Metabolic Spectrum of Liver Failure in Type 2 Diabetes and Obesity: From NAFLD to NASH to HCC - MDPI
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
International Journal of
Molecular Sciences
Review
Metabolic Spectrum of Liver Failure in Type 2 Diabetes and
Obesity: From NAFLD to NASH to HCC
Hyunmi Kim 1,2,† , Da Som Lee 1,† , Tae Hyeon An 1,2,† , Hyun-Ju Park 1,2 , Won Kon Kim 1,2 ,
Kwang-Hee Bae 1,2, * and Kyoung-Jin Oh 1,2, *
1 Metabolic Regulation Research Center, Korea Research Institute of Bioscience and Biotechnology (KRIBB), 125
Gwahak-ro, Yuseong-gu, Daejeon 34141, Korea; khm7607@kribb.re.kr (H.K.); dasom89@kribb.re.kr (D.S.L.);
anth0291@kribb.re.kr (T.H.A.); h18509@kribb.re.kr (H.-J.P.); wkkim@kribb.re.kr (W.K.K.)
2 Department of Functional Genomics, KRIBB School of Bioscience, Korea University of Science and
Technology (UST), 217 Gajeong-ro, Yuseong-gu, Daejeon 34141, Korea
* Correspondence: khbae@kribb.re.kr (K.-H.B.); kjoh80@kribb.re.kr (K.-J.O.); Tel.: +82-42-860-4268 (K.-H.B.);
+82-42-879-8265 (K.-J.O.)
† These authors contributed equally to this work.
Abstract: Liver disease is the spectrum of liver damage ranging from simple steatosis called as
nonalcoholic fatty liver disease (NAFLD) to hepatocellular carcinoma (HCC). Clinically, NAFLD
and type 2 diabetes coexist. Type 2 diabetes contributes to biological processes driving the severity
of NAFLD, the primary cause for development of chronic liver diseases. In the last 20 years, the
rate of non-viral NAFLD/NASH-derived HCC has been increasing rapidly. As there are currently
no suitable drugs for treatment of NAFLD and NASH, a class of thiazolidinediones (TZDs) drugs
for the treatment of type 2 diabetes is sometimes used to improve liver failure despite the risk of
side effects. Therefore, diagnosis, prevention, and treatment of the development and progression
Citation: Kim, H.; Lee, D.S.; An, T.H.;
of NAFLD and NASH are important issues. In this review, we will discuss the pathogenesis of
Park, H.-J.; Kim, W.K.; Bae, K.-H.; Oh,
NAFLD/NASH and NAFLD/NASH-derived HCC and the current promising pharmacological
K.-J. Metabolic Spectrum of Liver
therapies of NAFLD/NASH. Further, we will provide insights into “adipose-derived adipokines”
Failure in Type 2 Diabetes and
Obesity: From NAFLD to NASH to
and “liver-derived hepatokines” as diagnostic and therapeutic targets from NAFLD to HCC.
HCC. Int. J. Mol. Sci. 2021, 22, 4495.
https://doi.org/10.3390/ijms22094495 Keywords: non-alcholic fatty liver disease (NAFLD); non-alcoholic steatohepatitis (NASH); hepato-
cellular carcinoma (HCC); type 2 diabetes; obesity; adipokines; hepatokines
Academic Editors: Montserrat Esteve
and Maria del Mar Romeno
Received: 2 April 2021 1. Introduction
Accepted: 23 April 2021
Type 2 diabetes is the main public health problem in terms of global epidemic and
Published: 26 April 2021
pandemic diseases [1,2]. It is closely related with the worldwide epidemic of obesity, and
approximately 75% of type 2 diabetes is related with obesity [3,4]. The relationship between
Publisher’s Note: MDPI stays neutral
type 2 diabetes and obesity is further explained by the descriptive term of “Diabesity” [5].
with regard to jurisdictional claims in
Actually, the modern sedentary lifestyle contributes to weight gain by promoting excessive
published maps and institutional affil-
food intake and even adding physical inactivity [6,7]. For that reason, chronic metabolic
iations.
diseases such as type 2 diabetes and obesity have been increasing globally.
Together with obesity and type 2 diabetes, non-alcoholic fatty liver (NAFLD) is
the most common liver disease, and is observed in approximately 30% of the general
population [8–10]. NAFLD is characterized by hepatic triglyceride (TG) accumulation
Copyright: © 2021 by the authors.
and insulin resistance [11,12]. It is the hepatic manifestation of metabolic syndrome
Licensee MDPI, Basel, Switzerland.
and is a spectrum of conditions ranging from benign hepatic steatosis to non-alcoholic
This article is an open access article
steatohepatitis (NASH) [13]. That is, it is broadly categorized into non-alcoholic fatty liver
distributed under the terms and
(NAFL) and NASH [14]. NAFL is marked by isolated steatosis, and NASH is characterized
conditions of the Creative Commons
by steatosis, lobular inflammation (inflammatory cell infiltration), and hepatocellular
Attribution (CC BY) license (https://
ballooning in the presence or absence of fibrosis [15]. NASH, the more aggressive form
creativecommons.org/licenses/by/
4.0/).
of NAFLD, could develop into progressive fibrosis, and is directly associated with the
Int. J. Mol. Sci. 2021, 22, 4495. https://doi.org/10.3390/ijms22094495 https://www.mdpi.com/journal/ijms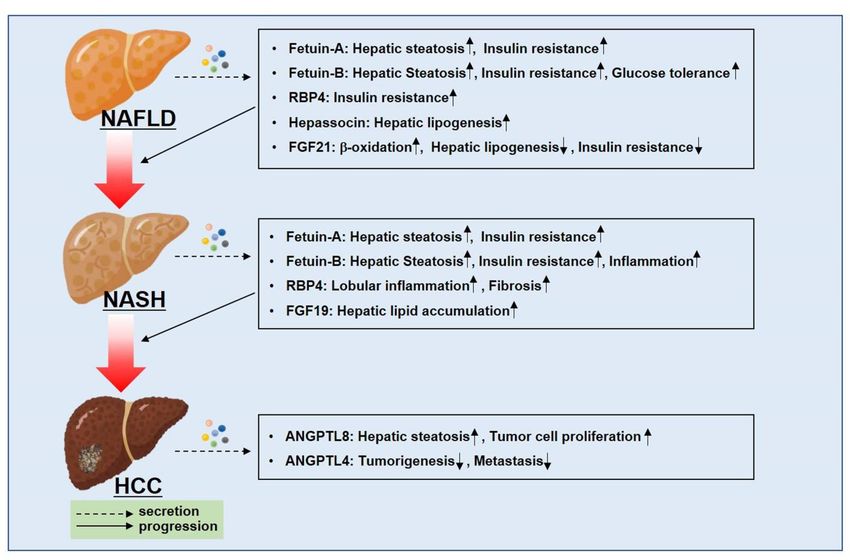
oping hepatocellular carcinoma (HCC), which could be a major cause of morbidity
mortality induced from liver failure (Figure 1) [8]. The prevalence of NASH is app
mately ~30% for patients with NAFLD [16–19]. Approximately 20% of NASH pat
with fibrosis progress to cirrhosis [20]. Liver cirrhosis is present in only 50% of pat
with NAFLD-related HCC [21,22]. The incidence of NAFLD-related HCC without ci
Int. J. Mol. Sci. 2021, 22, 4495 2 of 30
sis is approximately 8% of all HCC cases [23,24]. The incidence rate for HC
NAFLD/NASH with cirrhosis ranges from 2% to 13% (Figure 1) [25,26].
risk of developing Clinically,
hepatocellularNAFLD coexists (HCC),
carcinoma with type 2 diabetes
which couldandbe obesity,
a majorand it exerts
cause of a syne
tic effect, leading to more severe liver failures [27]. The prevalence
morbidity and mortality induced from liver failure (Figure 1) [8]. The prevalence of NASH rate of NAFLD is
is approximatelymated
~30%toforbe patients
approximately 75% in [16–19].
with NAFLD patientsApproximately
with type 2 diabetes
20% ofand
NASHabout 90% i
patients with fibrosis progress to cirrhosis [20]. Liver cirrhosis is present in only 50% of2 diabete
obese population, which show the strong relationship of NAFLD with type
obesity [28–31].HCC
patients with NAFLD-related NAFLD plays
[21,22]. Thean important
incidence role in increasesHCC
of NAFLD-related of the incidence of ty
without
cirrhosis is approximately 8% of all HCC cases [23,24]. The incidence rate for HCC in to mo
diabetes and its complications [28]. Type 2 diabetes also exacerbates NAFLD
NAFLD/NASHvere withforms of NASH,
cirrhosis rangesfibrosis,
from 2% andtoHCC (Figure 1)
13% (Figure 1) [25,26].
[30,32,33].
Figure
Figure 1. Type 2 1. Type 2 and
diabetes diabetes andaggravate
obesity obesity aggravate the progression
the progression of NAFLD/NASH
of NAFLD/NASH to HCC.toClinically,
HCC. Clinically,
type 2 diabetes
coexists with
typeNAFLD, and coexists
2 diabetes it aggravates
with NAFLD
NAFLD,toandmore severe forms
it aggravates of NASH,
NAFLD hepatocirrhosis,
to more severe formsand
ofHCC,
NASH,leading to a
metabolically worse phenotype.
hepatocirrhosis, and HCC, leading to a metabolically worse phenotype.
Clinically, NAFLD HCC is one with
coexists of thetype
most aggressive
2 diabetes andgrowing
obesity, cancers [34,35].
and it exerts Previously, hepat
a synergistic
effect, leading tovirus
more(HCV)
severewasliverthought
failuresto[27].
be the
Theleading cause
prevalence of of
rate HCCNAFLD[36–38], but recent reports
is estimated
showed
to be approximately 75%up to
in50% of newly
patients withdiagnosed HCC patients
type 2 diabetes are non-viral
and about 90% in the HCC [39,40], There
obese
population, which NAFLD/NASH-derived HCC has been
show the strong relationship highlighted.
of NAFLD withThetypeetiology
2 diabetesof NAFLD/NASH
and
obesity [28–31].rived
NAFLDHCCplays is very
ancomplex
important androle
is related with various
in increases of the mechanisms
incidence of such type as
2 cellular
diabetes and itsticity, inflammation,
complications apoptosis,
[28]. Type cell cycle,
2 diabetes and cell death
also exacerbates NAFLD [41,42]. It is not
to more easy to trea
severe
forms of NASH, improve
fibrosis,HCC.
and HCCTherefore,
(FigureNAFLD/NASH
1) [30,32,33]. treatment is required for prevention of
HCC is one versible chronic
of the most liver diseases
aggressive growingsuchcancers
as cirrhosis and
[34,35]. HCC. Unfortunately,
Previously, hepatitis C there a
virus (HCV) was FDA-approved
thought to bedrugs and treatment
the leading cause ofmethods yet. but recent reports that
HCC [36–38],
showed up to 50% ofInnewly this review,
diagnosed we HCC
will discuss
patients the pathogenesis
are non-viral HCCof[39,40],
NAFLD/NASH
Therefore,and NA
NAFLD/NASH-derivedNASH-derived HCCHCC and the
has been current promising
highlighted. pharmacological
The etiology of NAFLD/NASH- therapies of NA
derived HCC isNASH. Further, the
very complex andinitiation
is relatedand withprogression of NAFLD can
various mechanisms suchbe as
affected by organo
cellular
secreted from
plasticity, inflammation, metabolic
apoptosis, cell organs
cycle, andundercellmetabolic disturbance
death [41,42]. It is notsuch
easyastotype
treat2 diabete
and improve HCC. obesity [43–45]. Therefore,
Therefore, NAFLD/NASH we willtreatment
focus on organokines
is required that are secretedofby the ad
for prevention
tissues
irreversible chronic anddiseases
liver liver, which
such are critical organs
as cirrhosis for the
and HCC. regulation of lipid
Unfortunately, theremetabolism.
are no We
FDA-approvedprovidedrugs and newtreatment
insights into “adipokines”
methods yet. and “hepatokines” that can be potential diag
tic and
In this review, wetherapeutic
will discuss targets in NAFLD/NASH
the pathogenesis and NAFLD/NASH-derived
of NAFLD/NASH and NAFLD/ HCC. The
NASH-derivedthought HCC and to be
theable to be biological
current promisingmarkers that can predict
pharmacological NAFLD
therapies severity from NA
of NAFLD/
NASH. Further,tothe HCC.
initiation and progression of NAFLD can be affected by organokines
secreted from metabolic organs under metabolic disturbance such as type 2 diabetes and
obesity [43–45]. Therefore, we will focus on organokines that are secreted by the adipose
tissues and liver, which are critical organs for the regulation of lipid metabolism. We will
provide new insights into “adipokines” and “hepatokines” that can be potential diagnostic
and therapeutic targets in NAFLD/NASH and NAFLD/NASH-derived HCC. They are
thought to be able to be biological markers that can predict NAFLD severity from NAFLD
to HCC.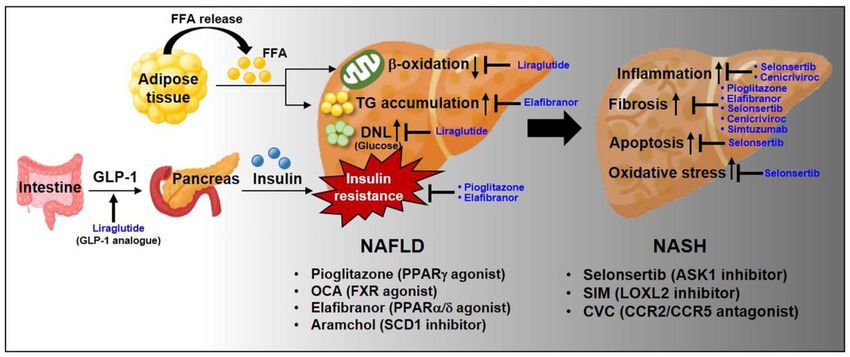
Int. J. Mol. Sci. 2021, 22, x FOR PEER REVIEW
Int. J. Mol. Sci. 2021, 22, 4495 3 of 30
2. Non-Alcoholic Fatty Liver Disease (NAFLD) and Non-Alcoholic Steatohepatit
2. Non-Alcoholic (NASH)
Fatty Liver Disease (NAFLD) and Non-Alcoholic
Steatohepatitis2.1.
(NASH)
Pathogenesis of NAFLD and NASH
2.1. Pathogenesis2.1.1.
of NAFLD and NASH
An Imbalance in Fatty Acid (FA) Metabolism
2.1.1. An Imbalance in Fatty Acid (FA) Metabolism
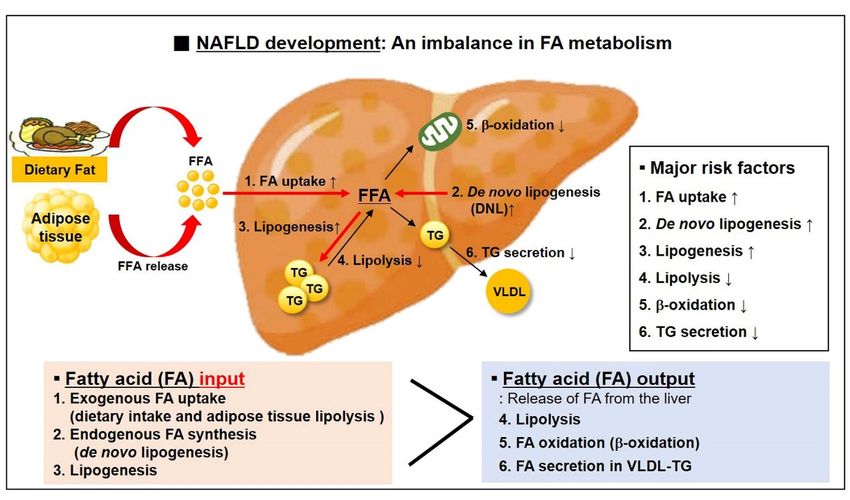
NAFLD is the most common etiology of chronic liver diseases. NAFLD results
NAFLD is excessive
the most common etiology
triglyceride of chronic liverindiseases.
(TG) accumulation the liverNAFLD
[11,12]. results fromthe balan
Therefore,
excessive triglyceride (TG) accumulation in the liver [11,12]. Therefore, the balance between
tween fatty acid (FA) input and FA output is critical [46,47]. That is, NAFLD dev
fatty acid (FA) when
input the
andamount
FA output is critical [46,47].
of “exogenous That
FA uptake is, NAFLD
(dietary intakedevelops
and adiposewhentissue lipo
the amount of “exogenous FA uptake (dietary intake and adipose tissue
and “endogenous FA synthesis (DNL: de novo lipogenesis)” in the liver lipolysis)” andis greate
“endogenous FA synthesis
“the (DNL:
release of de novo
FAs (FA lipogenesis)”
oxidation, lipolysis,inand
theFAliver is greater
secretion thanlow
in very “the
density lip
release of FAs (FA oxidation, lipolysis, and FA secretion
tein (VLDL)-TG)” from the liver (Figure 2). in very low density lipoprotein
(VLDL)-TG)” from the liver (Figure 2).
Figure 2.
Figure 2. NAFLD NAFLD development
development is caused by isancaused by an
imbalance imbalance
in the in the intrahepatocellular
intrahepatocellular fatty acid (FA) fatty acid Hepat
metabolism.
(FA) metabolism.
TG accumulation is promoted Hepatic
when theTG FAaccumulation is promoted
input is greater than thewhen the FA
FA output ininput is greater
the liver. than the
The greater FAof FA take
part
up by liveroutput
is mainly derived
in the fromgreater
liver. The the lipolysis
part of of
FAsubcutaneous adipose
taken up by liver tissue derived
is mainly TG. Another
from major sourceof
the lipolysis of FA in th
liver is derived from de novo lipogenesis that converts excess glucose into FAs. On the other
subcutaneous adipose tissue TG. Another major source of FA in the liver is derived from de novo hand, the consumption o
FA is possible through the signaling pathway involved in lipolysis, β-oxidation, and TG secretion
lipogenesis that converts excess glucose into FAs. On the other hand, the consumption of FA is (→: signaling pathway
related with TG accumulation by FA, →: signaling pathways related with the consumption of FA).
possible through the signaling pathway involved in lipolysis, β-oxidation, and TG secretion (→:
signaling pathways related with TG accumulation by FA, →: signaling pathways related with the
The release of FAs from adipose tissue and the efficiency of FA uptake by liv
consumption of FA).
increased in approximately 59% of patients with NAFLD [48]. Hepatic FA uptake de
The releaseonofplasma
FAs from FA adipose
concentration
tissue and
and on
thehepatocellular
efficiency of FAcapacity
uptakeforbyFA uptake
liver are that is
mined by the59%
increased in approximately number and activity
of patients of specialized
with NAFLD FA transporter
[48]. Hepatic FA uptake and carrier protein
depends
as FA translocase (FAT/CD36), FA transport polypeptide (FATP),
on plasma FA concentration and on hepatocellular capacity for FA uptake that is determined and FA binding p
by the number and activity of specialized FA transporter and carrier proteins suchCD36
(FABP) [49,50]. For example, hepatic expression of fatty acid translocase as is mar
FA translocase (FAT/CD36), FA transport polypeptide (FATP), and FA binding proteinand FAB
increased in subjects with NAFLD, and hepatic expression of FABP-4
(FABP) [49,50]. closely associated
For example, with
hepatic intrahepatic
expression TG accumulation.
of fatty acid translocase CD36 is markedly
In approximately 26% of patients
increased in subjects with NAFLD, and hepatic expression withofNAFLD,
FABP-4 theandway to provides
FABP-5 is closelyFA pool in
associated withisintrahepatic
de novo lipogenesis (DNL) [51]. DNL is the metabolic process that synthesizes ne
TG accumulation.
from excess
In approximately 26% glucose [52,53].
of patients withItNAFLD,
is an important
the waycontributor
to providestoward
FA poolhepatic
in liverlipid accu
is de novo lipogenesis (DNL) [51]. DNL is the metabolic process that synthesizes new of two
tion in the pathogenesis of NAFLD [52,53]. The effects result from activation
FAs from excessscription
glucose factors,
[52,53]. sterol
It is anregulatory
importantelement binding
contributor protein-1c
toward hepatic (SREBP-1c)
lipid accu- and car
drate responsive element binding protein (ChREBP),
mulation in the pathogenesis of NAFLD [52,53]. The effects result from activationboosted by insulin
of twoand gluco
transcription factors, sterol regulatory element binding protein-1c (SREBP-1c) and important
sponses to dietary carbohydrates [54,55]. They play a synergistically carbo- role
hydrate responsive element binding protein (ChREBP), boosted by insulin and glucose
responses to dietary carbohydrates [54,55]. They play a synergistically important role in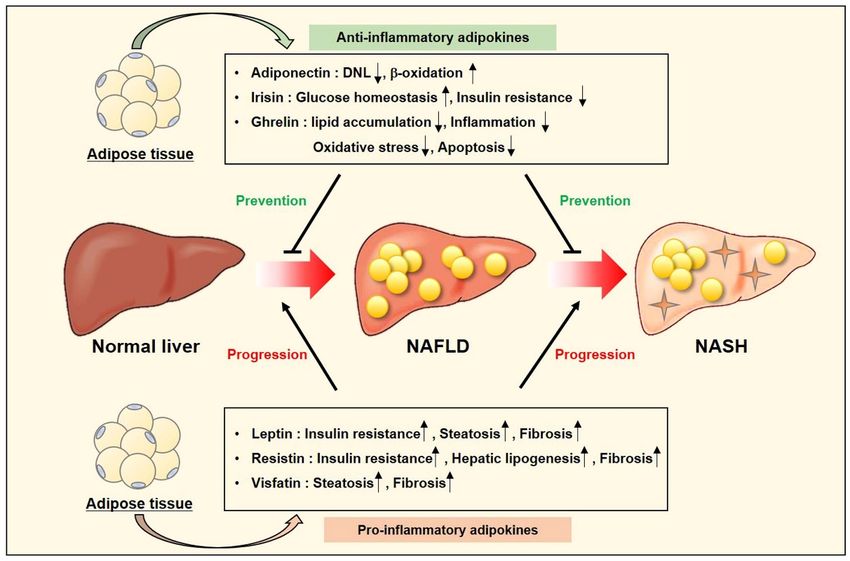
Int. J. Mol. Sci. 2021, 22, 4495 4 of 30
the coordinated regulation of hepatic DNL. In the remaining 15% of patients with NAFLD,
FA pool is derived from dietary TG, which is associated with chylomicrons [48].
The most acceptable theory in the pathogenesis of NAFLD is the “two-hit” hypothe-
sis [56]. The first hit is “insulin resistance” caused by excessive FA flux into the liver. The
second hit is “inflammation”, associated with gut-derived endotoxin, oxidative stress, and
mitochondria dysfunction. It is closely related with NAFLD progression toward NASH.
2.1.2. Endotoxin Behavior
NALFD and other insulin resistance-related diseases are associated with activation of
innate immune system, leading to chronic inflammation [57]. Recently, gut-derived endo-
toxins, such as lipopolysaccharide (LPS), have been proposed to have a critical role in liver
inflammation as well as progression of chronic liver diseases [58]. Under normal conditions,
endotoxin can be absorbed from the intestinal lumen into the portal vein system, and the
absorbed endotoxin will be rapidly removed in the hepatic reticuloendothelial system,
particularly Kupffer cells [59,60]. However, obesity, type 2 diabetes, and other nutrition
and environmental factors can alter intestinal permeability for bacterial overgrowth and
the resulting leaky mucosal barrier allows bacterial translocation, implicating the release of
gut-derived endotoxin into the systemic circulation [61,62]. The invasive pathogens and
harmful byproducts influence hepatic lipid accumulation and exacerbate pro-inflammatory
and fibrotic processes [60].
Recently, the role of LPS from gut microbiota in the development of NAFLD and NASH
has been attracting attention [63,64]. Circulating LPS levels, small intestinal permeability,
and bacterial overgrowth are increased in patients with NALFD, and these factors are
associated with the severity of hepatic steatosis [63,65,66]. Livers that directly receives
blood from the portal vein are the main target of LPS, also known as endotoxin, and
LPS-TLR4 is one of the critical pathways for NAFLD development. In mouse models, LPS
infusion triggers hepatic steatosis and hepatic insulin resistance, as well as hepatic weight
gain [67]. LPS exacerbates liver injury in mice fed a methionine-choline-deficient diet [68].
The LPS-binding protein (LBP)-CD14 complex activates Toll-like recpeotr4 (TLR4), which
is an essential inflammatory cascade in the progression of NAFLD [69,70]. Loss of LBP
attenuates inflammation-mediated liver damage [71]. TLR4 can activate NF-kB and release
pro-inflammatory cytokines such as interleukin-1β (IL-1β), tumor necrosis factor-α (TNF-
α), and IL-6 [72]. It can also recognize damage-associated molecular patterns (DAMPs)
that are released from damaged cells, and mediates FA-induced inflammation [57,73].
As pharmacological therapies in NAFLD and NASH targeting the microbiome, there are
IMM-24e (anti-LPS antibody), solithromycin (next-generation macrolide antbiotic), and
TLR4 antagonist [74].
2.1.3. Oxidative Stress
Chronic oxidative stress is one of the key mechanisms leading to liver injury in NAFLD.
Oxidative stress is a general event that occur in NAFLD and NASH as result of excessive
production of reactive oxygen species (ROS) [75,76]. ROS and lipid peroxidation can
explain most of histological features of NAFLD and NASH [77,78]. In patients with hepatic
steatosis, mitochondrial ROS oxidizes hepatic fat deposits, and ROS-induced expression
of Fas-ligand can induce apoptosis [77,78]. Peroxidation of and intracellular membranes
can directly trigger necrosis and apoptosis [77,78]. The degree of lipid peroxidation is
correlated with the severity of steatosis and can explain the association between steatosis
severity and the risk of necroinflammation and fibrosis in NASH [79–81]. ROS, which
plays a key player in the pathogenesis of NASH, can lead to a self-perpetuating cycle
of lipid peroxidation and can further generate ROS [82]. Lipid peroxidation products
alter mitochondrial DNA and activate transcription factor nuclear facto-kB (NF-kB) that
upregulates TNFα [83,84]. Resultingly, it further contributes to impaired mitochondrial
respiration and increased ROS formation [83,84].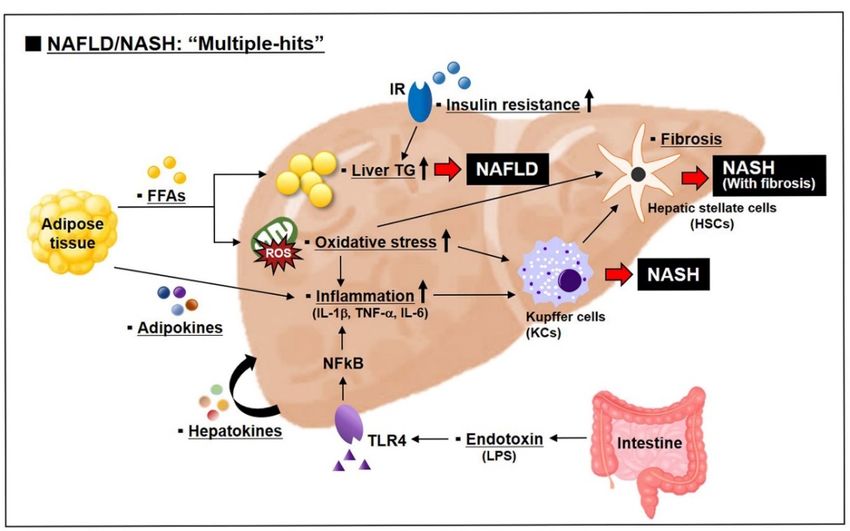
Int. J. Mol. Sci. 2021, 22, x FOR PEER REVIEW 5 of 30
Int. J. Mol. Sci. 2021, 22, 4495 5 of 30
Increased mitochondrial β-oxidation of FFA is an important source of ROS in NAFLD
and NASH [85]. Increased FFA flux in hepatic cells during early stages of NAFLD stimu-
Increased mitochondrial β-oxidation of FFA is an important source of ROS in NAFLD
late mitochondrial
and NASH [85]. Increased fatty acid
FFAoxidation
flux in hepatic(FAO), and
cells it reflects
during an early
early stages effort ofstimulate
of NAFLD the liver
compensatoryfatty
mitochondrial mechanisms to inhibit
acid oxidation (FAO),liverandfat it
accumulation
reflects an early andeffort
maintain
of the lipid
liverhomeosta-
compen-
sis [12]. In NAFLD and NASH, mitochondrial FAO is also
satory mechanisms to inhibit liver fat accumulation and maintain lipid homeostasis increased or at least preserved[12].
as NAFLD
In a compensatory
and NASH, response. The imbalance
mitochondrial FAO isbetween mitochondrial
also increased or at leastFAO and electron
preserved as a
transport chain
compensatory (ETC) will
response. Thecontribute
imbalanceto ROS overproduction
between mitochondrial FAO by increased
and electronelectron leak-
transport
age from the ETC [12,85,86]. ROS-induced lipid peroxidation
chain (ETC) will contribute to ROS overproduction by increased electron leakage from leads to inflammation and
hepatic
the ETCfibrogenesis through the activation
[12,85,86]. ROS-induced of hepatic leads
lipid peroxidation stellate tocells (HSCs) [87,88].
inflammation and hepatic
Recently, reliable circulating markers that can reflect
fibrogenesis through the activation of hepatic stellate cells (HSCs) [87,88]. oxidative stress in patients with
NAFLD have been reported. Urinary 8-iso-prostaglandin F2α (8-iso-PGF2α)
Recently, reliable circulating markers that can reflect oxidative stress in patients with is known as
a reliable indicator of oxidative stress in vivo [89,90], and
NAFLD have been reported. Urinary 8-iso-prostaglandin F2α (8-iso-PGF2α) is known as soluble NOX2-derived peptide
a(sNOX2-dp) are also
reliable indicator of an acceptable
oxidative stressmarker,
in vivowhich[89,90],is and
associated
solublewith ROS generation
NOX2-derived peptide by
activation of are
(sNOX2-dp) NOX2, also aanmember
acceptable of the NADPH
marker, which oxidase family [91,92].
is associated with ROS Elevated
generationlevelsby of
urinary 8-iso-PGF2α
activation of NOX2, aand serumofsoluble
member the NADPH NOX2-derived peptide[91,92].
oxidase family are considered
Elevatedas a relia-
levels of
ble indicator
urinary of oxidative
8-iso-PGF2α stresssoluble
and serum in chronic inflammation
NOX2-derived and metabolic
peptide are considered diseasesas a [93–95].
reliable
They alsoofcan
indicator be usedstress
oxidative as markers
in chronicof oxidative
inflammation stressand
for prediction of the severity
metabolic diseases [93–95].ofThey liver
damage in NAFLD [96,97]. LPS is an important outer membrane
also can be used as markers of oxidative stress for prediction of the severity of liver damage component of gram-neg-
ative
in NAFLDbacteria that induces
[96,97]. LPS is accelerated
an important inflammation
outer membrane and oxidative
component stressof[98,99]. Elevated
gram-negative
levels ofthat
bacteria circulating
induces NOX2 and LPS
accelerated in NAFLDand
inflammation patients suggest
oxidative stressthe potential
[98,99]. role of
Elevated gut-
levels
derived
of LPS in
circulating NOX2 systemic NOX2
and LPS activation
in NAFLD [100]. suggest
patients Further,the sNOX2-dp
potentiallevels
role ofare positively
gut-derived
related
LPS with the NOX2
in systemic histological grading
activation of steatosis,
[100]. inflammation,
Further, sNOX2-dp levelsballooning,
are positivelyfibrosis, and
related
with
NAFLD the histological
activity score grading
[100]. of steatosis, inflammation,
Gut-derived LPS can stimulate ballooning,
TLR4,fibrosis, and NAFLD
and TLR4-mediated
activity score [100].
NOXs activation can Gut-derived
generate ROSLPS can stimulateinfiltration
by macrophage TLR4, and TLR4-mediated
[101]. It can contribute NOXs to
activation can generate
hepatic steatosis ROS by
and insulin macrophage
resistance [101].infiltration [101]. It can contribute to hepatic
steatosis and insulin
However, resistance
the variety [101]. changes occurred in NAFLD are insufficient to be
of metabolic
However,
explained onlythe by variety of metabolic
the “two-hit” changes
hypothesis. occurred
Most in NAFLD
metabolic are insufficient
disorders such as obesity, to be
explained only bymetabolic
type 2 diabetes, the “two-hit” hypothesis.
syndrome, and Most metabolicare
dyslipidemia disorders
the risksuchfactorsas obesity,
for NAFLD type
2development.
diabetes, metabolic syndrome, and dyslipidemia are the risk
Recently, it has been thought that the development and progression of factors for NAFLD develop-
ment.
NAFLD Recently,
are induced it hasbybeen
thethought that the involving
“multiple-hits” development and progression
various factors (Figure of NAFLD
3) [102,103]. are
induced by the “multiple-hits” involving various factors (Figure
The “multiple-hits” include bioactive molecules secreted from the adipose tissue, nutri- 3) [102,103]. The “multiple-
hits”
tionalinclude
factors,bioactive molecules secreted
and environmental from the adipose tissue, nutritional factors, and
factors [102].
environmental factors [102].
Figure 3. Multiple-hits
Figure Multiple-hitspathogenesis
pathogenesisofof
NAFLD
NAFLD and NASH.
and NAFLD
NASH. NAFLD begins withwith
begins hepatic lipidlipid
hepatic ac-
cumulation and insulin resistance, and progresses to NASH with the concert of various factors
accumulation and insulin resistance, and progresses to NASH with the concert of various factors
such as inflammation, endotoxin, organokines (adipokines and hepatokines), and oxidative stress. (:
Factors related with multiple-hits).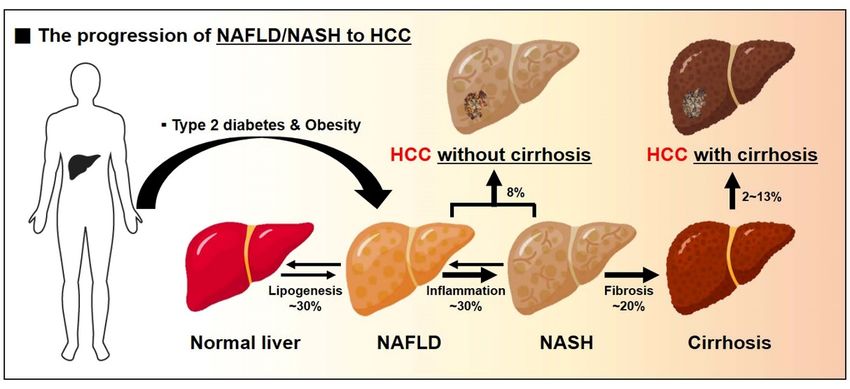
Int. J. Mol. Sci. 2021, 22, x FOR PEER REVIEW 6 of 30
such as inflammation, endotoxin, organokines (adipokines and hepatokines), and oxidative stress.
Int. J. Mol. Sci. 2021, 22, 4495 6 of 30
(▪: Factors related with multiple-hits).
2.2. Promising Therapies in NAFLD and NASH
2.2. Promising Therapies in NAFLD and NASH
As recently recommended pharmacotherapies, it has been reported that pioglitazone
As recently recommended pharmacotherapies, it has been reported that pioglitazone and
and high dosage vitamin E effectively improve the histology of patients with NASH [104–
high dosage vitamin E effectively improve the histology of patients with NASH [104–106]. On
106]. On the other hand, metformin does not recover liver histology of patients with
the other hand, metformin does not recover liver histology of patients with NAFLD [107,108],
NAFLD [107,108], and ursodeoxycholic acid (UDCA) does not improve liver histology,
and ursodeoxycholic acid (UDCA) does not improve liver histology, inflammation, or fibrosis
inflammation, or fibrosis of patients with NASH [109–111]. Below are some of pharmaco-
of patients with NASH [109–111]. Below are some of pharmaco-therapeutic options that are
therapeutic options
in clinical trials thatbe
or could are in clinical
good trialsfor
candidates orNASH
could treatment
be good candidates
(Figure 4). for NASH treat-
Additionally, the
ment (Figure 4). Additionally, the metabolic profile and liver histology-related
metabolic profile and liver histology-related efficacy of these promising drugs in humans efficacyare
of
these promising drugs
summarized in Table 1. in humans are summarized in Table 1.
Figure 4. Current therapeutic targets for pharmacological treatment of NAFLD and NASH. There are no FDA-approved
medications for
medications for patients
patients with
with NAFLD/NASH
NAFLD/NASH so so far.
far. Currently,
Currently, various
various pharmacological
pharmacological therapeutic
therapeutic candidates
candidates are being
are being
applied to the clinical trials. The illustration demonstrates the targeted pathway and phenotype for treatment of patients
applied to the clinical trials. The illustration demonstrates the targeted pathway and phenotype for treatment of patients
with NAFLD and NASH.
with NAFLD and NASH.
2.2.1. Pioglitazone
Pioglitazone
Pioglitazone is one of the anti-diabetic agents of the thiazolidinediones (TZDs) class
used in the management of type 2 diabetes [112]. TZDs TZDs is is also
also known
known as “glitazones”.
“glitazones”.
are two
There are twoTZDs,
TZDs,rosiglitazone
rosiglitazoneand and pioglitazone,
pioglitazone, which
which areare currently
currently approved
approved by
by the
the FDA
FDA as monotherapy
as monotherapy or combined
or combined therapies
therapies with with metformin
metformin and sulfonylureas
and sulfonylureas for
for man-
managing
aging type type 2 diabetes
2 diabetes [113].[113].
TZDs, TZDs, as insulin
as insulin sensitizers,
sensitizers, help regulate
help regulate glycemia
glycemia and
and insu-
insulin
lin resistance
resistance [113].[113]. The most
The most important
important advantage
advantage of TZD ofisTZD
thatisitthat
doesitnot
does not hypo-
cause cause
hypoglycemia
glycemia with single
with single therapy,therapy, and there
and there are noare no contraindications
contraindications for patients
for patients with
with renal
renal disease
disease [114]. [114].
TZDs regulates metabolic pathways
TZDs pathways by binding to the nuclear transcription factor
peroxisome proliferator-activated
peroxisome proliferator-activated receptor receptor gamma
gamma (PPARγ)
(PPARγ) and and modulating
modulating target
target gene
gene
expression [115]. The genes play a role in glucose metabolism, FA storage, and adipocyte
expression [115]. The genes play a role in glucose metabolism, FA storage, and adipocyte
differentiation [116].
differentiation [116]. InIn line
line with
with this,
this, PPARγ
PPARγ agonists
agonists increase
increase glucose
glucose transporter
transporter 44
(GLUT4, also
(GLUT4, alsoknown
knownasasSLC2A4)
SLC2A4) expression
expression andand
translocation,
translocation,inhibit TNF-α,
inhibit and enhance
TNF-α, and en-
insulin sensitivity in insulin-sensitive organs [117,118]. On the other
hance insulin sensitivity in insulin-sensitive organs [117,118]. On the other hand, TZD hand, TZD therapy
leads to leads
therapy weight togain as again
weight sideas effect,
a sidebecause
effect, PPARγ
becausereceptors are highlyare
PPARγ receptors expressed in
highly ex-
adipocytes [119]. Increases in fat mass are exclusively limited to the subcutaneous
pressed in adipocytes [119]. Increases in fat mass are exclusively limited to the subcuta- adipose
depot rather
neous adiposethandepotthe rather
visceral spot
than the[117,120].
visceral They can be improved
spot [117,120]. They can bybe treatment
improved with
by
metformin [121,122].
treatment with metformin [121,122].
Recently, it was reported that the PPARγ agonist Pioglitazone has significant effects
on NAFLD/NASH patients. In NASH patients, it improves liver fat accumulation and
fibrosis [123,124]. In NASH patients with type 2 diabetes, it reduces hepatic steatosis, in-Int. J. Mol. Sci. 2021, 22, 4495 7 of 30
flammation, and the serum alanine aminotransferase (ALT) and aspartate aminotransferase
(AST) levels and improves the liver [125]. In rodent models, it reduces hepatic gluconeo-
genesis, and improves insulin sensitivity in the liver and other peripheral tissues [126]. It
also improves hepatic fibrosis [126].
2.2.2. Obeticholic acid (OCA, Also Known as INT-747; FXR Agonist)
OCA is a potent and selective agonist of farnesoid X receptor (FXR), a nuclear receptor
that can regulate hepatic glucose and lipid metabolism, inflammation, and lipoprotein
composition as well as bile acid synthesis [127,128]. In rodent models, OCA exerts the HSCs
and macrophages anti-inflammatory and anti-fibrotic effects [129,130]. The transcriptional
repressor small or short heterodimer partner (SHP) interacts with liver receptor homolog-1
(LRH-1), a positive regulator of CYP7A1 that encodes the rate-limiting enzyme in the classic
bile acid synthesis pathways, and suppresses its transcriptional activity [131]. Exposure of
HSCs to FXR ligands increases the transcriptional repressor SHP expression and reduces
factors associated with liver fibrosis [130]. It is thought that an FXR-SHP regulatory axis
plays an important role in regulating liver fibrosis. OCA-induced FXR activity is 100-fold
more potent than human natural FXR agonist, chenodeoxycholic acid (CDCA) [132]. OCA
increases insulin sensitivity and reduces markers related with hepatic inflammation and
fibrosis in patients with type 2 diabetes and NAFLD [133]. OCA leads to weight loss in
patients with NASH, and weight loss caused by OCA is shown to exert additively beneficial
effects on serum aminotransferase and liver histology [134]. Additionally, it significantly
improves fibrosis in NASH patients [135]. It is one of the most promising drugs for treating
NASH and is now in phase 3 clinical trials [136].
2.2.3. Elafibranor (GFT505; PPARα/δ Agonist)
PPARs are ligand-activated transcription factors of nuclear hormone receptor su-
perfamily [137]. They are expressed in the liver, adipose tissue, skeletal muscle, heart,
and kidney, and regulate metabolic pathways including β-oxidation and gluconeogen-
esis [136]. There are three nuclear receptor isoforms: PPAR alpha (α), PPAR delta (δ),
and PPAR gamma (γ). PPARα promotes β-oxidation, reduces TG levels, and increases
high-density lipoprotein (HDL) cholesterol [138]. It also inhibits NF-kB-induced inflam-
matory genes [138]. PPARα agonist, in forms such as fibric acid derivatives (fibrates), is
broadly used for treatment of hypertriglycemia, whereas it has no significant effects on
patients with NAFLD [139]. This is considered to be because PPARα receptors are present
in other organs as well as the liver. Similar to PPARα, PPARδ increases FA oxidation and
additionally reduces activation of macrophages and Kupffer cells because it is present in
macrophages [140]. GW501516 is a synthetic PPARδ-specific agonist [141,142]. GW501516
might be considered as a promising therapy in clinical trials because of its potent efficacy,
but it has safety concerns [143].
Elafibranor, also known as GFT505, is a dual PPARα/δ agonist [144]. It improves
inflammation, apoptosis, and necroptosis in the NASH mouse model [145]. It reduced
histopathologically hepatic steatosis and inflammation, and reduced fibrosis severity in
both NAFLD/NASH and fibrosis mouse models [146,147]. It tends to reduce body weight,
but not liver weight in diet-induced NAFLD/NASH rodent models [148,149]. In obese
patients, it improves hepatic and peripheral insulin sensitivity [150]. Further, it inhibits
proinflammatory (IL-1β, TNF-α, and F4/80) and profibrotic (transforming growth factor-β
(TGF-β), tissue inhibitor of metalloproteinase 2, collagen type I, alpha 1, and collagen
type I, alpha 2) markers in obese patients [151]. In addition, it decreases liver dysfunction
markers such as ALT and alkaline phosphatase (ALP) [146,151]. It did not cause weight
gain [144,152]. It is currently being evaluated in a pivotal phase 3 clinical trials in NASH
patients [136].Int. J. Mol. Sci. 2021, 22, 4495 8 of 30
2.2.4. Arachidyl Amido Cholanoic Acid (Aramchol)
Aramchol is the liver targeted, oral stearoyl-CoA desaturase 1 (SCD1) inhibitor [153]. It
is a novel fatty acid bile acid conjugate (FABACs) [153]. In rodents, aramchol affects liver fat
metabolism by reducing FA synthesis and increasing β-oxidation [154,155]. Furthermore,
aramchol activates cholesterol efflux by stimulating the ATP-binding cassette transporter
A1 (ABCA1) [156]. In addition, it reduces inflammation and fibrosis in methionine and
choline deficient (MCD) fed mice [153]. Additionally, it improves steatohepatitis and
fibrosis by decreasing SCD1 levels and by regulating the transsulfuration pathway, leading
to a rise in glutathione (GSH) levels and the glutathione disulfide (GSSG)/GSH redox
couple to properly balance the redox environment [153]. Weight loss by aramchol treatment
is known to stabilize within 1 week [153].
In in a phase 2 trial of patients with NAFLD, aramchol reduces the liver fat content
and improves liver histology [157]. There was no significant toxicity as determined by the
circulating ALT, AST, and alkaline phosphatase levels [157]. Because it targets both the
general characteristics of NASH (excessive liver fat contents, lipotoxicity, and oxidative
stress) and fibrosis [153], aramchol is currently being developed for the treatment of NASH
and fibrosis. It is known that there were no significant changes in the body weight of
NASH patients. Phase 3 clinical trials in patients with NASH and fibrosis were initiated in
2019 and are ongoing.
2.2.5. Liraglutide (GLP-1R Agonist)
Glucagon-like peptide-1 receptor (GLP-1R) agonists are well established as an effective
medication showing promising anti-diabetic effects in both animal models and patients
with type 2 diabetes [158–160]. GLP-1 is a incretin hormone that is secreted from L-cells in
the distal ileum and colon [161]. It stimulates the pancreas, leading to insulin biosynthesis
and insulin secretion, and reduces glucagon production [162,163]. Endogenous GLP-1
is degraded within a few minutes by the dipeptidyl peptidase-4 (DPP-4) enzyme, but
liraglutide works for a long time, with a half-life of 13 h [164].
Exenatide, a synthetic exendin-4, was the first GLP-1R agonist approved by the FDA
in 2005 for the treatment of type 2 diabetes, as monotherapy or as add-on treatment to
metformin and/or sulfonylurea where control was inadequate [165].
Liraglutide is the second GLP-1R agonist to be licensed the FDA in 2010 for the
treatment of type 2 diabetes. It is also received FDA approval in 2020 as a treatment for
obesity patients, based on its lasting weight loss benefits [166,167]. It has cardiovascular
safety in treatment for weight management [168]. Liraglutide-induced anorexia is also
related with glutamatergic POMC neuron, leading to weight loss [169]. In patients with
NAFLD and NASH, it decreases liver fat contents and improves histological resolution
and serum liver enzyme levels without worsening fibrosis [170,171]. It is thought that
the effect of liraglutide on weight loss and reduced cardiovascular risk is critical for
treatment of NAFLD because the development of NAFLD is based on lipotoxicity and
insulin resistance [171,172]. As studies associated with NAFLD and NASH in rodents
showed, liraglutide protects pancreatic β-cells from apoptosis through AKT-mediated
survival signaling [173]. It improves insulin sensitivity by activating AMP-activated protein
kinase (AMPK) and reduces liver steatosis by modulating lipid transport, β-oxidation,
DNL, and autophagy [174–176].
2.2.6. Selonsertib (ASK1 Inhibitor)
Ballooned hepatocytes, implicating activation of the apoptotic pathway, are a hall
marker of NASH and fibrosis progression [177,178]. Selonsertib is a first-in-class inhibitor
of the apoptosis signal regulating kinase 1(ASK1) [179]. It inhibits the phosphorylation
and activation of ASK1 by binding to the catalytic kinase domain of ASK1. Recently, it
has proposed as therapeutic potential for fibrotic diseases. In mouse models, ASK1, a
serine/threonine signaling kinase, causes phosphorylation of p38 mitogen-activated kinase
and c-Jun N-terminal kinase (JNK), leading to activation of stress response pathways thatInt. J. Mol. Sci. 2021, 22, 4495 9 of 30
aggravate hepatic inflammation, apoptosis, and fibrosis [180–182]. In mouse models of
NASH, it significantly improves not only liver steatosis and fibrosis associated with NASH
but also cholesterol, bile acid, and lipid metabolism [180]. In phase 2 clinical trials of
patients with NASH and stage 2–3 fibrosis, it has been shown to prevent inflammation,
fibrosis, excessive apoptosis, and progression to cirrhosis [183]. On the other hand, phase 3
clinical trials of patients with NASH and advanced fibrosis were found to improve liver
histology, but did not affect fibrosis regression [184,185]
2.2.7. Simtuzumab (SIM, G6624)
SIM is a monoclonal antibody targeting the lysyl oxidase-like 2 (LOXL2) enzyme that
catalyzes the crosslinkage of collagen and elastin, leading to remodeling of the extracel-
lular matrix [186,187]. SIM binds to LOXL2 and inhibits its enzymatic activity [188]. As
a result, it inhibits synthesis of growth factors including connective tissue growth fac-
tor (CTGF/CCN2) and TGFβ1, and reduces liver fibrosis [189]. In a mouse model with
advanced fibrosis, SIM has an additive effect in combination with ASK1 inhibitor [183].
However, in phase 2b clinical trials of subjects with advanced fibrosis induced by NASH,
it was no effect on improving fibrosis and cirrhosis confirmed by hepatic collagen con-
tent [190].
2.2.8. Cenicriviroc (CVC; Dual CCR2/CCR5 Antagonist)
Liver inflammation is closely associated with chemokines that regulate activities
and migration of hepatocytes and immune cells [191]. The C-C chemokine receptors
CCR2 and CCR5 with their respective ligands (CCL2 and CLL3-5) are associated with
the pathogenesis of liver inflammation and fibrosis for the development of NAFLD and
NASH [191–193]. CCR2 and its ligand CCL2 enhances hepatic steatosis, macrophage
accumulation, inflammation, and fibrosis [191]. Activated HSCs, a contributor for fibrosis,
secretes CCL5. CCL5 exerts profibrotic activity in hepatocytes via its receptors CCR5 and
induces lipid accumulation and pro-inflammatory factors [192].
CVC is a novel and potent antagonist of CCR2 and CCR5 that is currently in clinical
development for treatment of liver fibrosis in patients with NASH [194,195]. CVC reduces
levels of inflammation markers including IL-1β and IL-6 and exerts anti-fibrotic activi-
ties [194,195]. It received Fast Track designation by the FDA in 2015 as a promising therapy
for NASH and liver fibrosis. In the phase 2b study of subjects with NASH and stage 2–3
fibrosis, CVC has shown improvement in liver fibrosis without worsening NASH [196].
Currently, phase 3 clinical trials are ongoing to evaluate and confirm the efficacy and safety
of CVC for the treatment of liver fibrosis in patients with NASH [197].
2.3. Diagnostic and Therapeutic Targets in NAFLD and NASH: Adipokines
Recently, it has been believed that NAFLD and NASH are caused by the multiple
factors [102,103]. Among them, we will focus on adipokines secreted from adipose tissues
that provide FA as the major source for NAFLD development [48]. Several adipokines
are involved in the pathogenesis and progression of NAFLD [198]. Leptin, resistin, and
visfatin play a role in NAFLD development and progression to NASH [199–204]. On
the other hand, adiponectin, irisin, and ghrelin exert beneficial effects on NAFLD and
NASH [205–211]. Pharmacological agents that affect liver histology and pathophysiology
could be influential in theses adipokine levels. It suggests that adipokines can be attractive
targets for treatment and can be biomarkers for prediction of NAFLD severity (Figure 5).
Adipokines can also play an active role in the development of HCC.
Table 1. Summary of promising drugs for NAFLD/NASH.
Clinical Stage
Name of Drug Mechanism of Action Metabolic Profile Liver Histology Ref.
(Title of Trial)
Insulin sensitivity(↑) Steatosis(↓)
Hepatic TG(↓) Ballooning(↓)
Pioglitazone PPAR γ agonist ALT(↓) Inflammation(↓) Phase 4 trial, 2008–2014 [104,105,125,212,213]
AST(↓) Fibrosis(↓)
BW(↑) NAS(↓)
Insulin sensitivity(↑)
ALT(↓) Steatosis(↓)
Phase 3 trial, ongoing
AST(↓) Ballooning(↓)
since 2017
Obeticholic acid (OCA) FXR agonist ALP(↑) Inflammation(↓) [214,215]
(REGENERATE,
HDL-C(↓) Fibrosis(↓)
REVERSE)
LDL-C(↑) NAS(↓)
BW(↓)Int. J. Mol. Sci. 2021, 22, 4495 10 of 30
Table 1. Cont.
Clinical Stage
Name of Drug Mechanism of Action Metabolic Profile Liver Histology Ref.
(Title of Trial)
Insulin sensitivity(↑)
Plasma TG(↓)
Steatosis(↓) Phase 3 trial, ongoing
ALT(↓)
Elafibranor Dual PPARα/δ agonist Inflammation(↓) since 2016 [144,150,151]
AST(-)
Fibrosis(↓) (RESOLVE-IT)
ALP(↓)
BW(-)
Insulin sensitivity(↑)
Hepatic TG(↓)
Steatosis(↓) Phase 3 trial, ongoing
Aramchol SCD1 inhibitor ALT(-) [157]
Fibrosis(↓) since 2019 (ARMOR)
AST(-)
BW(-)
Insulin sensitivity(↑)
Hepatic TG(↓) Phase 3 trial, ongoing
Steatosis(↓)
Liraglutide GLP-1R agonist ALT(↓) since 2014 [164,216,217]
Ballooning(↓)
AST(-) (CGH-LiNASH)
BW(↓)
Steatosis(↓)
ALT(↓) Ballooning(↓) Phase 3 trial, ongoing
Selonsertib ASK1 inhibitor AST(↓) Inflammation(↓) since 2019 (STELLAR3, [93]
BW(-) Fibrosis(↓) STELLAR4)
NAS(↓)
ALT(-)
LOXL2 monoclonal
Simtuzumab (SIM) AST(-) Fibrosis(-) Phase 2 trial, 2012–2017 [218,219]
antibody
BW(-)
ALT(-)
Dual CCR2/CCR5 Inflammation(↓) Phase 3 trial, ongoing
Cenicriviroc (CVC)Int. J. Mol. Sci. 2021, 22, x FOR PEER REVIEW AST(-) [196] 11
antagonist Fibrosis(↓) since 2017 (AURORA)
BW(-)
((↑): increase, (↓): decrease, (-): no significant).
Figure 5. Adipokines
Figure 5. as diagnostic as
Adipokines markers and therapeutic
diagnostic markers andtargets in NAFLD
therapeutic and NASH.
targets Adipokines
in NAFLD that are secreted
and NASH.
from adipose tissues are
Adipokines classified
that into anti-inflammatory
are secreted adipokines
from adipose tissues and pro-inflammatory
are classified adipokines.
into anti-inflammatory Anti-inflamma
adipokines
tory adipokines including adiponectin, irisin, and ghrelin inhibit the development and progression of NAFLD and NASH
and pro-inflammatory adipokines. Anti-inflammatory adipokines including adiponectin, irisin, and
whereas pro-inflammatory adipokines including leptin, resistin, and visfatin promote the development and progression
ghrelin inhibit the development and progression of NAFLD and NASH, whereas pro-inflammatory
of NAFLD and NASH.
adipokines including leptin, resistin, and visfatin promote the development and progression of
NAFLD and NASH. 2.3.1. Adiponectin
2.3.1. Adiponectin Adiponectin is an important adipokine that can inhibit NAFLD development. C
lating
Adiponectin is anadiponectin levels werethat
important adipokine decreased in patients
can inhibit NAFLDwith NAFLD and
development. NASH [220–
Circu-
lating adiponectin levels were decreased in patients with NAFLD and NASH [220–222].inflamma
These are inversely correlated with the severity of hepatic steatosis and
Pioglitazone, an anti-diabetic drug of thiazolidinedione-type, improves liver histo
and increases adiponectin levels in patients with NASH [104,125]. However, metfo
the most commonly used anti-diabetic medication, has no significant effects on the
histology of patients with NAFLD and NASH, and reduces adiponectin l
[107,108,223]. Vitamin E is a potent antioxidant that protects our cells against oxidInt. J. Mol. Sci. 2021, 22, 4495 11 of 30
These are inversely correlated with the severity of hepatic steatosis and inflammation.
Pioglitazone, an anti-diabetic drug of thiazolidinedione-type, improves liver histology
and increases adiponectin levels in patients with NASH [104,125]. However, metformin,
the most commonly used anti-diabetic medication, has no significant effects on the liver
histology of patients with NAFLD and NASH, and reduces adiponectin levels [107,108,223].
Vitamin E is a potent antioxidant that protects our cells against oxidative stress [224]. It is
an alternative medicine that is recommended in NAFLD and NASH. Vitamin E improves
liver histology and shows some beneficial effects in non-diabetic patient with NASH,
and also seems to increase adiponectin levels [225,226]. However, it has been found to
be ineffective alone in NASH patients with type 2 diabetes [226,227]. In mouse models,
adiponectin suppresses hepatic lipid accumulation by enhancing FA oxidation and re-
ducing DNL [206,228,229]. It exerts anti-inflammation, anti-fibrotic, and anti-apoptotic
effects [229]. Administration of adiponectin improves hepatic steatosis and inflamma-
tion [228,229]. Additionally, adiponectin expression is inversely correlated with tumor size
and local recurrence [230,231].
2.3.2. Leptin
Leptin is an appetite-suppressing hormone secreted by fat cells. It regulates food in-
take, body fat, and insulin sensitivity [232]. In animal models, it is thought that it improves
lipid metabolism in non-adipose tissues [233]. In the liver, however, it exacerbates hepatic
insulin resistance, which results in liver steatosis. It also enhances liver fibrosis [199,233].
Leptin administration can enhance pro-inflammatory and fibrogenic responses in the liver
via procollagen I and TGFβ1 [234]. In humans, however, its effects are unclear. Circulating
leptin levels are increased in patients with NASH [235,236]. Leptin levels are positively
correlated with steatosis severity, whereas it is unclear between leptin levels and the pro-
gression of inflammation and fibrosis [235–238]. Leptin expression is positively correlated
with cell proliferation in HCC, as confirmed by proliferation marker protein Ki67 [231].
2.3.3. Resistin
Resistin is a proinflammatory adipocyte-derived mediator of hepatic insulin resis-
tance [239,240]. It is also expressed in liver cells. Resistin is associated with hepatic
lipogenesis and liver fibrosis [241]. Circulating resistin levels are increased in patients with
NAFLD and NASH, and circulating resistin levels in patients with NAFLD are related to the
severity of steatosis, inflammation, and fibrosis [202,242,243]. Increased resistin levels are
thought to be associated with insulin resistance. In individuals with NAFLD, pioglitazone
treatment improves insulin sensitivity, and decreases plasma resistin levels [244].
2.3.4. Ghrelin
Ghrelin is an anti-inflammatory adipokine. It is an endogenous ligand for growth
hormone secretagog receptor with a peptide structure that contains 28 amino acids [245]. In
patients with NAFLD, lower ghrelin levels are associated with insulin resistance [246,247].
Plasma ghrelin levels are significantly correlated with liver function. However, ghrelin
is not affected by pioglitazone as one of insulin sentizers [45]. During and after NAFLD
development, ghrelin administration improves hepatic lipid metabolism, inflammation,
oxidative stress, and apoptosis [210]. In mouse models, ghrelin reduces the TG content and
the cytokins TNF-α and IL-6, and attenuates lipotoxicity through autophagy sitimulation
and NF-kB inhibition [248]. Collectively, ghrelin could be a biomarker for diagnosis and a
therapeutic target for treatment of NALFD.
2.3.5. Irisin
Irisin is a myokine secreted from skeletal muscle upon shivering and exercise stimula-
tion [249]. Fibronectin type III domain containing 5 precursors (FNDC5) is the precursor
of irisin. FNDC5/irisin promotes the thermogenic program in adipose tisseus through
ERK and p38 pathways [250]. It improves glucose homeostasis and insulin resistance, andInt. J. Mol. Sci. 2021, 22, 4495 12 of 30
induces weight loss [251]. Recently, FNDC5/irisin was induced during adipocyte differen-
tiation, and can be over-secreted from human obese visceral (VAT) and subcutaneous (SAT)
adipose tissues [252]. It is thought of as a compensatory effect. In line with this, circulating
irisin levels are increased in patients with NAFLD, and are positively related with portal
inflammation [218]. They are also believed to act as a compensatory effect.
2.3.6. Visfatin
Visfatin is one of the proinflammatory adipokines. Serum visfatin levels are raised in
type 2 diabetes and insulin resistant conditions [253,254]. Circulating visfatin levels are also
increased in patients with NAFLD, and are associated with the severity of hepatic steatosis
and fibrosis [204,255]. However, they are not affected by insulin sensitizers including
pioglitazone, rosiglitazone, and metformin [256,257].
3. NAFLD/NASH-Derived HCC
3.1. The Pathogenesis of NAFLD/NASH-Derived HCC
HCC is the third most common cause of cancer-related mortality [258]. NAFLD and
NASH-related HCC is the fastest growing indication for liver transplantation [259,260].
Cirrhosis is only present in approximately 60% of patients with NAFLD and NASH-
associated HCC [259]. This suggests that HCC can be induced from NAFLD/NASH
without cirrhosis. Therefore, it is thought that “inflammatory factors” will also play a
critical role in NAFLD/NASH-derived HCC.
3.1.1. Gut-Derived Endotoxin
As mentioned above, gut-derived endotoxins as alternative inflammatory factors play
an important role in the development of NAFLD and NASH. The levels of LPS, known as
endotoxins, are also increased in portal and peripheral veins of patients with HCC [261].
They significantly promote the invasive potential and induce the epithelial-mesenchymal
transition (EMT), although they also inhibit tumor growth [262]. LPS activates JNK and
MAPK via TLR4 in HCC cells, whereas inhibition of JNK/MAPK significantly reduces
EMT occurrence [262]. Therefor, the LPS-TLR4 signaling could be one of the promising
pathways regulating the progression from NAFLD to NASH to HCC [263].
3.1.2. Adipokines
Adipokines are inflammatory factors related with HCC development. Adiponectin
expression in human HCC is inversely correlated with tumor size [230]. It enhances
phosphorylation of c-Jun N-terminal kinase (JNK) and activates caspase-3, leading to
apoptosis in HCC [230]. Inhibition of JNK phosphorylation prevents anti-apoptotic effects
of adiponectin [230]. Adiponectin exerts chmoprotective and hepatoprotective effects
via sulfatase2 (SULF2) in HCC [264]. Loss of adiponectin promotes fibrosis and HCC
progression in a cholin-deficient NASH mouse model [265]. On the other hand, high levels
of circulating adiponectin make it possible to predict the consecutive development of HCC
and poor HCC survival [266,267]. Further, adiponectin inhibits the oncogenic effects of
leptin on cell proliferation, migration, and invasion in HCC [231].
Leptin expression is increased in both hepatoma tissues and cell lines [268]. Regulatory
T-cells (Tregs), effector CD4(+), and CD8(+) T-cells stimulate expression of the leptin
receptor (LEPR) in the liver after HCC induction [268]. Macrophage and dendritic cells
upregulate LEPR expression on the T-cell. Leptin inhibits Treg activation and function [268].
Increased leptin expression in HCC is associated with the expression of human telomerase
reverse transcriptase (hTERT) [269]. Leptin might play a critical role in obesity-related
tumorigenesis. Adipokines including adiponectin and leptin represent key players in
obesity-related disorders and might be involved in the pathogenesis of NAFLD and HCC.Int. J. Mol. Sci. 2021, 22, 4495 13 of 30
3.2. Diagnostic and Therapeutic Targets in NAFLD/NASH-Derived HCC: Hepatokines
The liver is a secretory organ that releases specific cytokines, termed hepatokines [43].
Adipose tissues in NAFLD, characterized by hepatic TG accumulation, play a critical
role in promoting FFA uptake into the liver through lipolysis [48]. Therefore, the role of
adipokines from adipose tissues, which provide the major energy source for the devel-
opment of NAFLD, will be very important in the liver. On the other hand, lipid droplet
accumulation itself does not affect inflammation and is considered as simple steatosis.
The progression from NAFLD to NASH to HCC needs additional factors such as oxida-
tive stress, mitochondrial dysfunction, and ER-stress [75,270,271]. Another important
factor driving NASH in simple steatosis is free non-esterified cholesterol and its oxidized
derivatives [272–274]. They are cytotoxic and exert synergistic effects with TNF, which is
Int. J. Mol. Sci. 2021, 22, x FOR PEER REVIEW
markedly increased in patients with NASH [274]. Therefore, hepatokines secreted from 14 ofthe
30
liver might exert a more potent ability in the progression of NAFLD and NASH to HCC
(Figure 6).
Figure 6. Hepatokines that
that are
are secreted
secretedfrom
fromthe
theliver
liverare
areclosely
closelyassociated
associatedwith
withthe
theprogression
progressionfrom NAFLD
from NAFLDto to
NASH
NASHto
to HCC.
HCC. Hepatokines
Hepatokines including
including Fetuin-A,
Fetuin-A, Fetuin-B,RBP4,
Fetuin-B, RBP4,and
andFGF19
FGF19play
playan
animportant
importantrolerolein
inNAFLD
NAFLD and
and NASH. They
are associated with
are associated with hepatic
hepatic lipid
lipid accumulation,
accumulation, insulin
insulin resistance,
resistance, and
and inflammatory
inflammatory signaling
signaling pathways.
pathways. Additionally,
Additionally,
ANGPTL4 and 8 tend to function in opposite ways in HCC tumorigenesis.
ANGPTL4 and 8 tend to function in opposite ways in HCC tumorigenesis.
(Fetuin-A and Fetuin-B)
α2-HS-Glycoprotein (Fetuin-A
3.2.1. α2-HS-Glycoprotein
Fetuin-A, one
Fetuin-A, one of
of the liver secreted glycoproteins, is known as the first hepatokine
shown
shown to associated with metabolic diseases [275,276]. Fetuin-A is positively associated
with hepatic steatosis and insulin resistance [277–279]. Its levels are increased in patients
with NAFLD,
with NAFLD, NASH,
NASH, and and type
type 22 diabetes
diabetes [280,281]. As an
[280,281]. As an important source of
important source of NAFLD
NAFLD
development, FFA
development, FFAenhances
enhancespro-inflammatory
pro-inflammatoryFetuin-A
Fetuin-A expression
expression [7].[7]. FFA-induced
FFA-induced Fe-
Fetuin-A
tuin-A functions
functions asas
anan endogenousligand
endogenous ligandofofToll-like
Toll-likereceptor
receptor44(TLR4),
(TLR4), and
and exacerbates
exacerbates
lipid-mediated insulin
lipid-mediated insulin resistance
resistance [282,283].
[282,283]. FFA
FFA can
can also
also enhances NF-kB recruitment
enhances NF-kB recruitment to
to
the Fetuin-A promoter and increases synthesis and the secretion of Fetuin-A in primary
hepatocytes [284]. Pioglitazone significantlly suppresses serum Fetuin-A levels in patients
with type 2 diabetes [285]. Pioglitazone inhibits mRNA and protein levels of hepatic Fe-
tuin-A, and oral administration of pioglitazone in mice partially ameliorates insulin re-
sistance with decreases on hepatic fetuin-A expression [286]. These data suggest that Fe-You can also read

















































