Nuclear grade and comedo necrosis of ductal carcinoma in situ as histopathological eligible criteria for the Japan Clinical Oncology Group 1505 ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Japanese Journal of Clinical Oncology, 2021, 51(3)434–443
doi: 10.1093/jjco/hyaa235
Advance Access Publication Date: 8 January 2021
Original Article
Original Article
Nuclear grade and comedo necrosis of ductal
carcinoma in situ as histopathological eligible
criteria for the Japan Clinical Oncology Group
Downloaded from https://academic.oup.com/jjco/article/51/3/434/6070012 by guest on 19 November 2021
1505 trial: an interobserver agreement study
Hitoshi Tsuda 1 ,*, Masayuki Yoshida2 , Futoshi Akiyama3 , Yasuyo Ohi4 ,
Keiichi Kinowaki5 , Nobue Kumaki6 , Yuzuru Kondo7 , Akihisa Saito8 ,
Eiichi Sasaki9 , Rieko Nishimura10 , Satoshi Fujii11,12 , Keiichi Homma13 ,
Rie Horii3 ,14 , Yuya Murata15 , Makiko Itami16 , Sabine Kajita17 ,
Hiroyuki Kato18 , Masafumi Kurosumi14,19 , Takashi Sakatani20 ,
Shigeki Shimizu21 , Kohei Taniguchi22 , Sadafumi Tamiya23 ,
Harumi Nakamura24 , Chizuko Kanbayashi25 , Tadahiko Shien 26 and
Hiroji Iwata27
1
Department of Basic Pathology, National Defense Medical College, Tokorozawa, Saitama, Japan, 2 Department of
Diagnostic Pathology, National Cancer Center Hospital, Chuo-ku, Tokyo, Japan, 3 Department of Pathology, The
Cancer Institute of Japan Foundation for Cancer Research, Koto-ku, Tokyo, Japan, 4 Department of Diagnostic
Pathology, Social Medical Corporation Hakuaikai Sagara Hospital, Kagoshima-city, Kagoshima, Japan, 5 Department
of Pathology, Toranomon Hospital, Minato-ku, Tokyo, Japan, 6 Department of Pathology, Tokai University School of
Medicine, Isehara, Kanagawa, Japan, 7 Department of Clinical Laboratories, National Hospital Organization
Kasumigaura Medical Center, Tsuchiura, Ibaraki, Japan, 8 Department of Diagnostic Pathology, National Hospital
Organization Kure Medical Center and Chugoku Cancer Center, Kure, HIroshima, Japan, 9 Department of Pathology
and Molecular Diagnostics, Aichi Cancer Center Hospital, Nagoya, Aichi, Japan, 10 Department of Pathology,
National Hospital Organization Nagoya Medical Center, Nagoya, Aichi, Japan, 11 Clinical Oncology and Pathology
Division, National Cancer Center Exploratory Oncology Research and Clinical Trial Center, Kashiwa, Chiba, Japan,
12
Department of Molecular Pathology, Yokohama City University School of Medicine, Yokohama, Kanagawa, Japan,
13
Department of Diagnostic Pathology, Niigata Cancer Center Hospital, Niigata-city, Niigata, Japan, 14 Department of
Pathology, Saitama Cancer Center, Ina, Saitama, Japan, 15 Department of Diagnostic Pathology, National Hospital
Organization Tokyo Medical Center, Meguro-ku, Tokyo, Japan, 16 Department of Diagnostic Pathology, Chiba Cancer
Center, Chiba-city, Chiba, Japan, 17 Department of Pathology, Kitasato University School of Medicine, Sagamihara,
Kanagawa, Japan, 18 Department of Experimental Pathology and Tumor Biology, Nagoya City University Graduate
School of Medical Sciences, Nagoya, Aichi, Japan, 19 Pathology Division, Breast Center, Kameda Medical Center,
Chuo-ku, Tokyo, Japan, 20 Department of Diagnostic Pathology, Nippon Medical School Hospital, Bunkyo-ku, Tokyo,
Japan, 21 Department of Pathology, Kindai University Faculty of Medicine, Osaka-sayama, Osaka, Japan,
22
Department of Pathology, Okayama University, Okayama-city, Okayama, Japan, 23 Department of Diagnostic
Pathology, Kitakyushu Municipal Medical Center, Kitakyushu, Fukuoka, Japan, 24 Department of Pathology and
Cytopathology, Osaka International Cancer Institute, Osaka-city, Osaka, 25 Department of Breast Oncology, Niigata
Cancer Center Hospital, Niigata-city, Niigata, Japan, 26 Department of Breast and Endocrine Surgery, Okayama
University Hospital, Okayama-city, Okayama, Japan and 27 Department of Breast Oncology, Aichi Cancer Center
Hospital, Nagoya, Aichi, Japan
*For reprints and all correspondence: Hitoshi Tsuda, Department of Basic Pathology, National Defense Medical College,
3-2 Namiki, Tokorozawa, Saitama 359-8513, Japan. E-mail: htsuda@ndmc.ac.jp
© The Author(s) 2021. Published by Oxford University Press. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com 434
Jpn J Clin Oncol, 2021, Vol. 51, No. 3 435
Received 11 August 2020; Editorial Decision 10 November 2020; Accepted 13 November 2020
Abstract
Objective: The Japan Clinical Oncology Group 1505 trial is a single-arm multicentre prospective
study that examined the possibility of non-surgical follow-up with endocrine therapy for patients
with low-grade ductal carcinoma in situ. In that study, the eligible criteria included histopathological
findings comprising low to intermediate nuclear grade and absence of comedo necrosis, and cases
were entered according to the local histopathological diagnosis. Nuclear grade is largely based
on the Consensus Conference criteria (1997), whereas comedo necrosis is judged according to the
Rosen’s criteria (2017). The purpose of this study was to standardize and examine the interobserver
agreement levels of these histopathological criteria amongst the participating pathologists.
Methods: We held slide conferences, where photomicrographs of haematoxylin–eosin-stained
Downloaded from https://academic.oup.com/jjco/article/51/3/434/6070012 by guest on 19 November 2021
slides from 68 patients with ductal carcinoma in situ were presented using PowerPoint. The nuclear
grade and comedo necrosis statuses individually judged by the pathologists were analysed using
κ statistics.
Results: In the first and second sessions, where 22 cases each were presented, the interobserver
agreement levels of nuclear grade whether low/intermediate grade or high grade were moderate
amongst 29 and 24 participating pathologists, respectively (κ = 0.595 and 0.519, respectively). In the
third session where 24 cases were presented, interobserver agreement levels of comedo necrosis
or non-comedo necrosis were substantial amongst 25 participating pathologists (κ = 0.753).
Conclusion: Although the concordance rates in nuclear grade or comedo necrosis were not high in
a few of the cases, we believe that these results could provide a rationale for employing the present
criteria of nuclear grade and comedo necrosis in the clinical study of ductal carcinoma in situ.
Key words: ductal carcinoma in situ, nuclear grade, comedo necrosis, interobserver agreement
Introduction radiotherapy. In other retrospective studies, high NG, larger tumour
The incidence of breast cancer is extremely high in Europe and size, younger patient’s age, CN and their various combinations were
the USA and is increasing in Asian countries. The rate of ductal also shown to be indicators of higher local recurrence rate (17–19).
carcinoma in situ (DCIS) is also increasing worldwide in association In studies conducted in Japan, however, there are insufficient data
with the spread of breast cancer screening (1–3). In Japan, in 2016, suggesting that these histopathological parameters are indicators of
95 257 novel female patients had breast cancer, and 13.7% of them biological behaviour, postsurgical recurrence or response to radio-
had DCIS (4). therapy (20,21).
DCIS is a direct precursor of invasive carcinoma of the breast (5); In the management of lower-risk DCIS, follow-up may be allowed
as the standard treatment for patients with DCIS, mastectomy or par- without surgical therapy with or without hormonal therapy. Four
tial resection with radiation therapy is recommended (6,7). However, clinical trials examining the validity of non-resection for low-risk
the biological behaviour of DCIS is highly heterogeneous from high- DCIS are ongoing (22–26). In Japan, a single-arm confirmatory trial
risk lesions with a tendency to progress to invasive carcinoma within of endocrine therapy alone for oestrogen receptor (ER)-positive, low-
5 years to lower-risk lesions that tend to remain DCIS over 10 years risk DCIS (JCOG1505, LORETTA trial) is now being undertaken
(8–10). If DCIS is subclassified into clinically low-risk and high-risk (UMIN ID 000028298) (27,28). The purpose of JCOG1505 is to
groups, treatment will be chosen according to the risk indicators, and confirm whether endocrine therapy alone for ER-positive, low-risk
observation could be performed if the tumour is certainly of low risk. DCIS is safe and effective compared with the current standard treat-
DCIS can be classified histologically by nuclear grade (NG) and ment. The primary outcome of the study was the 5-year cumulative
histological type. Consensus nuclear grading was first proposed in incidence of an invasive ipsilateral breast tumour.
1997 by the Consensus Conference Committee, where the cases of In the JCOG1505 trial, patients who had breast cancer that
DCIS were classified into Grade 1 (low), Grade 2 (intermediate) and fulfilled the following criteria were eligible for the study: (i) histo-
Grade 3 (high) (11). From histological type, DCIS can be classified logically proven DCIS; (ii) low or intermediate NG (NG1 or NG2);
into the comedo type and the non-comedo type including cribriform, (iii) absence of CN; (iv) high positive ER (29) and (v) negative
papillary, papillary–cribriform, solid, micropapillary, flat (clinging), HER2 (30). For (i), (iv) and (v), the diagnostic criteria have been
solid–papillary (endocrine) ones and so on (12,13). Many studies established. However, for (ii) NG and (iii) CN, no universal criteria
have been conducted to identify risk factors for DCIS. Silverstein or consensus have been established by pathologists. Therefore, in
and colleagues proposed the van Nuys risk index including NG and JCOG1505, the criteria for registering NG and CN were set and
comedo necrosis (CN), in which the high-risk DCIS group frequently informed to the pathologists who worked with collaborating hos-
showed local recurrence after partial resection (14–16). They found pitals. Slide conferences were then conducted by the pathologists
that risk estimation of local recurrence was possible by the combi- using photomicrographs of DCIS for standardization and revision
nation of age, tumour extension, NG, necrosis, distance margins and of the criteria, and a feedback was provided to them. In parallel, we436 Grade of ductal carcinoma in situ
Table 1. Nuclear grading employed in the present study
A. Nuclear grade (NG) (11)
Appearance:
Point 1: Monotonous (monomorphic)
Point 2: Between 1 and 3 points
Point 3: Markedly pleomorphic
Size:
Point 1: 1.5–2.0 normal red blood cell (RBC) or duct epithelial cell nucleus dimensions
Point 2: Between 1 and 3 points
Point 3: Nuclei usually >2.5 RBCs or duct epithelial cell nuclear dimensions
Features:
Point 1: Usually exhibit diffuse, finely dispersed chromatin, only occasional nucleoli and mitotic figures. Usually associated with the
polarization of constituent cells
Point 2: Between 1 and 3 points
Downloaded from https://academic.oup.com/jjco/article/51/3/434/6070012 by guest on 19 November 2021
Point 3: Usually vesicular and exhibit irregular chromatin distribution and prominent and often multiple nucleoli. Mitoses may be conspicuous
Caveat: The presence of nuclei of similar size but pleomorphic precludes a low-grade classification
Caveat: NG is to be given from the part with the highest atypia
∗Sum of the three elements
3–5 points: NG1
6–7 points: NG2
8–9 points: NG3
∗In the original Consensus Conference, only the upper three elements, namely, appearance, size and features, are described. In the sum-of-point
method, grade was evaluated based on the sum of the points of the three elements
B. Comedo necrosis (CN) (33)
Definition: Solid intraepithelial growth within the basement membrane with central (zonal) necrosis
The necrosis seen in the intraductal spread of carcinoma with a cribriform or micropapillary pattern is not included in the CN
evaluated the interobserver agreement in NG and CN amongst the from NCN. From an interim survey that was performed to clarify
pathologists at the slide conferences. the reasons why individual case entries failed in the JCOG1505 trial,
one of the major reasons was the presence of CN in the pathology
reports. The case entry was often discontinued because the pathology
Methods
report described only necrosis and CN or NCN remained unknown.
Criteria for NG and CN Based on the survey results, the criteria for CN were replaced with
The DCIS of NG3 was not eligible for the JCOG1505 trial. In the the Rosen’s criteria: ‘solid intraepithelial growth within the basement
study, the criteria used for determining NG were a modified version membrane with central (zonal) necrosis’ (33). Rosen also described
of Consensus Conference criteria on the Classification of Ductal that the necrosis observed in patients who presented with intraductal
Carcinoma In Situ (The Consensus Conference Committee 1997) spread of carcinoma with a cribriform or micropapillary pattern is
(11). In the Consensus Conference, NG was decided after a compre- not included in the CN criteria. According to these changes, the
hensive evaluation of three elements: appearance, size and features. In judgement of necrosis in DCIS appeared to be much clearer, and
histological grading (5,31) or nuclear grading (32) of invasive ductal the frequency of NCN was expected to increase. The method for
carcinoma, the sum of points of each element appears objective and the evaluation of necrosis employed in the JCOG 1505 study is also
was expected to provide stable interobserver reproducibility com- shown in Table 1.
pared with a comprehensive evaluation. Therefore, we introduced
the sum-of-point method of the Consensus Conference criteria. Interobserver reproducibility
In this method, three elements, namely, appearance, size and This work was approved by the Ethical Committee of the National
features, were separately evaluated, and a rating of 1–3 points was Defense Medical College.
provided as shown in Table 1. The scores of all three elements were From a total of 68 cases of DCIS, photomicrographic images of
summed. NG1 was given when the total score was 3–5 points, NG2 haematoxylin–eosin-stained slides were acquired with ×10, ×20 and
when the total score was 6–7 points and NG3 when the total score ×40 objective lens using the Olympus BX41 light microscope and the
was 8–9 points. Leica DFC CCD camera system (Tokyo, Japan).
Patients with DCIS with CN were not eligible in the JCOG1505 Slide conferences were held three times, and five sets of study data
trial. Initially, after the Consensus Conference Committee meeting were acquired: for interobserver agreement study of NG, two studies
(11), the JCOG1505 trial defined CN as the presence of any central were conducted in the first conference, and another study was con-
zone necrosis within a duct, usually exhibiting a linear pattern within ducted in the second conference. For interobserver agreement study
ducts if sectioned longitudinally. The presence of ghost cells and of CN, two other studies were conducted in the third conference.
karyorrhectic debris was important for distinguishing necrotic debris At each conference, the criteria and methods of NG and CN
from secretory material. By contrast, punctate necrosis, or non-zonal were at first explained with several representative images. Then,
type necrosis, was defined as non-CN (NCN). photomicrographic images of DCIS cases, taken using one ×10, one
However, no further details were described in the Consensus ×40 and one ×100 objective lens, were provided using a PowerPoint
Conference criteria; hence, it is often difficult to differentiate CN presentation.Jpn J Clin Oncol, 2021, Vol. 51, No. 3 437
Table 2. Results of the first conference where 29 observers provide the NG to 22 ductal carcinoma in situ (DCIS) cases according to the
comprehensive method and the sum-of-point method
Case NG by comprehensive method NG by sum-of-point method
NG1 vs, NG2 vs. NG3 Eligible vs. non-eligible NG1 vs. NG2 vs. NG3 Eligible vs. non-eligible
Modal grade No. of modal Major No. of major Modal No. of modal Major No. of major
grade (%) eligibility eligibility (%) grade grade (%) eligibility eligibility (%)
1 1 14/25 (56) Eligible 25/25 (100) 1 20/28 (71) Eligible 28/28 (100)
2 1 25/26 (96) Eligible 26/26 (100) 1 29/29 (100) Eligible 29/29 (100)
3 1 24/26 (92) Eligible 26/26 (100) 1 29/29 (100) Eligible 29/29 (100)
4 2 11/18 (61) Eligible 17/18 (94) 1 21/22 (95) Eligible 21/22 (95)
5 2 14/26 (54) Eligible 26/26 (100) 1 22/29 (76) Eligible 29/29 (100)
6 1 15/26 (58) Eligible 26/26 (100) 1 26/29 (90) Eligible 29/29 (100)
Downloaded from https://academic.oup.com/jjco/article/51/3/434/6070012 by guest on 19 November 2021
7 2 17/26 (65) Eligible 26/26 (100) 1 15/29 (52) Eligible 29/29 (100)
8 1/2 13/26 (50) Eligible 26/26 (100) 1 17/29 (59) Eligible 29/29 (100)
9 2 22/26 (85) Eligible 22/26 (85) 2 17/29 (59) Eligible 28/29 (97)
10 2 20/25 (80) Eligible 21/25 (84) 2 23/29 (79) Eligible 26/29 (90)
11 2 23/26 (88) Eligible 24/26 (92) 2 24/29 (83) Eligible 28/29 (97)
12 2 25/26 (96) Eligible 26/26 (100) 2 23/29 (79) Eligible 28/29 (97)
13 2 21/26 (81) Eligible 25/26 (96) 2 17/29 (59) Eligible 28/29 (97)
14 2 22/26 (85) Eligible 23/26 (88) 2 19/29 (66) Eligible 23/29 (79)
15 2 20/26 (77) Eligible 23/26 (88) 2 19/29 (66) Eligible 29/29 (100)
16 3 18/26 (69) Non- 18/26 (69) 3 19/29 (66) Non- 19/29 (66)
eligible eligible
17 3 22/26 (85) Non- 22/26 (85) 3 23/29 (79) Non- 23/29 (79)
eligible eligible
18 3 26/26 (100) Non- 26/26 (100) 3 25/29 (86) Non- 25/29 (86)
eligible eligible
19 2 16/26 (62) Eligible 16/26 (62) 2 17/29 (59) Eligible 19/29 (66)
20 3 26/26 (100) Non- 26/26 (100) 3 29/29 (100) Non- 29/29 (100)
eligible eligible
21 3 26/26 (100) Non- 26/26 (100) 3 29/29 (100) Non- 29/29 (100)
eligible eligible
22 3 14/26 (54) Non- 14/26 (54) 2/3 14/29 (48) Equivocal 14/29 (48)
eligible
NG judgements provided by >66% of the observers are underlined.
In the first conference, the two nuclear grading methods were two observers (34). According to Landis and Koch, the κ values
compared, that is, comprehensive evaluation and sum-of-point were divided into several scales to evaluate the strength of agree-
method based on the Consensus Conference criteria. At first, 29 ment (36): poor (κ < 0.00), slight (0.00–0.20), fair (0.21–0.40),
participants were requested to provide a comprehensive evaluation moderate (0.41–0.60), substantial (0.61–0.80) or almost perfect
of NG in 22 DCIS cases. Thereafter, they were requested to provide (0.81–1.00) (36).
the NG based on the sum of the points of the same 22 cases.
In the second conference, 140 days after the first meeting, the NG
of the 22 DCIS cases was re-evaluated using the sum-of-point method
by 24 pathologists. These 22 cases were identical to those examined Results
in the first conference, but the photomicrographs were presented Results of the first conference
from different microscopic fields, and the order of presentation was
Based on the comprehensive evaluation method, the κ value was
shuffled.
0.474 when the grades were trichotomized into NG1, NG2 and NG3.
In the third conference, with 25 participant pathologists, the
The κ value was 0.592 (moderate agreement) when the grades were
type of necrosis of 24 DCIS cases was initially classified into CN
dichotomized into eligible (NG1 or NG2) and non-eligible (NG3).
or NCN according to the Consensus Conference criteria and then
Based on the sum-of-point method, the κ value was 0.251 with
was re-classified according to Rosen’s criteria. Ten of these pho-
fair agreement when the given points were divided into seven levels
tomicrographs were obtained from the pathology data stored using
from 3 to 9. The κ values were 0.461 (moderate agreement) when
a Hamamatsu NDP slide scanner (Hamamatsu Photonics, Hama-
the sum of the points was trichotomized into NG1, NG2 and NG3
matsu, Japan).
and 0.596 (moderate agreement) when the points were dichotomized
into eligible (NG1 or NG2) and non-eligible (NG3). Unexpectedly,
Statistical analysis there was no large difference between the sum-of-point method
For each conference, the level of interobserver agreement on NG and the comprehensive evaluation method in terms of interobserver
and necrosis was tested using the generalized κ test for more than reproducibility.438 Grade of ductal carcinoma in situ
Table 3. Results of the second conference where 24 observers provided NG to 22 DCIS cases according to the sum-of-point method of the
Consensus Conference criteria
Case NG by sum-of-point method (1 vs. 2 vs. 3) NG by sum-of-point method (eligible vs. non-eligible)
Modal grade No. of modal grade (%) Major eligibility No. of major eligibility (%)
1 2 16 (67) Eligible 24 (100)
2 3 15 (63) Non-eligible 15 (63)
3 1 21 (88) Eligible 24 (100)
4 3 17 (71) Non-eligible 17 (71)
5 2 14 (58) Eligible 23 (96)
6 2 15 (63) Eligible 20 (83)
7 1 21 (88) Eligible 24 (100)
8 1 13 (54) Eligible 24 (100)
9 3 22 (92) Non-eligible 22 (92)
Downloaded from https://academic.oup.com/jjco/article/51/3/434/6070012 by guest on 19 November 2021
10 2 18 (75) Eligible 23 (96)
11 1 19 (79) Eligible 24 (100)
12 2 14 (58) Eligible 24 (100)
13 1 18 (75) Eligible 24 (100)
14 2 20 (83) Eligible 20 (83)
15 1 22 (92) Eligible 24 (100)
16 3 13 (54) Non-eligible 13 (54)
17 2/3 12 (50) Equivocal 12 (50)
18 2 15 (63) Eligible 24 (100)
19 3 23 (96) Non-eligible 23 (96)
20 1 20 (83) Eligible 23 (96)
21 2 15 (63) Eligible 15 (63)
22 2 18 (75) Eligible 22 (92)
NG judgements provided by >66% of the observers are underlined.
The results of the first conference are shown in Table 2 and the points were dichotomized into eligible (NG1 or NG2) and non-
Supplementary Figure S1. Of the 22 cases, the modal NGs amongst eligible (NG3).
29 observers were NG1 in 4, NG2 in 11, NG3 in 6 and equivocal Of these 22 cases, the modal NGs amongst 24 observers were
between NG1 and NG2 in 1 as determined using the comprehensive NG1 in 7, NG2 in 9, NG3 in 5 and equivocal between NG2 and
evaluation method. In 14 of these 22 DCIS cases (64%), >66% of the NG3 in 1. In 13 DCIS cases (59%), >66% of the observers provided
observers provided a modal NG (Cases 2, 3, 9–18, 20 and 21). When the modal NG (Cases 1, 3, 4, 7, 9–11, 13–15, 19, 20 and 22).
classified as either eligible (NG1 or NG2) or non-eligible (NG3), 16 When they were classified as eligible (NG1 or NG2) and non-eligible
were judged as eligible and 6 as non-eligible as the major judgement. (NG3), 16 were judged as eligible and 5 as non-eligible as the major
In 20 DCIS cases (91%), except for Cases 19 and 22, >66% of the judgement and 1 as equivocal between eligible and non-eligible. In 18
observers provided the major judgement. DCIS cases (82%), except for Cases 2, 16, 17 and 21, >66% of the
Of these 22 cases, the modal NGs amongst 29 observers were observers provided modal judgement. Representative cases to which
NG1 in 8, NG2 in 8, NG3 in 5 and equivocal between NG2 and NG3 a majority (>66%) of observers provided NG1, NG2 and NG3 and
in 1 as determined using the sum-of-point method. In 13 DCIS cases other representative cases for which NGs were separated are shown
(59%), >66% of the observers provided a modal grade (Cases 1–6, in Figure 1A–H.
10–12, 17, 18, 20 and 21). When they were classified as eligible (NG1
or NG2) or non-eligible (NG3), 17 were judged as eligible and 5 as
non-eligible as the major judgement. In 19 of the DCIS cases (86%), Results of the third conference
except for Cases 16, 19 and 21, >66% of the observers provided the The results of the third conference are presented in Table 4 and
major judgement. Supplementary Figure S3. In the judgements of whether CN or NCN,
based on the Consensus Conference criteria, the κ value was 0.721
(substantial agreement). In cases with central necrosis and karyor-
rhectic debris with background solid and/or cribriform structures,
Results of the second conference a high interobserver agreement was achieved. In cases with necrosis
The results of the second conference are presented in Table 3 and and background micropapillary and/or a flat structure, the observers’
Supplementary Figure S2. Because the sum-of-point method was judgements were divided between CN and NCN. In the cases with
decided to be used for nuclear grading in the JCOG1505 study, secreted material, histiocyte accumulation and punctate necrosis, a
a repeat interobserver agreement study was performed using this high interobserver agreement was achieved.
method. The κ value was 0.180, with slight agreement when the given Of the 24 cases, based on the Consensus Conference criteria, the
points were divided into seven levels from 3 to 9. The κ values were major judgement amongst 25 observers was CN in 10 and NCN in
0.406 (moderate agreement) when the points were trichotomized 14. In 22 DCIS cases (92%), except for Cases 9 and 17, >66% of the
into NG1, NG2 and NG3 and 0.519 (moderate agreement) when observers provided major judgement.Jpn J Clin Oncol, 2021, Vol. 51, No. 3 439
Downloaded from https://academic.oup.com/jjco/article/51/3/434/6070012 by guest on 19 November 2021
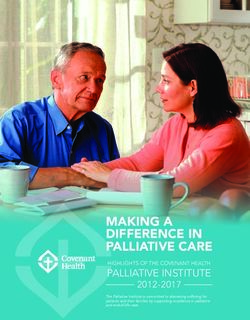
Figure 1. Representative ductal carcinoma in situ (DCIS) cases of nuclear grade (NG) 1, 2 and 3 and equivocal cases according to the sum-of-point method in the
second conference. In A–F, a majority (>66%) of observers provided the same NG: (A) NG1 (Case 7); (B) NG1 (Case 15); (C) NG2 (Case 10); (D) NG2 (Case 14); (E)
NG3 (Case 4); (F) NG3 (Case 9). In G and H, judgements of NG separated between NG2 and NG3: (G) Case 16; (H) Case 17. Objective lens ×100.
Table 4. Results of the third conference where 25 observers judged the necrosis in 24 DCIS cases according to the Consensus Conference
criteria and Rosen’s criteria
Case Necrosis judgement by Consensus Conference criteria Necrosis judgement by Rosen’s criteria
Comedo (%) Non-comedo (%) Comedo (%) Non-comedo (%)
1 22 (88) 3 (12) 23 (92) 2 (8)
2 4 (16) 21 (84) 0 (0) 25 (100)
3 25 (100) 0 (0) 24 (96) 1 (4)
4 4 (16) 21 (84) 5 (20) 20 (80)
5 0 (0) 25 (100) 0 (0) 25 (100)
6 24 (96) 1 (4) 23 (92) 2 (8)
7 0 (0) 25 (100) 0 (0) 25 (100)
8 25 (100) 0 (0) 3 (12) 22 (88)
9 13 (52) 12 (48) 0 (0) 25 (100)
10 0 (0) 25 (100) 0 (0) 25 (100)
11 0 (0) 25 (100) 0 (0) 25 (100)
12 20 (80) 5 (20) 3 (12) 22 (88)
13 20 (80) 5 (20) 6 (24) 19 (76)
14 0 (0) 25 (100) 0 (0) 25 (100)
15 3 (12) 22 (88) 0 (0) 25 (100)
16 1 (4) 24 (96) 0 (0) 25 (100)
17 14 (56) 11 (44) 0 (0) 25 (100)
18 0 (0) 25 (100) 1 (4) 24 (96)
19 24 (96) 1 (4) 25 (100) 0 (0)
20 0 (0) 25 (100) 0 (0) 25 (100)
21 2 (8) 23 (92) 0 (0) 25 (100)
22 20 (80) 5 (20) 5 (20) 20 (80)
23 2 (8) 23 (92) 2 (8) 23 (92)
24 0 (0) 25 (100) 0 (0) 25 (100)
The necrosis judgements provided by >66% of the observers are underlined.440 Grade of ductal carcinoma in situ
Downloaded from https://academic.oup.com/jjco/article/51/3/434/6070012 by guest on 19 November 2021
Figure 2. Representative DCIS cases with comedo necrosis and with discrepancy in comedo necrosis judgements in the third conference. (A–D) Comedo necrosis
without discrepancy: (A–B) Case 3. (C–D) Case 19. By both the Consensus Conference criteria and Rosen’s criteria, the major judgement of comedo necrosis did
not differ. (E–H) Comedo necrosis with discrepancy. (E) Case 12; (F) Case 8; (G) Case 17 and (H) Case 22. According to the Consensus Conference criteria, the
major judgement was comedo necrosis; however, based on the Rosen’s criteria, the major judgement changed to non-comedo necrosis. Objective lens ×10 in
E, ×20 in F–H.
In the judgement of whether CN or NCN, based on Rosen’s information to the participating pathologists and for conducting
criteria, the κ value was 0.753 (substantial agreement). In the cases interobserver agreement studies. The study results of the conferences
with central necrosis and a background solid structure (Fig. 2A–D) were sent to the physicians and pathologists from collaborating
and those with secreted material, histiocyte accumulation and hospitals for feedback (Supplementary material). Accurate under-
punctate necrosis, a high interobserver agreement was observed. standing of the histopathological criteria of NG and CN will help
In cases with necrosis with background cribriform, micropapillary enhance case entry to JCOG1505. In June 2020, >70 cases were
and/or flat structure, a high interobserver agreement was acquired, recruited for the ongoing trial.
although the major judgement was changed from CN to NCN In the first study, nuclear grading of DCIS using both the com-
(Fig. 2E–H). prehensive method and the sum-of-point method revealed a similar
Based on Rosen’s criteria, the major judgement as to whether CN interobserver agreement level with an acceptable (moderate) level.
or NCN amongst the 25 observers was CN in 4 and NCN in 20. In Although the number of cases with modal NG1 doubled by the sum-
all 24 DCIS cases (100%), >66% of the observers provided major of-point method (n = 8, 36%) in comparison with that by the com-
judgement. prehensive method (n = 4, 18%), the percentage of eligible cases eval-
uated by these two methods was the same (73%, each) (Table 5). In
Discussion addition, agreement levels calculated by κ statistics (0.592 and 0.596)
Low-to-intermediate NG and NCN are necessary conditions for did not differ between these two methods. Furthermore, between the
entry in the JCOG1505 trial (27,28). To date, the classifications first and the second conferences that aimed at comparing the rates
of NG and CN established by the Consensus Conference appear of eligible cases and interobserver agreement levels using the sum-of-
to be the most standard and internationally influential. However, point method, these rates and levels were very similar between the
these classifications are not well known, and they are not clinically two conferences: the rates being 73% each and the κ values being
applied by diagnostic pathologists. Therefore, in the beginning of 0.596 and 0.519, respectively (Table 5). Therefore, the sum-of-point
protocol preparation and the revision of the study protocol, it was method employed in this study appeared to be reasonable in terms
necessary to establish and modify the criteria and inform these to the of the percentage of eligible cases and interobserver agreement level.
pathologists from different participating hospitals. At present, the By conducting repeat slide conferences, the interobserver
Consensus Conference criteria (11) with modification by the sum- reproducibility of nuclear grading of DCIS could be improved. In
of-point method were employed for nuclear grading, and Rosen’s particular, the feedback of the slides used and the results of the
criteria (33) were employed for the evaluation of CN. conference to the participants and periodic repetition of the
Slide conferences using photomicrographs of DCIS were conference would be effective. However, in interobserver variability
conducted three times to standardize the criteria and provide this studies published by other study groups, the agreement levels wereJpn J Clin Oncol, 2021, Vol. 51, No. 3 441
Table 5. Summary of the results of the present study
A. NG
Number of cases (%)
First conference First conference Second conference
(comprehensive) (sum of points) (sum of points)
Modal NG
NG1 4 (18) 8 (36) 7 (32)
NG2 11 (50) 8 (36) 9 (40)
NG3 6 (27) 5 (23) 5 (23)
Equivocal NG1 vs. NG2 1 (5) 0 (0) 0 (0)
Equivocal NG2 vs. NG3 0 (0) 1 (5) 1 (5)
Downloaded from https://academic.oup.com/jjco/article/51/3/434/6070012 by guest on 19 November 2021
Major eligibility status
Eligible (NG1 or NG2) 16 (73) 16 (73) 16 (73)
Non-eligible (NG3) 6 (27) 6 (27) 6 (27)
Cases to which >66% observers provided modal NG 14 (64) 13 (59) 13 (59)
Cases to which >66% observers provided major status 20 (91) 19 (86) 18 (82)
κ value (NG1 vs. NG2 vs. NG3) 0.474 0.461 0.406
κ value (eligible vs. non-eligible) 0.592 0.596 0.519
B. Necrosis
Number of cases (%)
Third conference Third conference
(Consensus Conference) (Rosen’s criteria)
Major necrosis status
Non-comedo necrosis 14 (59) 19 (79)
Comedo necrosis (CN) 10 (41) 5 (21)
Equivocal CN vs. NCN 0 (0) 0 (0)
Cases to which >66% observers provided major eligibility status 22 (92) 24 (100)
κ value (CN vs. NCN) 0.721 0.753
reported as moderate or substantial (36–38). In fact, the interobserver decreased to 21% (n = 5) according to the Rosen’s criteria. From
agreement level in the second conference (κ = 0.519) did not these successful revisions of CN criteria, it was expected to be able
increase compared to that in the first conference (κ = 0.596). The to expand the indication of accrual to the JCOG1505 trial without
reason for no obvious improvement was considered to be partly affecting the interobserver agreement level.
due to the facts that a majority of the participant pathologists were Is it appropriate to introduce the Rosen’s criteria that may
working for large-volume cancer centres and already familiar with change the diagnosis from comedo DCIS to non-comedo DCIS in
the diagnosis of DCIS and that more than half of these participants nearly 20% of the cases? The biological properties of recruited
differed between the first and second conferences. Only 14 observers cases of DCIS were evaluated not only by CN but also by NG,
participated in both the first and second conferences. Amongst these tumour size, ER, HER2, imaging diagnosis and so on. Non-eligibility
14 observers, kappa values in the first and second conferences were in these factors would help exclude high-risk cases from Rosen’s
0.667 and 0.519 (data not shown). Therefore, the proper difficulty NCN cases. Other than Rosen’s criteria, a detailed description
in the nuclear grading of DCIS is another cause of suboptimal of CN was not found in the literature; in terms of interobserver
agreement. Even in the histological grading of invasive carcinoma, reproducibility, both the Consensus Conference criteria and Rosen’s
tubular formation and the count of mitotic figures were considered criteria revealed equally substantial agreement levels. For these
semiquantitative or quantitative, but the evaluation of nuclear atypia reasons, we considered that the introduction of Rosen’s criteria to the
is difficult because of its qualitative nature (5,31,32). Amongst the JCOG1505 trial was reasonable, although whether the introduction
NG elements evaluated in this study, ‘appearance’ and ‘features’ are of these criteria was the best choice or not should be verified in the
essentially qualitative, although the size appeared only much more future.
quantitative. Such properties of DCIS nuclear grading might also In routine diagnosis, most pathologists do not evaluate CN based
have affected the interobserver agreement levels. on the Rosen’s criteria; hence, some pathologists may be concerned
Interobserver agreement levels in the judgements of CN were about consistency in diagnosing CN between routine practice and
substantial irrespective of the usage of the Consensus Conference this clinical trial. To address this problem, when the entry was taken
criteria or the usage of Rosen’s criteria (κ = 0.721 and 0.753, into consideration by the physician, the physician was recommended
respectively). The major judgement was CN in 42% (n = 10) of to ask the pathologist to report the status of CN using both conven-
cases according to the Consensus Conference criteria, but the rate tional criteria and Rosen’s criteria.442 Grade of ductal carcinoma in situ
The differentiation of CN from punctate necrosis from the view- References
point of the size or the area ratio of central necrosis remained 1. Ernster VL, Ballard-Barbash R, Barlow WE, et al. Detection of ductal
undetermined. In addition, on judging necrosis according to Rosen’s carcinoma in situ in women undergoing screening mammography. J Natl
criteria, whether the structural pattern of DCIS is solid or cribriform Cancer Inst 2002;94:1546–54.
is sometimes difficult to determine. In cases of an almost solid pattern 2. Duffy SW, Dibden A, Michalopoulos D, et al. Screen detection of
but only small or partial small secondary tubules are visible, the ductal carcinoma in situ and subsequent incidence of invasive interval
method of judgement is still unclear. breast cancers: a retrospective population-based study. Lancet Oncol
In the LORIS trials, the central pathology review system was 2016;17:109–14.
3. Román M, Rué M, Sala M, et al. Trends in detection of invasive cancer and
employed for case entry (23–25). In the COMET trial, review and
ductal carcinoma in situ at biennial screening mammography in Spain: a
agreement of histology slides between the two clinical pathologists
retrospective cohort study. PLoS One 2013;8:e83121 eCollection 2013.
were the eligibility criteria (26). In cases of disagreement between 4. Japanese Breast Cancer Society. Aggregated data of National Clinical
the two pathology reviews about whether or not a case fulfils the Database Breast Cancer Registry in 2016. 2019. http://jbcs.gr.jp/ (accessed
eligibility criteria, a third pathology review will be required. In the May 10, 2020).
present trial, a local diagnosis system was employed. To maintain 5. Pinder SE, Collins LC, Fox SB, et al. Ductal carcinoma in situ. In: WHO
Downloaded from https://academic.oup.com/jjco/article/51/3/434/6070012 by guest on 19 November 2021
and improve the quality and interobserver agreement as high as the Classification of Tumours Editorial Board, editor. Breast Tumours. WHO
central pathology review system, it would be helpful to introduce Classification of Tumours, 5th edn. Lyon: World Health Organization,
digital pathology tools, for example, pathology atlas containing 2019; 76–81.
representative and equivocal cases with detailed explanation. 6. Gradishar WJ, Anderson BO, Balassanian R, et al. Breast cancer, version
4.2017, NCCN clinical practice guidelines in oncology. J Natl Compr
The limitations of the present study include the formation of a
Canc Netw 2018;16:310–20.
slide conference and the small number of cases. Because of the slide
7. Inokuchi M, Kutomi G, Kijima Y, et al. The Japanese Breast Cancer Society
conference style, the pathologists were not able to correctly evaluate clinical practice guidelines for surgical treatment of breast cancer, 2018
the NG and necrosis conditions from the entire tumour area for each edition. Breast Cancer 2020;27:4–8.
case. The number of cases for each study was only 22 to 24; hence, 8. Collins LC, Tamimi RM, Baer HJ, Connolly JL, Colditz GA, Schnitt
the selection bias might exist and might have influenced the study SJ. Outcome of patients with ductal carcinoma in situ untreated
results. Nonetheless, we believe that the present study could provide after diagnostic biopsy: results from the Nurses’ Health Study. Cancer
a rationale for employing the present criteria of NG and CN in DCIS. 2005;103:1778–84.
9. Sanders ME, Schuyler PA, Dupont WD, Page DL. The natural history
of low-grade ductal carcinoma in situ of the breast in women treated
Supplementary Material by biopsy only revealed over 30 years of long-term follow-up. Cancer
Supplementary material can be found at Japanese Journal of Clinical 2005;103:2481–4.
Oncology online. 10. Sanders ME, Schuyler PA, Simpson JF, Page DL, Dupont WD. Continued
observation of the natural history of low-grade ductal carcinoma in situ
reaffirms proclivity for local recurrence even after more than 30 years of
Acknowledgements follow-up. Mod Pathol 2015;28:662–9.
11. The Consensus Conference Committee. Consensus Conference on the
The authors thank to Drs. Akinobu Araki, Koji Arihiro, Misa Iijima, Tomo
classification of ductal carcinoma in situ. Cancer 1997;80:1798–802.
Osako, Masako Ohmori, Mayumi Kaneko, Kaori Kameyama, Kae Kawauchi,
12. Hoda SA. Ductal carcinoma in situ. In: Hoda SA, Brogi E, Koerner FC,
Junko Kuramoto, Kimiya Sato, Kaishi Satomi, Takashi Sugino, Masafumi
Rosen PP, editor. Rosen’s Breast Pathology, 4th edn. Philadelphia: Wolters
Takimoto, Kenichi Taguchi, Norihiro Teramoto, Shinichiro Horiguchi, Ichiro
Kluwer, 2014; 331–411.
Maeda, Kiyoshi Mori, Hiroyuki Yanai and Jiro Watanabe for the participa-
13. Lester SC, Bose S, Chen YY, et al. Protocol for the examination of
tion in the conference and collaboration to the acquisition of interobserver
specimens from patients with ductal carcinoma in situ of the breast. Arch
agreement data. Authors also thank to Ms. Chinami Onuma for technical
Pathol Lab Med 2009;133:15–25.
assistance.
14. Boland GP, Chan KC, Knox WF, Roberts SA, Bundred NJ. Value of the
van Nuys prognostic index in prediction of recurrence of ductal carcinoma
in situ after breast-conserving surgery. Br J Surg 2003;90:426–32.
Funding 15. Di Saverio S, Catena F, Santini D, et al. 259 patients with DCIS of the
breast applying USC/van Nuys prognostic index: a retrospective review
This work was supported in part by the National Cancer Cen- with long term follow up. Breast Cancer Res Treat 2008;109:405–16.
ter Research and Development Fund (26-A-4); Japan Agency for 16. Silverstein MJ, Lagios MD. Choosing treatment for patients with ductal
Medical Research and Development (AMED) Practical Research for carcinoma in situ: fine tuning the University of Southern California/van
Innovative Cancer Control (20ck0106429h0003). Nuys prognostic index. J Natl Cancer Inst Monogr 2010;2010:193–6.
17. Smith GL, Smith BD, Haffty BG. Rationalization and regionalization of
treatment for ductal carcinoma in situ of the breast. Int J Radiat Oncol
Conflict of interest statement Biol Phys 2006;65:1397–403.
Dr. Tsuda reports grants from Taiho and Goryo Chemical and per- 18. Sagara Y, Freedman RA, Vaz-Luis I, et al. Patient prognostic score and
sonal fees from Chugai outside the submitted work. Dr. Horii reports associations with survival improvement offered by radiotherapy after
breast-conserving surgery for ductal carcinoma in situ: a population-based
grants from Roche Diagnostics K.K. and personal fees from Chugai
longitudinal cohort study. J Clin Oncol 2016;34:1190–6.
and US-Lead outside the submitted work. Dr. Iwata reports grants
19. Solin LJ, Gray R, Hughes LL, et al. Surgical excision without radiation for
and personal fees from Novartis, AstraZeneca, Pfizer, Lilly, Daiichi- ductal carcinoma in situ of the breast: 12-year results from the ECOG-
Sankyo, MSD, Kyowa Hakko Kirin, and Chugai, and grants from ACRIN E5194 study. J Clin Oncol 2015;33:3938–44.
Bayer, Boehringer Ingelheim, Nihon Kayaku, and Sanofi, outside the 20. Sakai T, Iwase T, Teruya N, et al. Surgical excision without whole breast
submitted work. All remaining authors have declared no conflicts of irradiation for complete resection of ductal carcinoma in situ identified
interest. using strict, unified criteria. Am J Surg 2017;214:111–6.Jpn J Clin Oncol, 2021, Vol. 51, No. 3 443
21. Tamura N, Tsuda H, Yoshida M, et al. Clinicopathological predic- 29. Hammond ME, Hayes DF, Dowsett M, et al. American Society of Clinical
tive factors for ipsilateral and contralateral events following initial Oncology/College Of American Pathologists guideline recommendations
surgery to treat ductal carcinoma in situ. Breast Cancer 2016;23: for immunohistochemical testing of estrogen and progesterone receptors
510–8. in breast cancer. J Clin Oncol 2010;28:2784–95.
22. Elshof LE, Tryfonidis K, Slaets L, et al. Feasibility of a prospective, ran- 30. Wolff AC, Hammond ME, Hicks DG, et al. Recommendations for human
domized, open-label, international multicenter, phase III, non-inferiority epidermal growth factor receptor 2 testing in breast cancer: American
trial to assess the safety of active surveillance for low risk ductal carcinoma Society of Clinical Oncology/College of American Pathologists clinical
in situ – the LORD study. Eur J Cancer 2015;51:1497–510. practice guideline update. J Clin Oncol 2013;31:3997–4013.
23. Francis A, Thomas J, Fallowfield L, et al. Addressing overtreatment of 31. Elston EW, Ellis IO. Method for grading breast cancer. J Clin Pathol
screen detected DCIS: the LORIS trial. Eur J Cancer 2015;51:2296–303. 1993;46:189–90.
24. Pilewskie M, Stempel M, Rosenfeld H, Eaton A, Van Zee KJ, Morrow 32. Tsuda H, Akiyama F, Kurosumi M, Sakamoto G, Watanabe T. Establish-
M. Do LORIS trial eligibility criteria identify a ductal carcinoma in situ ment of histological criteria for high-risk node-negative breast carcinoma
patient population at low risk of upgrade to invasive carcinoma? Ann Surg in a randomized clinical trial of adjuvant therapy. Jpn J Clin Oncol
Oncol 2016;23:3487–93. 1998;28:486–91.
25. Pilewskie M, Olcese C, Patil S, Pilewskie M, Van Zee KJ. Women with 33. Hoda SA, Brogi E, Koerner FC, Rosen PP. Rosen’s Diagnosis of Breast
low-risk DCIS eligible for the LORIS trial after complete surgical exci- Pathology by Needle Core Biopsy, 4th edn. Philadelphia: Wolters Kluwer,
Downloaded from https://academic.oup.com/jjco/article/51/3/434/6070012 by guest on 19 November 2021
sion: how low is their risk after standard therapy? Ann Surg Oncol 2017; 148–73.
2016;23:4253–61. 34. Fleiss JL. Measuring nominal scale agreement among many raters. Psychol
26. Hwang ES, Hyslop T, Lynch T, et al. The COMET (comparison of Bull 1971;76:378–82.
operative versus monitoring and endocrine therapy) trial: a phase III 35. Landis JR, Koch GG. The measurement of observer agreement for cate-
randomised controlled clinical trial for low-risk ductal carcinoma in situ gorical data. Biometrics 1977;33:159–74.
(DCIS). BMJ Open 2019;9:e026797. 36. Van Bockstal M, Baldewijns M, Colpaert C, et al. Dichotomous
27. Kanbayashi C, Iwata H. Current approach and future perspective for histopathological assessment of ductal carcinoma in situ of the
ductal carcinoma in situ of the breast. Jpn J Clin Oncol 2017;47: breast results in substantial interobserver concordance. Histopathology
671–7. 2018;73:923–32.
28. UMIN-CTR Clinical Trial UMIN000028298. Single-arm confirmatory 37. Alghamdi SA, Krishnamurthy K, Garces Narvaez SA, et al. Low-grade
trial of endocrine therapy alone for estrogen receptor-positive, low- ductal carcinoma in situ. Am J Clin Pathol 2020;153:360–7.
risk ductal carcinoma in situ of the breast (JCOG1505, LORETTA 38. Dano H, Altinay S, Arnould L, et al. Interobserver variability in upfront
trial). https://upload.umin.ac.jp/cgi-open-bin/ctr_e/ctr_view.cgi?recptno= dichotomous histopathological assessment of ductal carcinoma in situ of
R000032260&language=E (accessed May 6, 2020). the breast: the DCISion study. Mod Pathol 2020;33:354–66.You can also read