [1-7]. a high dissemination rate to the
It appears most frequently in males cerebrospinal fluid (CSF) (33% at the
below 10 years of age, while in adults
§ ICONOGRAPHIC ESSAY /Dres. Gonzalez I., Arburuas M., Sgarbi N. 272
moment of diagnosis) and a high Spectroscopy (MRS) and perfusion
recurrence rate [6]. (PWI) are other useful MR
The most frequent location is the sequences whose contributions are
cerebellum, the vermis in particular currently being reviewed. Neither
[2, 4]; the tumor tends to spread to technique offers specific data for
the cerebellar hemispheres in diagnosis, but both are used as
adolescents and adults [6, 7]. complements to the conventional
Atypical forms usually occur in those sequences, mainly to confirm
two age groups. diagnosis in doubtful cases.
In general, clinical illness is of short It is essential to grade tumors with
duration (less than 3 months), which precision; therefore it is mandatory to
reflects the aggressive behavior of perform MR of the whole neural axis
this tumor. to assess spread to the CSF and
The most common symptoms are subsequent leptomeningeal seeding
headache, nausea and vomiting [6]. [6].
In classic magnetic resonance (MR) Nowadays different PNET-Mb
the image is that of a subgroups are described, each with
heterogeneously contrast-enhanced different histological and genomic
lesion of the cerebellar vermis, with characteristics which are mainly
well-defined margins, of iso- or reflected in their prognoses [8, 9].
hypointense signal in the T1- These various subgroups also show
weighted images and of differential imaging characteristics,
hyperintense signal in the T2- as we will see in the cases presented
weighted images, surrounded by below.
vasogenic edema [2,6]. Surgical resection, radiotherapy and
More than 40% of PNET-Mbs deviate chemotherapy have decreased the
in some way from this classic pattern, mortality associated to this tumor,
mainly when they occur in adult with a 5-year survival rate of 50%-
patients. 80% [6, 7].
These tumors spread to the Prognosis is better for female
cerebellar hemispheres and their patients aged 10 to 19, whose
aspect in T1- and T2-weighted hemispheric lesions were completely
images changes: cystic zones resected.
appear as a result of degeneration or Both dissemination at the moment of
necrosis, there is no diffusion diagnosis and recurrence remain the
restriction, enhancement is poor, chief limiting factors for the cure [2,
hemorrhagic areas are noted, and 6].
margins become indistinct. The objective of this study is to
Diffusion-weighted sequences (DWI review and highlight MR signs in a
sequences) nearly constantly show group of atypical PNET-Mb patients.
intense restriction. Several authors
have considered this sign as very
characteristic and linked it to high
tumoral cellularity.
The more cellular a tumoral tissue
becomes, the more aggressive it is,
that is why the apparent diffusion
coefficient (ADC) can be used to
determine tumor grading [2, 4].
28 Rev. Imagenol. 2da Ep. Jul/Dic 2016 XX (1).3
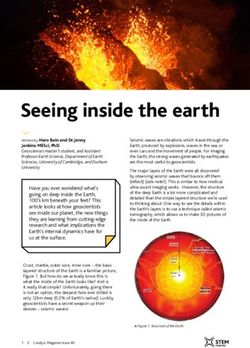
DESCRIPTION OF CASES Edema is also present. Figure 1
In the DWI/ADC scans the lesion
CASE 1 (Figures 1 and 2) evidences restriction. After
22-year-old male. administering a contrast agent
Present illness: Pulsating headaches moderate heterogeneous uptake is
for the last 2 months, drunken gait on observed. Figure 2. The remaining
examination. neuraxis and the rest of the body
The MR scan shows a lesion of the were scanned in order to complete
left cerebellar hemisphere that grading, but no other lesions were
causes mass effect locally. It is a found.
solid lesion, with hypointense signal The surgeon decided to resect this
in T1-weighted images and process. A complete removal was
hyperintense signal in T2-weighted performed and no complications
images; it includes inner cystic zones ensued.
(*) and a central calcification (è).
Figure 1: Sagittal T1 SE sequences, FSE T2-weighted images, FLAIR
images, GRE T2-weighted images, diffusion-weighted images and axial
ADC map (see text for description).
§ ICONOGRAPHIC ESSAY /Dres. Gonzalez I., Arburuas M., Sgarbi N. 294
Figure 2: Axial and coronal SE T1-weighted sequences with
fat saturation and gadolinium in both axial and coronal
planes (see text for description).
The diagnosis was confirmed: it was the last 2 weeks, Horizontal
a desmoplastic PNET-Mb of the SHH nystagmus on examination.
subgroup. The patient did well, was MR scan was performed and showed
discharged and is being followed up a vermis lesion compressing the
by the oncologist. fourth ventricle as well as
Tumors of this group accounts for a supratentorial hydrocephalus.
little less than 30% of the total It was a solid-cystic lesion. The solid
number of these tumors. They occur zones (*) appear as isointense
in children and young adults, with no signals in T1-weighted sequences
gender predominance. and predominantly as hyperintense
signals in T2-weighted sequences
and FLAIR scans, with intense
CASE 2 (Figure 3) heterogeneous enhancement.
12-year-old female. No restriction was present in the
Present illness: Moderate DWI/ADC scans.
headaches, mostly occipital, during The peripheral cystic component
shows a homogeneous content (è)
and non-enhanced walls.
30 Rev. Imagenol. 2da Ep. Jul/Dic 2016 XX (1).5
Figure 3: Sagittal SE T1-weighted sequences, FSE T2-weighted images,
FLAIR images, diffusion-weighted images, axial ADC map and post-
gadolinium Fat-Sat SE T1-weighted images (see text for description).
Surgery was performed: partial CASE 3 (Figures 4 and 5)
tumoral resection and 3-year-old male patient.
ventriculoperitoneal shunt, Present illness. Irrepressible
The Pathology report confirmed the vomiting during the last 4 days. Gait
diagnosis of anaplasic PNET-Mb disorder on examination.
belonging to the Non-WNT/Non-SHH The MR scan shows a cerebellar
Group 3. Two weeks after the lesion located in the left hemisphere
operation follow-up MR was done that compresses and displaces the
and showed that the tumoral process fourth ventricle. It is mostly solid with
persisted with evidence of seeding in hypointense signal in T1-weighted
the subarachnoid space, but with no sequences and hyperintense signal
hydrocephalus. in T2-weighted sequences and
These tumors represent around 30% FLAIR scans.
of the total number of The central zone shows
medulloblastomas, the rate of hyperintense signal in the T2-
incidence being higher in male weighted sequences. In the FLAIR
children. This group has the worst scan the signal is suppressed
prognosis: 5-year survival rate of indicating a small cystic area.
50%.
§ ICONOGRAPHIC ESSAY /Dres. Gonzalez I., Arburuas M., Sgarbi N. 316
Figure 4:
Sagittal SE T1-
weighted
sequences;
axial SE T1-
weighted
sequences,
FSE T2-
weighted
sequences and
FLAIR images
(see text for
description).
Figure 5:
Diffusion-
weighted
images; axial
ADC map; axial
and coronal fat-
saturated post-
gadolinium SE
T1-weighted
images (see
text for
description).
32 Rev. Imagenol. 2da Ep. Jul/Dic 2016 XX (1).7
In the DWI/ADC sequences Tumors in this group represent about
restriction is intense and there is no 10% of the total number of
enhancement with the contrast medulloblastomas. They occur in
agent. children or adults, with a slight
The patient underwent emergency predominance of females.
surgery, which confirmed the It is the group with the best
histopathological diagnosis of classic prognosis: 5-year survival rate of
PNET-Mb of the WNT subgroup. 95%.
Figure 6: Axial SE T1-weighted, FLAIR and FSE T2-weighted images;
coronal FSE T2-weighted images; axial post-gadolinium SE T1-weighted
images and axial diffusion-weighted images (see text for description).
§ ICONOGRAPHIC ESSAY /Dres. Gonzalez I., Arburuas M., Sgarbi N. 338
CASE 4 (Figure 6) It had no restriction in DWI/ADC
20-year-old female patient. scans and was not enhanced by the
Progressively intense headaches contrast agent.
during the last month, with vomiting. The patient underwent partial
No focal neurological signs, no fever. resection. The diagnosis was
A cerebellar lesion, of paramedian confirmed: it was a classic PNET-Mb,
vermian location, was observed in a Non-WNT/Non-SHH lesion
the MR head scan. It appeared to be belonging to group 4.
infiltrative, with a moderate local Such lesions constitute the most
mass effect. This lesion was important molecular subgroup,
hypointense in the T1-weighted amounting to nearly 35%. They occur
sequences and hyperintense in both most frequently in males and are rare
T2-weighted sequences and FLAIR in adults.
scans. Lack of enhancement is
characteristic. Prognosis is similar to
that of group 3.
Figure 7. Axial sequences: FSE T2-weighted, SE T1-weighted, FLAIR and
diffusion-weighted. Axial ADC map. Post-gadolinium SE T1-weighted
sequences. (see text for description).
34 Rev. Imagenol. 2da Ep. Jul/Dic 2016 XX (1).9
CASE 5 (Figure 7) lack of diffusion restriction, poor
23-year-old female. No previous enhancement and hemorrhagic
medical history. Had intense areas.
headaches and vertigo shortly before Topography is one of the atypical
admission. No focal neurological characteristics and in general relates
signs on examination. An to age. The older the patient, the
infratentorial lesion at the left greater the tendency to spread
cerebellopontine angle stands out in laterally to the cerebellar
the MR scans. This mostly solid hemispheres [6, 7].
lesion is hypointense in T1-weighted Out of five cases, three were located
sequences, hyperintense in the T2- in the hemispheres; another
weighted ones and shows restriction occupied the vermis as well as the
zones in the DWI/ADC scans. It has left cerebellar hemisphere and only
a cystic center. Poor heterogeneous one presented with the typical
enhancement is present. vermian location.
The patient underwent surgery and The most frequent atypical
the immediate outcome was good. phenomenon to be observed was
Diagnosis was confirmed, it was a cystic degeneration, which appeared
classic PNET-Mb, of the WNT in four cases.
subgroup. Restriction is a frequent
As we have already seen, this type manifestation in Mb, in spite of which
occurs more frequently in females two of our cases lack restriction in the
and young adults. DWI/ADC scans.
Mb characteristically shows
DISCUSSION enhancement after injection of the
contrast agent. In two of these five
We have presented a series of 5 cases gadolinium administration was
cases of medulloblastoma with followed by poor enhancement or did
atypical findings in the MR scans. not cause enhancement, all of which
Pathology results confirmed the is rated as an atypical characteristic
diagnosis in all cases. in scientific literature.
Case histories match with In one case calcifications were
descriptions in published reports: identified within the tumor, another
same symptoms (headache, element in the spectrum of atypical
vomiting), all of them progressing Mb characteristics.
rapidly which reflects the great No case presented with hemorrhage.
aggressiveness of the tumor. These atypical presentations
Two of the patients were notwithstanding, in the series under
adolescents, an atypical age for review MR permitted a diagnosis of
onset [2]. Mb, which confirms the overall good
The classic MR image of Mb was performance of this method, no
observed in 60% of the scans. matter what signs are present.
Atypical manifestations were
observed mainly in adults: lateral
spread to the cerebellar
hemispheres, different behavior of
T1 and T2, cystic zones caused by
degeneration or necrosis,
calcifications, ill-defined borders,
§ ICONOGRAPHIC ESSAY /Dres. Gonzalez I., Arburuas M., Sgarbi N. 3510
CONCLUSIONS
6. Koeller K., Rushing E. From the
archives of the AFIP:
In the series we have presented the Medulloblastoma: a
most frequently observed atypical comprehensive review with
elements were different locations, radiologic-pathologic correlation.
with lesions appearing in the Radiographics. 2003; 23:1613-
cerebellar hemispheres. 37.
Other atypical findings in this series:
lack of restriction in DWI/ADC scans, 7. García Casales Z, Echebarría
presence of cysts and calcifications Barona A, Urberuaga Pascual A
in the centre of the tumor, no et al. Meduloblastoma: aspectos
enhancement after injection of diferenciales entre el tumor
contrast agent. infantil y del adulto. Medicina
Diagnosis was made possible by Clínica 2009; 133(12):454-459.
previous knowledge of the possibility
of these atypical characteristics, 8. Taylor MD, Northcott PA, et al.
correct analysis of tumoral Molecular subgroups of
semiology, clinical context and sense medulloblastoma: the current
of frequency. consensus. Acta
Neuropathologica 2012; 123 (4):
465-472.
REFERENCES
9. Ellison DW, Giangaspero F,
Eberhart CG et al.
1. Fisher J, Schwartzbaum J, Meduloblastomas, genetically
Wrensch M et al. Epidemiology defined. Cap 8: Embryonal
of brain tumors. Neurol Clin 2007; tumours, pag: 188-193. En: WHO
25(4):867-90. Classification of Tumours of the
central nervous system. 4th
2. Martínez León M. Review and edition, Lyon 2016.
update about medulloblastoma in
children. Radiologia. 2011;
53:134-45.
3. Dahll G. Medulloblastoma. J
Child Neurol. 2009; 24:1418-30.
4. Adamski J, Ramaswamy V,
Huang A, et al. Advances in
managing medulloblastoma and
intracranial primitive neuro-
ectodermal tumors. F1000Prime
Reports 2014; 6:56-68.
5. Dipu B, Mrinal B, Pradipta
RC. The clinical profile and
radiological variations of
medulloblastoma. IJHS 2014; 4-
31(11):22
36 Rev. Imagenol. 2da Ep. Jul/Dic 2016 XX (1).You can also read