POSSIBLE CROSS-REACTIVITY BETWEEN SARS-COV-2 PROTEINS, CRM197 AND PROTEINS IN PNEUMOCOCCAL VACCINES MAY PROTECT AGAINST SYMPTOMATIC SARS-COV-2 ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Article
Possible Cross-Reactivity between SARS-CoV-2
Proteins, CRM197 and Proteins in Pneumococcal
Vaccines May Protect Against Symptomatic
SARS-CoV-2 Disease and Death
Robert Root-Bernstein
Department of Physiology, Michigan State University, East Lansing, MI 48824, USA; rootbern@msu.edu
Received: 31 July 2020; Accepted: 16 September 2020; Published: 24 September 2020
Abstract: Various studies indicate that vaccination, especially with pneumococcal vaccines, protects
against symptomatic cases of SARS-CoV-2 infection and death. This paper explores the possibility that
pneumococcal vaccines in particular, but perhaps other vaccines as well, contain antigens that might be
cross-reactive with SARS-CoV-2 antigens. Comparison of the glycosylation structures of SARS-CoV-2
with the polysaccharide structures of pneumococcal vaccines yielded no obvious similarities.
However, while pneumococcal vaccines are primarily composed of capsular polysaccharides, some are
conjugated to cross-reacting material CRM197, a modified diphtheria toxin, and all contain about
three percent protein contaminants, including the pneumococcal surface proteins PsaA, PspA and
probably PspC. All of these proteins have very high degrees of similarity, using very stringent criteria,
with several SARS-CoV-2 proteins including the spike protein, membrane protein and replicase 1a.
CRM197 is also present in Haemophilus influenzae type b (Hib) and meningitis vaccines. Equivalent
similarities were found at lower rates, or were completely absent, among the proteins in diphtheria,
tetanus, pertussis, measles, mumps, rubella, and poliovirus vaccines. Notably, PspA and PspC are
highly antigenic and new pneumococcal vaccines based on them are currently in human clinical trials
so that their effectiveness against SARS-CoV-2 disease is easily testable.
Keywords: COVID-19; SARS-CoV-2; pneumococcal; Streptococcus pneumoniae; vaccine;
vaccination; cross-reactivity; similarity; protection; CRM197; PspA; PsaA; PspC; BCG; poliovirus;
measles–mumps–rubella; diphtheria–tetanus–pertussis; meningococcus
1. Introduction
Various studies have indicated that some vaccines may protect against symptomatic SARS-CoV-2
infection and death. A very significant inverse correlation has been found between rates of
pneumococcal vaccination at both the national and local population levels and rates of SARS-CoV-2
infections and death [1]. The study found no such correlations to the tuberculosis vaccine
BCG (Bacillus Calmette–Guerin), Haemophilus influenzae type B (Hib), diphtheria–tetanus–pertussis,
measles–mumps–rubella, or poliovirus vaccinations. The results were controlled for percent of the
population over 65 years of age, percent of obese individuals, percent of diabetics and the sum of these
factors. Pneumococcal vaccination with PCV13 was again found to be very significantly protective
in a study of 137,037 individuals for whom vaccination records were available [2] and other recent
vaccinations also provided apparent protection against SARS-CoV-2 after controlling for other variables.
The purpose of this paper is to provide a possible mechanism for how pneumococcal and other vaccines
might protect against SARS-CoV-2.
The specific hypothesis tested here is that antigens in pneumococcal vaccines induce antibodies
protective against SARS-CoV-2 by means of cross-reactivity with similar SARS-CoV-2 antigens.
Vaccines 2020, 8, 559; doi:10.3390/vaccines8040559 www.mdpi.com/journal/vaccinesVaccines 2020, 8, 559 2 of 20
I have treated all other vaccines as controls. There are two types of antigens that might play
such a role, one being the capsular polysaccharide antigens in current pneumococcal vaccines
and the other the proteins that they contain. An extensive search for polysaccharide structures
comparing SARS-CoV-2 glycosylated proteins [3] and S. pneumoniae serotypes [4] failed to identify
any obvious similarities. SARS-CoV-2 glycosylations are composed mainly of various arrangements
of N-acetylglucosamine, mannose, galactose and N-acetylneuraminic acid, with fucose appearing
in about half of the polysaccharides [3]. While N-acetylglucosamine and some mannose derivatives
appear in pneumococcal polysaccharides, N-acetylneuraminic acid does not appear in any, and only
pneumococcal serogroups 4, 5, 12 and 46 contain polysaccharides composed of both mannose and
fucose or N-acetylglucosamine and fucose [4]. These pneumococcal polysaccharides do not, however,
appear to share any obvious structural similarities with SARS-CoV-2 polysaccharides. While the
identity of polysaccharide structures is probably not required for antigenic cross-reactivity, with no
obvious structural homologies, the search then shifted to possible protein similarities.
While current pneumococcal vaccines are composed primarily of capsular polysaccharides,
they also contain one or both of two types of proteins. The polysaccharide component is never pure,
generally containing around three percent of the cell surface proteins to which the polysaccharides are
attached [5–7]. Proteins identified in pneumococcal vaccines include pneumococcal surface protein A
(PspA) and pneumococcal surface adhesin A (PsaA) [8,9]. Because the presence of PsaA was identified
only by immunological methods and PsaA cross-reacts strongly with an additional pneumococcal
surface protein, PspC (also known as CbpA and SpsA) [10,11], it is likely that PspC is also present in
capsular polysaccharide-based pneumococcal vaccines. Additionally, pneumococcal conjugate vaccines
covalently attach the polysaccharides to a modified diphtheria toxin protein called Cross-Reactive
Material 197 (CRM197), which is also present in Hib and meningitis vaccines [12].
This study investigates whether SARS-CoV-2 proteins contain regions that mimic sequences
within pneumococcal surface proteins and/or CRM197 (which is also found in Haemophilus influenzae
type B (Hib) vaccine and meningitis vaccine). Other vaccines such as measles, mumps, rubella, polio,
mycobacteria and pertussis are investigated as controls.
2. Materials and Methods
In order to ascertain whether PspA, PsaA, PspC and CRM197 have regions of significant similarity
to SARS-CoV-2 proteins, LALIGN (at www.expasy.org) was employed to perform pair-wise protein
comparisons. The parameters chosen were the 20 best alignments to show; BLOSUM80 (in order
to maximize small, local similarities); E = 10; the gap penalty of −10.0 (to maximize continuous
sequence similarities as are recognized by human leukocyte antigens and T cell receptors). SARS-CoV-2
sequences were retrieved from https://viralzone.expasy.org/8996 as HTML files or using the accession
numbers from the UniProtKB database (UniProtKB accession numbers P0DTC1–P0DTC9). Streptococcus
pneumoniae PspA, PsaA and PspC sequences were retrieved as accession numbers (provided in the
Tables below) from the UniProtKB database. Because different streptococcal serotypes have slightly
different versions of these proteins, several were randomly selected for each search and the sequences’
similarities displayed in Figure 1 are representative of several serotype results. The accession numbers
for the pneumococcal vaccines, CRM197 and the control vaccine proteins are listed in Table 1.Vaccines 2020, 8, 559 3 of 20
Table 1. UniProtKB accession numbers for viral and bacterial proteins used in this study.
UniProt
MICROBE List of Proteins
Identification
O34097
Q9LAZ1
pspA, Pneumococcal Surface Protein A
B2IRK1
Q9LAY4
P0A4G2
P0A4G3
STREPTOCOCCUS psaA, Pneumococcal surface protein, Manganese ABC transporter substrate protein
PNEUMONIAE P42363
Q04JB8
Q9KK40
Q9FDQ1
pspC, Pneumococcal Surface protein PspC
Q9KK37
Q9KK24
Q8DRK2 Pneumococcal Gram-positive anchor protein
P11235| HN_MUMPM (HN)RecName: Full = Hemagglutinin-neuraminidase
P30929 L_MUMPM (L)RecName: Full = RNA-directed RNA polymerase L
MUMPS P09458 FUS_MUMPR (F)RecName: Full = Fusion glycoprotein F0
P30928 V_MUMPM (P/V)RecName: Full = Non-structural protein V
P22112 SH_MUMPM (SH)RecName: Full = Small hydrophobic protein
P08362 HEMA_MEASE (H)RecName: Full = Hemagglutinin glycoprotein
Q89933 NCAP_MEASF (N)RecName: Full = Nucleoprotein
MEASLES P12576 L_MEASE (L)RecName: Full = RNA-directed RNA polymerase L
Q786F3 FUS_MEASC (F)RecName: Full = Fusion glycoprotein F0
P0C774 V_MEASC (P/V)RecName: Full = Non-structural protein V
POLS_RUBVM RecName: Full = Structural polyprotein (contains spike protein E1,
P08563
spike protein E2, capsid protein) 1063 aa
RUBELLA POLN_RUBVM RecName: Full = Non-structural polyprotein p200 (contains p90,
Q86500
p150 and p200 proteins) 2116 aa
P03301|POLG_POL1S RecName: Full = Genome polyprotein; 2209 aa CONTAINS:
POLIO P03301 P3; Protein 3AB; P1; Capsid protein VP0; Capsid protein VP4; Capsid protein VP2;
Capsid protein VP3
P04977 TOX1_BORPE (ptxA)RecName: Full = Pertussis toxin subunit 1
P04978 TOX2_BORPE (ptxB)RecName: Full = Pertussis toxin subunit 2
P04979 TOX3_BORPE (ptxC)RecName: Full = Pertussis toxin subunit 3
P0A3R5 TOX4_BORPE (ptxD)RecName: Full = Pertussis toxin subunit 4
P04981 TOX5_BORPE (ptxE)RecName: Full = Pertussis toxin subunit 5
PERTUSSIS
FHAC_BORPE (fhaC)RecName: Full = Filamentous hemagglutinin transporter
P35077
protein FhaC
P14283 PERT_BORPE (prn)RecName: Full = Pertactin autotransporter
P05788 FM2_BORPE (fim2)RecName: Full = Serotype 2 fimbrial subunit
P17835 FM3_BORPE (fim3)RecName: Full = Serotype 3 fimbrial subunit
TETANUS P04958 TETX_CLOTE (tetX)RecName: Full = Tetanus toxin
Q5PY51 Q5PY51_CORDP SubName: Full = Diphtheria toxin
DIPHTHERIA
Q6NK15 Q6NK15_CORDI (tox)SubName: Full = Diphtheria toxinVaccines 2020, 8, 559 4 of 20
Table 1. Cont.
UniProt
MICROBE List of Proteins
Identification
OMPA_NEIMB (porA)RecName:
MENINGOCOCCUS 0DH58
Full = Major outer membrane protein
P0DTC1 P0DTC1 Replicase polyprotein 1a (pp1a)
P0DTC2 P0DTC2 Spike glycoprotein (S)
P0DTC3 P0DTC3 Protein 3a (NS3a)
P0DTC4 P0DTC4 Envelope small membrane protein (E)
P0DTC5 P0DTC5 Membrane protein (M)
P0DTC6 P0DTC6 Non-structural protein 6 (NS6)
SARS-CoV-2 P0DTC7 P0DTC7 Protein 7a (NS7a)
P0DTC8 P0DTC8 Non-structural protein 8 (NS8)
P0DTC9 P0DTC9 Nucleoprotein (N)
P0DTD1 P0DTD1 Replicase polyprotein 1ab (pp1ab)
P0DTD2 P0DTD2 Protein 9b (NS9B)
P0DTD3 P0DTD3 Uncharacterized protein 14 (NS14)
P0DTD8 P0DTD8 Protein 7b (NS7b)
Mycobacterium MYCTU_UP
M. tuberculosis (strain ATCC 25618/3997 protein sequences; 1,332,562 total letters
tuberculosis 000001584
BORPE_UP B. pertussis strain Tohama I/ATCC BAA-589/NCTC
Bordetella pertussis
000002676 13251; 3260 proteins sequences
ECOLI_UP
Escherichia coli K12 Escherichia coli K12, 4403 protein sequences
000000625
9CLOT_UP
Clostridium leptum Clostridium leptum CAG:27 proteome; 2482 protein sequences
000018168
Lactobacillus LACP3_ UP Lactobacillus paracasei strain ATCC 334/BCRC;
paracasei 000001651 2708 protein sequences
LACLA_UP Lactococcus lactis subsp. lactis (strain IL1403);
Lactococcus lactis
000002196 2225 protein sequences
The LALIGN results were culled by applying the criterion that any sequence similarity reported
must have an E value of less than either 0.1 (Table 2) or 1.0 (Table 3), a Waterman–Eggert score of more
than 50, and a region containing at least six out of ten identities. These criteria are based on a number
of experimental studies involving the average length of peptide recognized by major histocompatibility
(MHC) receptors and T cell receptors (TCR), which is about 10 consecutive amino acids [13–15], and the
degree of similarity between two antigens that is likely to induce cross-reactive immune responses,
which generally consists of at least five consecutive identical amino acids or six identities distributed
within a 10 amino acid sequence [14,16–20].In essence, setting the E value to 0.1 or 1.0 determines
how many matches the BLAST program will yield. The lower the E value, the less matches BLAST
will yield because a lower E value limits the matches to those with rare combinations of amino acids
such as methionines, tryptophans, tyrosines, cysteines, etc., rather than ones made up of sequences of
very common amino acids such as glycine, alanine, valine and leucine, which appear at high rates
in almost all proteins. In this case, keeping the E value low also selects for matching sequences that
have a high probability of being antigenic since the immune system is more sensitive to rare amino
acids than to common ones. Conversely, the lower the Waterman–Eggert score, the less amino acid
matches are likely to be found in a pair of sequences. Thus, limiting the Waterman–Eggert score to
more than 50 provides reasonable assurance that any sequence that appears in the BLAST search
will display a high proportion of amino acid identities and similarities. Experience shows [16–20]
that the combination of low E value and high Waterman–Eggert score tends to yield reasonably short
sequences of high similarity, which is emphasized by using BLOSUM80. Despite using these boundaryVaccines 2020, 8, 559 5 of 20
conditions, however, experience shows that about half of the sequences that BLAST yields are unlikely
to be antigenically cross-reactive. As noted above, TCR and MHC recognize short peptide sequences
averaging about 10 amino acids in length [13–15] and experimental evidence has shown that within
such peptides, sequences of five contiguous identical amino acids or six non-contiguous amino acids
are generally required for two peptides to elicit cross-reactive T cell or B cell responses [14,16–20].
Thus, the BLAST results were culled for sequences meeting the latter criteria. By employing the
tried-and-tested set of parameters just described, previous experimentation demonstrates that the
resulting matches have a high probability of being recognized as cross-reactive antigens.
As controls for the LALIGN results, all thirteen SARS-Cov-2 proteins were used to search for
similarities to bacterial proteins found in diphtheria, pertussis, and tetanus vaccines (Table 1) and
viral proteins incorporated into the measles, mumps, rubella and polio vaccines. The only identified
proteins in Hib and meningitis vaccines are CRM197 or meningococcal outer membrane complex
protein, so these were also examined for similarities to SARS-CoV-2 proteins (Tables 1 and 2). The same
criteria used above were used to screen the results for sequences having at least six identities in a span
of ten amino acids.
Table 2. Summary of LALIGN searches set to E = 0.1 comparing SARS-CoV-2 proteins (left-hand column)
with vaccine proteins (see Table 1 for list of individual proteins). PNEUM = pneumococcal; CRM197
= Cross-Reactive Material 197; Acell PERT = acellular pertussis vaccine; DIPH = diphtheria vaccine;
TET = tetanus vaccine; Whole PERT = whole cell pertussis vaccine; BCG = Bacillus Calmette–Guerin,
here represented by M. tuberculosis. Avg/Pro = average number of matches per protein.
CRM RUB- MEAS- Acell
LALIGN E = 0.1 PNEUM MUMPS DIPH TET POLIO Men-ingitis
197 ELLA LES PERT
P0DTC1 Repl 1a 15 0 2 2 0 2 0 0 0 0
P0DTC2 Spike Prot 4 0 0 0 0 0 0 0 0 0
P0DTC3 Prot 3a 0 0 0 0 0 0 0 1 0 0
P0DTC4 Env Prot 0 0 0 0 0 0 0 0 0 0
P0DTC5 Memb Prot 0 1 2 0 0 0 0 0 0 0
P0DTC6 NS6 Prot 0 0 0 0 0 0 0 0 0 0
PODTC7 Prot 7a 0 0 0 0 0 0 0 0 0 0
P0DTC8 NS8 Prot 0 0 0 0 0 0 0 0 0 0
P0DTC9 Nucleoprot 2 0 0 0 0 0 0 0 0 0
P0DTD1 Repl 1ab 0 0 0 0 0 0 0 0 0 0
P0DTD2 NS9b Prot 0 0 0 0 0 0 0 0 0 0
P0DTD3 NS Prot 14 0 0 0 0 0 0 0 0 0 0
P0DTD8 Prot 7b 0 0 0 0 0 0 0 0 0 0
Total Matches 21 1 4 2 0 2 0 1 0 0
# Proteins 4 1 6 5 5 9 1 1 7 1
Avg/Prot 5.2 1.0 0.7 0.4 0 0.2 0 1.0 0 0
Bacillus Calmette–Guerin (BCG) vaccine could not be searched with the other vaccines. BCG is a
version of Mycobacterium bovis consisting of 3891 proteins. It has no integrated, searchable proteome
on BLAST (www.expasy.org); instead, each protein is separately listed in the UniProt database
(https://www.uniprot.org/uniprot/?query=taxonomy:410289). M. tuberculosis ([MYCTU_UP000001584]
Mycobacterium tuberculosis (strain ATCC 25618/comprised 3997 sequences) was substituted for BCG
since they are highly cross-reactive. Since searching nearly 4000 proteins using the LALIGN method
listed above was unreasonable, the complete proteome was searched instead and BLAST was used
with the parameters set similarly (BLOSUM80; E = 10; filter low complexity regions; no gaps permitted;
show best 100 matches). As with the other microbial comparisons, the results were hand curated to
eliminate any sequences failing to meet the six-in-ten antigenic-cross-reactivity criterion and an E valueVaccines 2020, 8, 559 6 of 20
of less than 1.0 (rather than 0.1, because this value gave equivalent length and quality of matches to the
LALIGN searches) and a Waterman–Eggert score of at least 50.
Table 3. Summary of LALIGN searches set to E = 1.0 comparing SARS-CoV-2 proteins (left-hand
column) with vaccine proteins (see Table 1 for list of individual proteins). Note that the BLAST
searches on Whole PERT and BCG were set to E = 10 because of the much larger size of the entire
genome as compared with the average of 17 proteins searched for in the other vaccines. PNEUM
= pneumococcal; CRM197 = Cross-Reactive Material 197; Acell PERT = acellular pertussis vaccine;
DIPH = diphtheria vaccine; TET = tetanus vaccine; Whole PERT = whole cell pertussis vaccine;
BCG = Bacillus Calmette–Guerin, here represented by M. tuberculosis. Avg/Pro = average number of
matches per protein.
CRM RUB- MEAS- Acell
LALIGN E = 1.0 PNEUM MUMPS DIPH TET POLIO Men-ingitis
197 ELLA LES PERT
P0DTC1 Repl 1a 26 4 18 9 6 2 3 1 3 3
P0DTC2 Spike Prot 4 0 5 2 2 0 0 6 1 2
P0DTC3 Prot 3a 2 0 6 1 2 0 0 1 1 0
P0DTC4 Env Prot 0 0 1 0 0 0 0 0 0 0
P0DTC5 Memb Prot 7 2 0 0 1 2 2 1 1 0
P0DTC6 NS6 Prot 0 1 1 0 0 0 0 0 0 0
PODTC7 Prot 7a 0 0 0 0 0 0 0 0 0 0
P0DTC8 NS8 Prot 2 0 0 0 0 0 0 0 0 0
P0DTC9 Nucleoprot 4 1 0 0 1 0 0 0 2 0
P0DTD1 Repl 1ab 6 2 3 0 0 2 0 0 0 0
P0DTD2 NS9b Prot 0 0 0 0 0 0 0 0 0 0
P0DTD3 Prot NS14 0 0 0 0 0 0 0 0 0 0
P0DTD8 Prot 7b 0 0 0 0 0 0 0 0 0 0
Total Matches 51 10 34 12 12 6 5 9 8 5
# Proteins 4 1 6 5 5 9 1 1 7 1
Avg/Prot 12.8 10.0 5.7 2.4 2.4 0.7 5.0 9.0 1.1 5
Bordetella pertussis vaccines come in two forms; one is acellular (which is the form tested above
using LALIGN) but there are also whole-cell pertussis vaccines, so the same BLAST procedure
used to examine M. tuberculosis was used to examine Bordetella pertussis UP000002676. Taxonomy,
257313—(strain Tohama I/ATCC BAA-589/NCTC 13251) comprised 3260 protein sequences.
As controls for the whole-bacteria BLAST searches, two human commensal bacteria, Escherichia
coli (Escherichia coli K12 UP000000625, 4403 protein sequences) and Clostridium leptum ([UP000018168]
Clostridium leptum CAG:27 proteome, 2482 protein sequences), as well as the probiotics Lactococcus lactis
([LACLA_UP000002196] Lactococcus lactis subsp. lactis (strain IL1403) 2225 protein sequences) and
Lactobacillus paracasei ([LACP3_UP000001651] Lactobacillus paracasei strain ATCC 334/BCRC, 2708 protein
sequences), were tested for similarities to SARS-CoV-2 proteins.
3. Results
Results of the LALIGN similarity searches that satisfy the criteria of at least six identical amino
acids in a sequence of ten amino acids and a Waterman–Eggert (W–E) score of 50 or greater are found
in Tables 2 and 3 and in the Figures. Results with E values of 0.1 or less are summarized in Table 2 and
Figures 1–4. Those that satisfy a W–E score of 50 or greater and an E value of 1.0 or less are summarized
in Table 3 but sequences are not provided as they are too numerous.
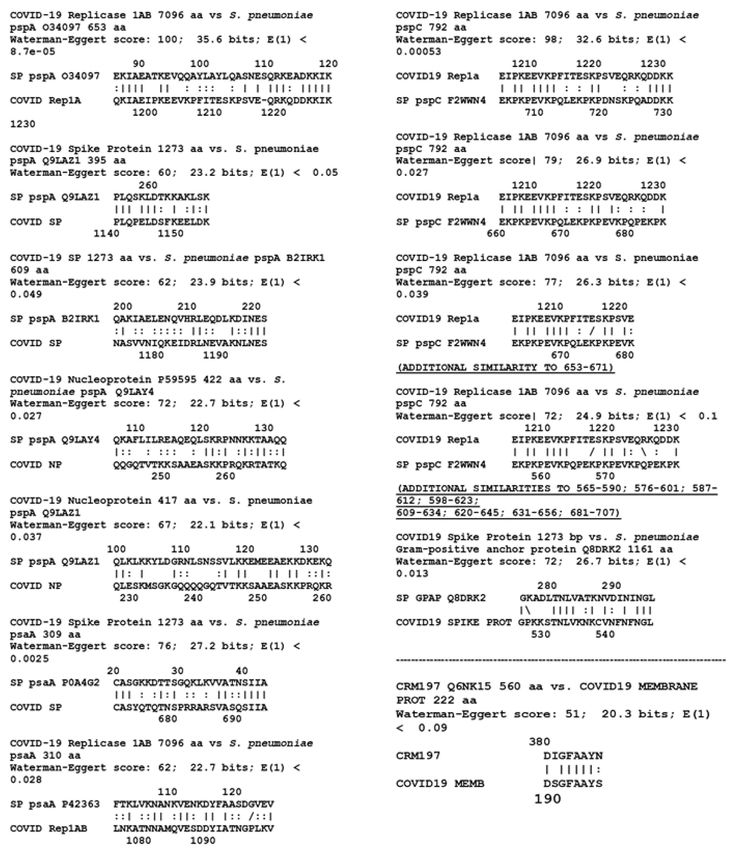
Table 2 demonstrates that pneumococcal proteins psaA, pspA and pspC present a very large
number of high-quality sequence matches with various SARS-CoV-2 proteins. All of these matches are
provided in Figure 1. Twenty-one significant similarities were observed, ten of which are indicatedVaccines 2020, 8, 559 7 of 20
in the figure in bold type as sequences that repeat within pairs of proteins. Note that a significant
sequence similarity was also found between SARS-CoV-2 proteins and the S. pneumoniae Gram-positive
anchor protein (Q8DRK2), which serves as an anchor site for capsular polysaccharides. It is not known
at this time whether this protein is among those contaminating capsular polysaccharide preparations,
but because of its association with polysaccharide anchoring, it is likely to be such a contaminant of the
polysaccharide material used in pneumococcal vaccines. Each of the four streptococcal proteins was
tested against each of the SARS-CoV-2 proteins, yielding 52 pairwise tests. Six of these combinations
yielded one or more matches that satisfied all similarity criteria employed here. An additional 30
matches between these pneumococcal proteins and SARS-CoV-2 proteins were found when E was
relaxed to 1.0 (Table 3) for a total, including the CRM197 matches, of 61.
One significant match at E = 0.1 was also found between CRM197 and the membrane protein
(P0DTC5) of SARS-CoV-2 (Table 2 and Figure 1) with an additional nine matches at E = 1.0 (Table 3).
However, there were no significant similarities at E = 0.1 between the meningococcal outer membrane
protein complex and any SARS-CoV-2 protein (Table 2), and only five when E was relaxed to 1.0 (Table 3).
Figure 1. Similarities between the four known or probable pneumococcal vaccine protein contaminants
PsaA, PspA, PspC, Gram-positive anchor protein and SARS-CoV-2 proteins, as well as CRM197,
the modified diphtheria toxin to which pneumococcal conjugate vaccines are attached. Multiple variants
for each protein were examined and the results provided here are representative of results at E = 0.1.Vaccines 2020, 8, 559 8 of 20
Figure 2. Similarities between nine SARS-CoV-2 proteins and 32 proteins from measles, mumps,
rubella, polio, Haemophilus influenzae type B (Hib), meningitis, diphtheria, pertussis and tetanus vaccines
(Table 1). A total of 288 pairwise combinations were searched. Only similarities satisfying the criteria
laid out in the Methods section are shown with E = 0.1.
Figure 2 displays the results for the pairwise tests of the thirteen SARS-CoV-2 proteins with the
additional bacterial and viral proteins listed in Table 1 that are present in measles, mumps, rubella,
polio, diphtheria, pertussis, and tetanus vaccines, for a total of 32 microbial proteins. Of these,
six yielded one or more significant similarities for a total of nine matches out of 416 possible pairwise
combinations (Table 2). When the E value was relaxed to 1.0 (Table 3), an additional 81 matches were
found, most notably between rubella vaccine proteins and SARS-CoV-2 proteins.
Results from the BLAST searches on whole bacteria are presented in Table 4. The 3997 M.
tuberculosis proteins yielded five significant similarities at an E value of 1.0 or less when compared
with the 13 SARS-CoV-2 proteins (51,961 combinations) (Figure 3). These matches are of roughly
equivalent quality to those of the LALIGN searches conducted on the other vaccine proteins described
above. The sequences are listed in Figure 3. Raising the E value to 10 and lowering the Waterman–Eggert
(W–E) score to 40 increased the total number of matches (still including at least six identities in a stretch
of 10 amino acids) to 36. These matches appear to be equivalent in quality to those found for E = 1.0
for the LALIGN searches. Similarly, the whole pertussis proteome (3260 proteins) yielded only six
matches at E = 0.1 and the W–E score at 50 (Table 2 and Figure 4), which increased to 55 when the
W–E score was lowered to 40 and E was raised to 1.0 (Table 3). However, these results do not differVaccines 2020, 8, 559 9 of 20
significantly from those obtained from commensal and probiotic control bacteria (Table 4): the average
number of matches per protein for the tuberculosis and pertussis bacteria at E = 1.0 was 0.0015 and at E
= 10.0, 0.013, whereas the average number of matches per protein for the control bacteria at E = 1.0 was
0.0015, and at E = 10.0, 0.014. These results suggest that the rate of matches between M. tuberculosis
and SARS-CoV-2 is what can be expected as the result of randomness rather than any of the tested
bacteria expressing particular protein sequences of relevance to the current study.
Large differences in the number of matches was found between pneumococcal proteins and
those from other protein antigen vaccines for the LALIGN E = 0.1 group (Table 2, Figures 1 and 2).
All four of the pneumococcal proteins and the CRM197 protein had significant similarities (i.e., meeting
the similarity criteria laid out in the Methods) to at least one of the thirteen SARS-CoV-2 proteins.
Altogether, seven of the 65 possible permutations of pneumococcal protein pairs yielded significant
similarities, or 10.8 percent. In contrast, only eight of the 35 viral and bacterial vaccine proteins other
than whole-cell pertussis and M. tuberculosis had significant matches to any of the nine SARS-CoV-2
proteins (1.8% of the 455 pairwise comparisons). The four pneumococcal proteins yielded 21 significant
matches with SARS-CoV-2 proteins, for an average of 5.25 per pneumococcal protein, while the 35
other vaccine proteins yielded only nine significant matches, for an average of 0.26 per protein. In other
words, at the E = 0.1 criterion, the probability of a match leading to cross-reactivity is over 20 times
more likely for pneumococcal proteins than for those from other vaccines.
Figure 3. SARS-CoV-2 protein similarities with Mycobacterium tuberculosis (Mtb). Note that BCG,
unlike the vaccines in Figures 1 and 2 that are composed of one to seventeen proteins, is composed
of 3993 proteins, so that even given the somewhat larger number of significant similarities displayed
here, the probability of them being major antigens is extremely small. Note also that because of the
size of the BCG proteome, BLAST (rather than LALIGN, as in Figures 1 and 2), was used to find these
similarities, and a cut-off value for significance of E = 1.0 rather than 0.1 was used.Vaccines 2020, 8, 559 10 of 20
Figure 4. SARS-CoV-2 protein similarities with Bordetella pertussis polyprotein (UniProte accession
number UP000002676). Note that whole B. pertussis is used as a vaccine. It is composed of 3260
proteins so that the probability that the matches shown are major antigens is extremely small. Note also
that because of the size of the size of the B. pertussis proteome, BLAST (rather than LALIGN, as in
Figures 1 and 2), was used to find these similarities, and a cut-off value for significance of E = 1.0 rather
than 0.1 was used, as was the case with M. tuberculosis (Figure 3) as well.
The E = 1.0 data (Table 3) yielded similar results. The pneumococcal proteins exhibited a total of
61 matches (including CRM197) with SARS-CoV-2 proteins for an average of 12.2 matches per protein.
The rest of the vaccines (other than whole cell pertussis and BCG) exhibited 90 total matches spread
out over 35 proteins for an average of 2.5 matches per protein. The 61 pneumococcal matches were
found among 23 of the 65 permutations with SARS-CoV-2 proteins, or 35.2 percent. In contrast, the 90
other vaccine matches were spread out over 53 of the 455 pairwise permutations, representing 11.6
percent of the possibilities. In other words, using the E = 1.0 criterion as a cutoff, it is three times more
likely that pneumococcal proteins will result in a cross-reactive match than for other proteins. In this
instance, rubella antigens account for more than thirty percent of the non-pneumococcal matches,
making rubella the next best candidate for protecting against SARS-CoV-2 infection.
The whole cell vaccines were treated separately from the limited antigen vaccines because BLAST
was used rather than LALIGN to perform the searches and because the average number of individual
vaccine protein matches to SARS-CoV-2 was very different: for the whole cell bacteria, it was 0.0145
with an SD of 0.0055, whereas the individual vaccine proteins (using the E =1.0 data in Table 3) is about
5.4 with a standard deviation of 2.6. For M. tuberculosis, for example, the best rate of matches was 40 outVaccines 2020, 8, 559 11 of 20
of 51,961 combinations [E = 10], or 0.08 percent, with an average of one match per 100 M. tuberculosis
proteins. At worst, using E =1.0, there were only 5 matches out of 51,961 combinations or 0.01 percent,
with one match per every 800 M. tuberculosis proteins. The pertussis results were very similar. On a
per-protein basis, these two bacteria resulted in rates of matches that were two orders of magnitude
lower than the other proteins tested (Tables 2 and 3). Thus, the percent of whole-bacteria matches
(Table 4) is clearly very much lower than the percent of matches for the limited-antigen vaccines listed
in Tables 2 and 3. The paucity of matches on a per-protein basis resulting from the tuberculosis and
pertussis bacteria comparisons is itself noteworthy, strongly suggesting that the quality of matches
reported in Figures 1 and 2 for the other vaccines are intrinsically extraordinary, and the pneumococcal
(both E = 0.1 and E = 1.0) and rubella (E = 1.0) results particularly so.
Table 4. Summary of BLAST search result matches between SARS-CoV-2 proteins (left-hand column)
and whole bacteria at E = 1.0 (shaded left-hand columns) and E = 10.0 (unshaded right-hand
columns): Bordetella pertussis (whole PERT); Mycobacterium tuberculosis (BCG); Clostridium leptum
(C. lept); Escherichia coli (E. coli); Lactococcus lactis (L. lact); Lactobacillus paracasei (L. para). Note that
in contrast to the LALIGN searches (Tables 2 and 3), the BLAST searches were set to E =1 or E = 10
because of the much larger size of the entire genome as compared with the average of 17 proteins
searched for the other vaccines (compare sequences in Figures 3 and 4 to Figures 1 and 2). Avg/Pro =
average number of matches per protein.
BLAST, E = 1.0 Whole C. E. L. L. Whole C. E. L. L.
BCG BCG
and 10.0 PERT lept coli lact para PERT lept coli lact para
P0DTC1 Repl 1a 0 5 0 2 0 1 5 4 4 6 4 3
P0DTC2 Spike Protein 1 0 0 0 0 1 9 4 1 6 1 4
P0DTC3 Protein 3a 0 0 0 1 2 0 10 6 7 5 4 4
P0DTC4 Env Protein 0 0 0 0 0 0 2 0 2 1 0 0
P0DTC5 Memb Prot 1 0 1 1 1 1 2 6 4 6 9 10
P0DTC6 NS6 Protein 1 0 0 0 1 0 4 1 2 0 10 5
PODTC7 Protein 7a 0 0 1 1 0 1 3 2 2 5 6 3
P0DTC8 NS8 Protein 0 0 0 1 0 0 2 1 2 3 1 3
P0DTC9 Nucleoprot 1 0 0 0 0 0 7 4 1 3 2 2
P0DTD1 Repl 1ab 1 0 0 0 1 0 5 4 3 3 4 5
P0DTD2 NS9b 0 0 0 0 0 0 0 3 4 5 3 3
P0DTD3 NS Protein 14 0 0 0 0 0 0 0 1 1 3 0 2
P0DTD8 Protein 7b 1 0 0 0 0 0 6 0 0 0 0 0
Total Matches 6 5 2 6 5 4 55 36 33 46 44 42
# Proteins 3260 3997 2482 4403 2225 2708 3260 3997 2482 4403 2225 2708
Avg/Prot 0.002 0.001 0.001 0.001 0.002 0.002 0.017 0.009 0.013 0.010 0.020 0.016
4. Discussion
The results of this study indicate that while pneumococcal vaccines are primarily composed
of polysaccharides, there are no obvious structural homologies between these polysaccharides and
SARS-CoV-2 glycosylations. The absence of such homologies does not rule out antigenic cross-reactivity
between these polysaccharides, but makes their identification difficult using anything other than
direct tests of whether SARS-CoV-2 antibodies recognize pneumococcal polysaccharides or whether
pneumococcal antibodies recognize SARS-CoV-2. Such tests might be worth conducting if only as
controls for studies of possible cross-reactivity between proteins found in pneumococcal vaccines and
SARS-CoV-2 proteins.
CRM197, which is used to conjugate pneumococcal polysaccharides in conjugate vaccines such
as the Prevnar series, and pneumococcal proteins known to contaminate the vaccines significantly,Vaccines 2020, 8, 559 12 of 20
both mimic SARS-CoV-2 proteins (Figure 1), satisfying rigid similarity and antigenicity constraints,
though there are many more high-quality matches between the pneumococcal proteins than with
CRM197. The results point specifically to potential cross-reactivity between SARS-CoV-2 proteins and
the pneumococcal proteins PspA and PsaA, which are known to contaminate polysaccharide-based
pneumococcal vaccines [5–7] as well as PspC, which it is reasonable to assume is another such
contaminant since it derives from the same outer membrane protein complex and is highly cross-reactive
with the antibodies against PspA used to demonstrate the presence of PspA in vaccines [10,11].
Such cross-reactivity would be consistent with epidemiological studies suggesting a protective effect of
pneumococcal vaccination against SARS-CoV-2 [1,2]. Since the CRM197 protein is used to conjugate
some Haemophilus and meningitis vaccines, these vaccines may also provide some cross-reactive
protection against SARS-Cov-2 proteins (Figure 1), a result that is consistent with the findings of
Pawlowski, et al. [2]. Further clinical and experimental tests of whether these vaccines elicit antibodies
that are cross-reactive with SARS-CoV-2 proteins are clearly needed.
It is important to emphasize that the fact that a microbe expresses an antigen that is sequentially
similar to a SARS-CoV-2 protein is not sufficient to guarantee that the two will elicit cross-reactive
immunity or, for that matter, any immune response whatsoever, since that sequence may not be
processed as an antigen by macrophages or presented to T cells. The full range of determinants of
antigenicity are as yet unknown. Among the key factors seem to be the concentration of the antigen,
how dissimilar it is from its host, where the antigen is expressed within a protein (e.g., whether it is
freely accessible in a random loop or protected within a pleated beta sheet), how the antigen is presented
to the immune system (e.g., by ingestion, inoculation, infection), and the inflammatory context in
which the antigen is processed (e.g., in the presence of an adjuvant or bystander infection) [21]. In this
context, it is notable that the rate of SARS-CoV-2 matches to pneumococcal vaccine antigens is 14%,
so that there is a reasonable chance of the immune system encountering a cross-reactive antigen, as is
the case for CRM197-conjugated vaccines and rubella and measles, whereas the rates of matches to
mycobacterial and pertussis antigens are very low (less than 0.1%). However, the data presented here
do not rule out the possibility of cross-reactivity to pertussis and/or mycobacterial proteins, though it is
striking that the rate of SARS-CoV-2 matches to pertussis and mycobacterial proteins is not significantly
different than to the commensal and probiotic control bacteria L. lactis, L. paracasei, C. leptum and E. coli
(Table 4). On the one hand, these data could be interpreted to mean that mycobacteria and pertussis are
as unlikely as the commensal and probiotic bacteria to protect against SARS-CoV-2. On the other hand,
if mycobacteria or pertussis bacteria are sufficient to induce protection against SARS-CoV-2, one might
argue that these commensal and probiotic bacteria could do so as well; since everyone encounters
them, protection against SARS-CoV-2 should then be universal. However, several factors undermine
this latter conclusion. One is that the mode of presentation of vaccines to the host immune system
is very different than that of commensal and probiotic bacterial antigens. Vaccines either actively
infect the host (e.g., polio or influenza), or are (more often) inoculated at very high concentrations;
in both cases, the resulting tissue damage initiates an immune response. Probiotic and commensal
microbes, in contrast, are retained (in healthy people) in the gut and do not cause tissue damage or
initiate an active immune response [22]. Additionally, the immune system often develops tolerance
for commensal and probiotic organisms and such organisms express large numbers of antigens that
mimic host antigens, including T cell receptors and human leukocyte antigens, thereby camouflaging
themselves from immune surveillance [23–27]. Thus, while any given commensal or probiotic microbe
has some small probability of expressing antigens that could potentially protect against SARS-CoV-2
infection, their general inability to elicit active immunity militates against this being a likely scenario.
The concentration of antigen presented to the immune system is also a determinant of whether an
active immune response results, so that microbes expressing very large numbers of antigens in very
small quantities are unlikely to elicit a strong immune response to most of them. The concentration of
protein contaminants in pneumococcal vaccines is clearly sufficient to induce immunity. CRM197 is
present in equal amounts to the capsular polysaccharides in the vaccines and is present because it isVaccines 2020, 8, 559 13 of 20
known to be highly antigenic. In Prevnar-13, for example, there are 30.4 µg of capsular polysaccharides
and 34.0 µg of CRM197 for a total of 64.4 micrograms of antigen per dose [28]. Protein contaminants
may make up an additional 3%, or 1.92 µg, of antigenic material according to WHO guidelines and
confirmed by laboratory analysis [5–7]. This 1.92 µg of protein is virtually identical to the 2.2 µg
of each of twelve of the capsular polysaccharides present (plus 4.4 µg of serotype 6) or the 2.3
micrograms of CRM197 conjugated to each polysaccharide type [28] and is therefore sufficient to
induce an immune response, especially since PspA and PspC are strongly antigenic and cross-reactive.
Pneumovax-23, in contrast, has 25 µg of each capsular polysaccharide, adding up to a total of 575 µg
of antigen [29]. The three percent protein contamination allowed by the WHO [5–7] could result in
17.25 µg of total PsaA, PspA and PspC per dose, which is certainly sufficient to induce immunity.
For comparison, each 0.5-mL dose of Adacel® , a diphtheria–tetanus–pertussis vaccine (Sanofi Pasteur),
contains only 2.5 µg detoxified pertussis toxoid, 5 µg FHA, 3 µg pertactin and 5 µg FIM acellular
pertussis antigens [30].
In addition to being present in concentrations that could induce protective immunity,
the pneumococcal-SARS-CoV-2 similarities reported here satisfy multiple criteria involving sequence
identities and search parameters for predicting potential antigenic cross-reactivity, so it is possible that
pneumococcal vaccination can protect individuals against SARS-CoV-2 disease. Evidence of protection
against SARS-CoV-2 by T cells reactive to unidentified, cross-reactive microbes has been reported by
several groups [31–33]. The studies report that 40 to 60% of people unexposed to SARS-CoV-2 had
SARS-CoV-2-reactive CD4+ T cells. This cross-reactivity is proposed to result from prior exposure to
coronaviruses that cause colds but this hypothesis has not yet been tested [33]. Moreover, the studies
also report that this cross-reactive immunity is greatest in young people and least in older people,
which is not consistent with cold virus exposures, nor is the fact that over 90% of people have T-cells
that are reactive to cold viruses but few seem to be immune to SARS-CoV-2 [33]. Such waning
immunity is, however, consistent with waning childhood vaccination immunity and particularly for
vaccinations such as pneumococci that are not universal. In light of the data presented here, it is
therefore possible that at least some proportion of individuals with cross-reactive immunity developed
it through exposure to pneumococcal vaccinations. Such cross-reactivity would also explain the
epidemiological observation that pneumococcal vaccination rates correlate inversely with rates of
serious SARS-CoV-2 disease and death, but that vaccination rates with other commonly used vaccines
(DTP, MMR, polio, meningitis, and BCG), do not [1].
One might ask whether the immunity conferred by pneumococcal (and perhaps other) vaccines is
sufficient to prevent SARS-CoV-2 infection completely. The current study is incapable of addressing that
question meaningfully but the fact that the vast majority of similarities between pneumococcal proteins
and SARS-CoV-2 involve the replicase (Tables 2 and 3) suggests that any protection would be reactive
rather than preventative. The reason for this is that the replicase is not expressed until cells are infected so
that pneumococcal-related immunity would mainly come into play only at that point. This factor might
explain why many people seem to become infected with SARS-CoV-2 and remain infectious without
themselves displaying symptoms of COVID-19 [34–38]. Indeed, increasing evidence indicates that
the primary protection against SARS-CoV-2 is T-cell-mediated rather than antibody-mediated [31–33],
suggesting that control of the infection is at the level of cellular infection rather than against free
virus. Nonetheless, it is notable that the next most prevalent set of SARS-CoV-2–pneumococcal protein
similarities after the replicase involve the viral spike protein (Tables 2 and 3), which is a major target
for antibodies and which might, therefore, mediate SARS-CoV-2 infectivity.
The observation that viral and bacterial proteins exhibit antigens similar enough to be cross-reactive
may be surprising but it is not novel. Härkönen, et al. [39] found that rabbit antibodies to HSP65 of
Mycobacterium bovis (from which BCG is derived) recognized capsid protein VP1 of coxsackievirus
A9, VP1, and/or VP2 of coxsackievirus B4. Misko, et al. [40] demonstrated that Epstein–Barr virus
mimicked a Staphylococcus aureus replication initiation protein and induced antibodies cross-reactive
with it. Trama, et al., [41] and Williams, et al. [42] have documented antibodies against the gp41Vaccines 2020, 8, 559 14 of 20
protein of human immunodeficiency virus that cross-react with commensal bacteria in the human gut.
Ross, et al. [43] reported that sera from chickens inoculated with infectious bursal disease viruses or
infectious bursal disease vaccines cross-reacted with Mycoplasma gallisepticum and Mycoplasma synoviae.
In addition, Bordenave [44] found that antibodies against Salmonella abortusequi also recognized tobacco
mosaic virus. In short, while the phenomenon may be rare—and, indeed, the data reported here
suggests that such similarities may occur at a rate as high as 1/70 pairwise protein combinations or as
low as 1/1000—bacterial antigens are known to occasionally induce antibodies that cross-react with
viral antigens or vice versa. This observation is consistent with the fact that every possible sequence of
five amino acids has been shown to appear randomly in the microbial proteome [45,46]. Completely
unrelated microbes should, therefore, have a small, but finite, probability of expressing identical
antigens capable of inducing cross-reactive immune responses. The question becomes one of whether
these antigens are ever encountered by the host and presented to the immune system in a way that
initiates cross-reactive immunity.
The almost completely negative results reported here for antigenic mimicry between SARS-CoV-2
proteins and proteins from measles, mumps, diphtheria, pertussis and tetanus at E = 0.1 (Table 1),
and the relatively low rate of similarities with poliovirus at E = 1.0 (Table 2), are consistent with the lack
of association between these vaccines and SARS-CoV-2 rates of disease or death [1], although Pawlowski,
et al. [2] found some protective effect from polio vaccination and the measles–mumps–rubella (MMR)
combination vaccine. The current study would suggest that the rubella component of MMR is
the major protective agent, though measles also exhibits some high-quality antigenic similarities to
SARS-CoV-2. Indeed, Franklin, et al., [47] also report significant similarities between both rubella
and measles proteins and SARS-CoV-2, and their key results were independently reproduced here in
Figure 2. Additionally, Gold [48] has also proposed that the measles–mumps–rubella vaccine may
confer protection against SARS-CoV-2. However, there are significantly fewer similarities between
measles and rubella proteins and those of SARS-CoV-2 proteins (and none with mumps proteins)
than there are with pneumococcal proteins, making pneumococci a much higher probability source of
protection. Moreover, epidemiological evidence does not support measles containing vaccines (which
often include rubella) as protective against SARS-CoV-2, though using measles-containing vaccines as
Root-Bernstein [1] did, may hide important rubella-related protection since not all measles-containing
vaccines include rubella and rubella vaccination can be performed independently from measles
vaccination. The suggestion that the polio vaccine be tested as a SARS-CoV-2 vaccine [49] is likewise
not well-supported by either the data presented here, which found only one significant similarity
between polio proteins and SARS-CoV-2 proteins at E = 0.1 and five at E = 1.0 (Tables 1 and 2 and
Figure 2), or by epidemiological data [1], though, once again, Pawlowski, et al. [2] found some
protective effect in children.
The data presented here must be interpreted both probabilistically—which is to say as a guide
to whether any particular vaccine has a greater or lesser probability of providing antigens that are
both cross-reactive and protective against SARS-CoV-2 infection or complications—and antigenically,
which is a measure of how strong an immune response a sequence actually elicits. Using both criteria,
pneumococcal vaccine antigens are the most probable candidates for providing such protection since
there are many matches and the pneumococcal proteins are known to be highly antigenic. The rubella
antigens are the next most likely for the same reasons. However, we cannot know for certain until
the appropriate immunological cross-reactivity studies are conducted to determine both whether
antibodies against the vaccine antigens recognize SARS-CoV-2 antigens and protect against infection,
and whether SARS-CoV-2 antibodies recognize the potentially cross-reactive antigens identified in
Figures 1–4.
The criteria just described apply equally to considerations of whether there is cross-reactivity
to the BCG vaccine. Tuberculosis (BCG) vaccination has also been proposed to protect against
SARS-CoV-2 [50]. While BCG vaccination was purported to be associated with SARS-CoV-2 protection
in several epidemiological studies (reviewed in [51]), that result was not replicated in others (e.g., [1,2,52])Vaccines 2020, 8, 559 15 of 20
and serious concerns about methodologies have called into question the association [51,53]. The current
study leads to the conclusion that BCG protection against SARS-CoV-2 is unlikely. While between 5
(E = 0.1) and 40 (E = 1.0) similarities were found between M. tuberculosis proteins and SARS-CoV-2
proteins, this number is insignificant in relation to the number of proteins expressed by M. tuberculosis
and BCG (approximately 4000). This paucity of significant M. tuberculosis similarities (0.04%) as
compared with the high incidence of pneumococcal similarities (11.6–14%) makes it probable that
pneumococcal proteins will induce cross-reactive antibodies and extremely unlikely that any of
the M. tuberculosis antigens will do so. Indeed, none of the M. tuberculosis proteins identified in
Figure 3 are among the known dominant antigens expressed by either M. tuberculosis infection or BCG
vaccination [54–58].
The question of whether pertussis antigens may protect against SARS-CoV-2 is more complicated
than that for BCG. There appear to be no epidemiological studies associating pertussis vaccination
with protection against SARS-CoV-2 infection or death and the one study that has looked for such an
association found none [1]. However, while acellular pertussis vaccines have a very small number
of sequences that are potentially cross-reactive with SARS-CoV-2 proteins, the whole cell vaccine,
which is still available in some countries, has many matches specifically to the SARS-CoV-2 spike
protein, which is a major target of neutralizing antibodies (Table 4). The difficulty is that with 3260
proteins in the whole cell vaccine, the probability that any of these potentially cross-reactive sequences
are actually processed as major antigens inducing significant antibody responses is small, particularly
compared to pneumococcal and rubella vaccines (Tables 1 and 2). However, some of these proteins
have been incorporated into the acellular pertussis vaccines and are known to be highly antigenic.
Thus, the total number of matches is probably a less useful predictor of antigenic cross-reactivity than
whether the potentially cross-reactive proteins are known to be highly antigenic, as is the case with the
pneumococcal and rubella proteins. Again, theory can be a guide here, but experiment will provide
the final answers.
Finally, it must be mentioned that the correlations between pneumococcal vaccination (and
perhaps other vaccinations) and decreased risk of SARS-CoV-2 cases and deaths may be due not to
cross-reactivity between pneumococcal (or other vaccine) antigens and SARS-CoV-2 antigens but rather
to protection against super-infection of SARS-CoV-2 by pneumococci and other bacteria. While it is
common to attribute all of the symptoms of COVID-19 to SARS-CoV-2 infection, a rapidly expanding
literature is demonstrating that, as with influenza [59,60], serious COVID-19 cases are characterized
by bacterial super-infections of which pneumococci, Haemophilus influenzae and Mycoplasmas are
the most common [61–69]. For example, a recent study from China found that 60% of COVID-19
patients had streptococcal infections, about 55% Klebsiella pneumoniae infections and 40% had Hib [70].
Indeed, severe COVID-19 cases are characterized by elevated procalcitonin levels [68,69] and by
eosinopenia [66,67], both of which are diagnostic for disseminated bacterial infections [71,72]. If this is
the case, then pneumococcal and Hib vaccination may not prevent SARS-CoV-2 infection but should
decrease the probability of developing the complications associated with severe COVID-19 disease.
5. Conclusions
To conclude, there are many reasons to investigate whether pneumococcal, Hib, meningitis and
rubella vaccination may protect against SARS-CoV-2 infection or complications. Epidemiologically, a
strong inverse association of pneumococcal vaccinations with rates of SARS-CoV-2 rates of disease
and death has been documented by two studies [1,2]. The epidemiological association makes sense in
terms of the particular proteins found in pneumococcal vaccines that are identified in this study as
being potentially protective. These are CRM197, PspA, PsaA and PspC, all proteins known to be highly
antigenic [73]. Since CRM197 is also found in Hib vaccines, which have also been associated with
protection against SARS-CoV-2 [2], its cross-reactivity with SARS-CoV-2 proteins should be investigated.
The other pneumococcal proteins (PspA, psaA and PspC) are under active investigation as more
effective and broadly protective pneumococcal vaccine components to replace the polysaccharide-basedVaccines 2020, 8, 559 16 of 20
vaccines [74–77]. Some of these vaccine candidates are already in human trials [77,78]. Thus, it should
be possible rapidly and readily to determine whether such pneumococcal protein-based vaccines can
be effective mitigators of SARS-CoV-2 disease and these vaccines may provide needed protection until
a SARS-CoV-2 vaccine is produced in sufficient quantities to be effective worldwide. Finally, rubella
vaccination should also be investigated further since rubella proteins have the second highest rate of
similarities to SARS-CoV-2 proteins in this study and rubella vaccination has been reported to have
some protective efficacy against SARS-CoV-2 [2].
Because pneumococcal vaccination has the highest degree of protection in both studies that have
compared it with other vaccines [1,2], it seems logical to focus current efforts on this type of vaccination.
Regardless of the efficacy of such pneumococcal vaccines in protecting against serious SARS-CoV-2
infection, increased use of pneumococcal vaccination should be urged because the world will be facing
dual epidemic/pandemics this coming fall and winter and perhaps for many years hereafter, involving
concurrent influenza and SARS-CoV-2. Increasing pneumococcal and Hib (which also contains
CRM197) vaccination coverage has been demonstrated to be one of the most effective means to lower
the incidence of pneumonias and intensive care unit cases following influenza infections [79,80]. At a
minimum, decreasing the rates of invasive pneumococcal and Haemophilus influenzae superinfections
following influenza infections will free up badly needed resources, personnel and intensive care units
for treating SARS-CoV-2 patients. Several nations have already adopted, or are considering, policies
to increase pneumococcal vaccination coverage for just this reason [81–84]. If the current research
is accurate, Hib should be added to this list and nations adopting these policies may also benefit in
having fewer serious SARS-CoV-2 cases because of protection from cross-reactive antigens. This is a
no-lose and possibly a win-win situation.
Funding: This research received no external funding.
Conflicts of Interest: The author declares no conflict of interest.
References
1. Root-Bernstein, R. Age and Location in Severity of COVID-19 Pathology: Do Lactoferrin and Pneumococcal
Vaccination Explain Low Infant Mortality and Regional Differences? BioEssays 2020. [CrossRef]
2. Pawlowski, C.; Puranik, A.; Bandi, H.; Venkatakrishnan, A.J.; Agarwal, V.; Kennedy, R.; O’Horo, J.C.;
Gores, G.J.; Williams, A.W.; Halamka, J.; et al. Exploratory analysis of immunization records highlights
decreased SARS-CoV-2 rates in individuals with recent non-COVID-19 vaccinations. medRxiv 2020. [CrossRef]
3. Watanabe, Y.; Allen, J.D.; Wrapp, D.; McLellan, J.S.; Crispin, M. Site-specific glycan analysis of the SARS-CoV-2
spike. Science 2020, eabb9983. [CrossRef] [PubMed]
4. Shajahan, A.; Supekar, N.T.; Gleinich, A.; Azadi, P. Deducing the N- and O-glycosylation profile of the spike
protein of novel coronavirus SARS-CoV-2. Glycobiology 2020. [CrossRef]
5. WHO. Recommendations to Assure the Quality, Safety and Efficacy of Pneumococcal Conjugate Vaccines;
World Health Organization: Geneva, Switzerland, 2009.
6. Lee, C.; Chun, H.J.; Park, M.; Kim, R.K.; Whang, Y.H.; Choi, S.K.; Baik, Y.O.; Park, S.S.; Lee, I. Quality
Improvement of Capsular Polysaccharide in Streptococcus pneumoniae by Purification Process Optimization.
Front. Bioeng. Biotechnol. 2020, 8, 39. [CrossRef] [PubMed]
7. Morais, V.; Dee, V.; Suárez, N. Purification of Capsular Polysaccharides of Streptococcus pneumoniae:
Traditional and New Methods. Front. Bioeng. Biotechnol. 2018, 6. [CrossRef]
8. Yu, X.; Sun, Y.; Frasch, C.; Concepcion, N.; Nahm, M.H. Pneumococcal Capsular Polysaccharide Preparations
May Contain Non-C-Polysaccharide Contaminants That Are Immunogenic. Clin. Diagn. Lab. Immunol. 1999,
6, 519–524. [CrossRef]
9. Yu, J.; Briles, D.E.; Englund, J.A.; Hollingshead, S.K.; Glezen, W.P.; Nahm, M.H. Immunogenic Protein
Contaminants in Pneumococcal Vaccines. J. Infect. Dis. 2003, 187, 1019–1023. [CrossRef]
10. Brooks-Walter, A.; Briles, D.E.; Hollingshead, S.K. The pspC Gene of Streptococcus pneumoniae Encodes a
Polymorphic Protein, PspC, Which Elicits Cross-Reactive Antibodies to PspA and Provides Immunity to
Pneumococcal Bacteremia. Infect. Immun. 1999, 67, 6533–6542. [CrossRef]Vaccines 2020, 8, 559 17 of 20
11. Ogunniyi, A.D.; Woodrow, M.C.; Poolman, J.T.; Paton, J.C. Protection against Streptococcus pneumoniae
Elicited by Immunization with Pneumolysin and CbpA. Infect. Immun. 2001, 69, 5997–6003. [CrossRef]
12. Möginger, U.; Resemann, A.; Martin, C.E.; Parameswarappa, S.; Govindan, S.; Wamhoff, E.-C.; Broecker, F.;
Suckau, D.; Pereira, C.L.; Anish, C.; et al. Cross Reactive Material 197 glycoconjugate vaccines contain
privileged conjugation sites. Sci. Rep. 2016, 6, 20488. [CrossRef] [PubMed]
13. Rudensky, A.Y.; Preston-Hurlburt, P.; Hong, S.-C.; Barlow, A.; Janeway, C.A. Sequence analysis of peptides
bound to MHC class II molecules. Nature 1991, 353, 622–627. [CrossRef] [PubMed]
14. Hemmer, B.; Kondo, T.; Gran, B.; Pinilla, C.; Cortese, I.; Pascal, J.; Tzou, A.; McFarland, H.F.; Houghten, R.;
Martin, R. Minimal peptide length requirements for CD4+ T cell clones—Implications for molecular mimicry
and T cell survival. Int. Immunol. 2000, 12, 375–383. [CrossRef]
15. Ekeruche-Makinde, J.; Miles, J.J.; Berg, H.A.V.D.; Skowera, A.; Cole, D.K.; Dolton, G.; Schauenburg, A.J.A.;
Tan, M.P.; Pentier, J.M.; Llewellyn-Lacey, S.; et al. Peptide length determines the outcome of
TCR/peptide-MHCI engagement. Blood 2013, 121, 1112–1123. [CrossRef] [PubMed]
16. Cunningham, M.W.; McCormack, J.M.; Fenderson, P.G.; Ho, M.K.; Beachey, E.H.; Dale, J.B. Human
and murine antibodies cross-reactive with streptococcal M protein and myosin recognize the sequence
GLN-LYS-SER-LYS-GLN in M protein. J. Immunol. 1989, 143, 2677–2683.
17. Kanduc, D. Quantifying the possible cross-reactivity risk of an HPV16 vaccine. J. Exp. Ther. Oncol. 2009, 8,
65–76.
18. Root-Bernstein, R. Autoreactive T-cell receptor (Vbeta/D/Jbeta) sequences in diabetes are homologous to
insulin, glucagon, the insulin receptor, and the glucagon receptor. J. Mol. Recognit. 2009, 22, 177–187.
19. Root-Bernstein, R. Rethinking Molecular Mimicry in Rheumatic Heart Disease and Autoimmune Myocarditis:
Laminin, Collagen IV, CAR, and B1AR as Initial Targets of Disease. Front. Pediatr. 2014, 2, 85. [CrossRef]
20. Root-Bernstein, R. T Cell Receptor Variable Regions in Diabetes Bind to Each Other, to Insulin, Glucagon or
Insulin Receptor, and to Their Antibodies. Open Autoimmun. J. 2012, 4, 10–22. [CrossRef]
21. Root-Bernstein, R. How to Make a Non-Antigenic Protein (Auto) Antigenic: Molecular Complementarity
Alters Antigen Processing and Activates Adaptive-Innate Immunity Synergy. Anti-Cancer Agents Med. Chem.
2015, 15, 1242–1259. [CrossRef]
22. Takiishi, T.; Fenero, C.M.; Câmara, N.O.S. Intestinal barrier and gut microbiota: Shaping our immune
responses throughout life. Tissue Barriers 2017, 5, e1373208. [CrossRef] [PubMed]
23. Damian, R.T. Molecular Mimicry in Biological Adaptation. Science 1965, 147, 824. [CrossRef] [PubMed]
24. De Groot, A.S.; Moise, L.; Liu, R.; Gutierrez, A.; Tassone, R.; Bailey-Kellogg, C.; Martin, W. Immune
camouflage: Relevance to vaccines and human immunology. Hum. Vaccines Immunother. 2014, 10, 3570–3575.
[CrossRef]
25. Moise, L.; Beseme, S.; Tassone, R.; Liu, R.; Kibria, F.; Terry, F.; Martin, W.; De Groot, A.S. T cell epitope
redundancy: Cross-conservation of the TCR face between pathogens and self and its implications for vaccines
and autoimmunity. Expert Rev. Vaccines 2016, 15, 607–617. [CrossRef] [PubMed]
26. Root-Bernstein, R. Autoimmunity and the microbiome: T-cell receptor mimicry of “self” and microbial
antigens mediates self tolerance in holobionts. BioEssays 2016, 38, 1068–1083. [CrossRef]
27. Root-Bernstein, R. Human Immunodeficiency Virus Proteins Mimic Human T Cell Receptors Inducing
Cross-Reactive Antibodies. Int. J. Mol. Sci. 2017, 18, 2091. [CrossRef]
28. Bobes, N.S. Package inserts. N. Engl. J. Med. 1968, 278, 282.
29. FDA. Package Insert. PNEUMOVAX 23 1983. Available online: https://www.fda.gov/media/80547/download
(accessed on 28 June 2020).
30. CDC. About Diphtheria, Tetanus, and Pertussis Vaccines. 2020. Available online: https://www.cdc.gov/
vaccines/vpd/dtap-tdap-td/hcp/about-vaccine.html (accessed on 28 June 2020).
31. Grifoni, A.; Weiskopf, D.; Ramirez, S.I.; Mateus, J.; Dan, J.M.; Moderbacher, C.R.; Rawlings, S.A.;
Sutherland, A.; Premkumar, L.; Jadi, R.S.; et al. Targets of T Cell Responses to SARS-CoV-2 Coronavirus in
Humans with COVID-19 Disease and Unexposed Individuals. Cell 2020, 181, 1489–1501.e15. [CrossRef]
32. Mateus, J.; Grifoni, A.; Tarke, A.; Sidney, J.; Ramirez, S.I.; Dan, J.M.; Burger, Z.C.; Rawlings, S.A.; Smith, D.;
Phillips, E.J.; et al. Selective and cross-reactive SARS-CoV-2 T cell epitopes in unexposed humans. Science
2020, eabd3871. [CrossRef]
33. Sette, A.; Crotty, S. Pre-existing immunity to SARS-CoV-2: The knowns and unknowns. Nat. Rev. Immunol.
2020, 20, 1–2. [CrossRef]You can also read