3D and 4D ultrasound in fetal cardiac scanning: a new look at the fetal heart
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Ultrasound Obstet Gynecol 2007; 29: 81–95
Published online in Wiley InterScience (www.interscience.wiley.com). DOI: 10.1002/uog.3912
3D and 4D ultrasound in fetal cardiac scanning: a new look
at the fetal heart
S. YAGEL*, S. M. COHEN*, I. SHAPIRO† and D. V. VALSKY*
*Department of Obstetrics and Gynecology, Hadassah-Hebrew University Medical Centers, Jerusalem and †Department of Obstetrics and
Gynecology, Bnai Zion Medical Center, Haifa, Israel
K E Y W O R D S: 3D-4D ultrasound; fetal echocardiography; inversion mode; power Doppler; STIC; tomographic ultrasound
imaging
ABSTRACT of its offline networking capabilities may improve health-
care delivery systems. These features may work to extend
Over the last decade we have been witness to a the benefits of prenatal cardiac screening to poorly-served
burgeoning literature on three-dimensional (3D) and areas. The introduction of ‘virtual planes’ to fetal car-
four-dimensional (4D) ultrasound-based studies of the diac scanning has helped sonographers obtain views of
fetal cardiovascular system. Recent advances in the the fetal heart not generally accessible with a standard
technology of 3D/4D ultrasound systems allow almost two-dimensional (2D) approach.
real-time 3D/4D fetal heart scans. It appears that It is perhaps too early to evaluate whether 3D/4D
3D/4D ultrasound in fetal echocardiography may make a cardiac scanning will improve the accuracy of fetal
significant contribution to interdisciplinary management echocardiography programs. However, there is no doubt
team consultation, health delivery systems, parental that 3D/4D ultrasonography gives us another look at the
counseling, and professional training. fetal heart.
Our aim is to review the state of the art in 3D/4D fetal The purpose of this review is to summarize the recent
echocardiography through the literature and index cases technological advances in 3D/4D fetal echocardiography,
of normal and anomalous fetal hearts. Copyright 2007 demonstrating their application through normal and
ISUOG. Published by John Wiley & Sons, Ltd. anomalous case examples.
3D/4D TECHNIQUES AND THEIR
INTRODUCTION APPLICATION TO FETAL CARDIAC
SCANNING
Three-dimensional (3D) and four-dimensional (4D) appli-
cations in fetal ultrasound scanning have made impressive Spatio-temporal image correlation (STIC)
strides in the past two decades. Today, many more centers STIC acquisition is an indirect motion-gated offline
have 3D/4D ultrasound capabilities at their command, scanning mode1 – 4 . The automated volume acquisition is
and we are witness to a burgeoning literature of 3D/4D- made possible by the array in the transducer performing
based studies. Perhaps in no other organ system is this a slow single sweep, recording a single 3D data set
recent outstanding progress so evident as in the fetal car- consisting of many 2D frames one behind the other.
diovascular system. Recent technological developments The volume of interest (VOI) is acquired over a period
of motion-gated cardiac scanning allow almost real-time of about 7.5 to 30 s at a sweep angle of approximately
3D/4D heart examination. It appears from this growing 20–40◦ (depending on the size of the fetus) and frame
body of literature that 3D/4D ultrasonography can make a rate of about 150 frames per second. A 10-second, 25◦
significant contribution to our understanding of the devel- acquisition would contain 1500 B-mode images4 .
oping fetal heart in both normal and anomalous cases, Following acquisition the ultrasound system applies
to interdisciplinary management team consultation, to mathematical algorithms to process the volume data and
parental counseling, and to professional training. 3D/4D detect systolic peaks, which are used to calculate the
ultrasound may facilitate screening methods, and by dint fetal heart rate. The B-mode images are arranged in order
Correspondence to: Prof. S. Yagel, Department of Obstetrics and Gynecology, Hadassah-Hebrew University Medical Centers, PO Box
24035, Mt. Scopus, Jerusalem, Israel (e-mail: simcha.yagel@gmail.com)
Accepted: 17 November 2006
Copyright 2007 ISUOG. Published by John Wiley & Sons, Ltd. REVIEW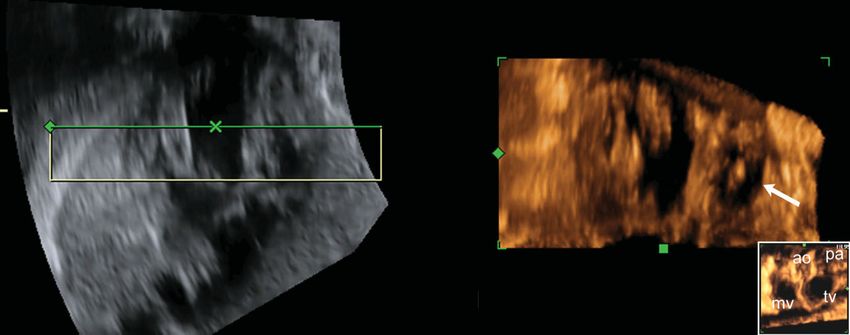
82 Yagel et al.
(a)
0 sec. 1 sec. 2 sec. 3 sec.
First cycle (total 4 seconds) Second cycle
(b)
1
Contracting
object Combining frames
scanned in three of identical phase
1 2 3 consecutive in the cycle from
Time from slices consecutive slices
beginning of cycle Frame's spacial
Total cycle duration: 2 position is restored
4 seconds
3
Frames Frames Frames
acquired in acquired in acquired in
first 2D slice second 2D slice third 2D slice
0 sec.
1 sec.
2 sec.
3 sec
(c)
0 sec. 1 sec. 2 sec. 3 sec.
Repetition of
Reconstructed cycle reconstructed cycle
(d)
Copyright 2007 ISUOG. Published by John Wiley & Sons, Ltd. Ultrasound Obstet Gynecol 2007; 29: 81–95.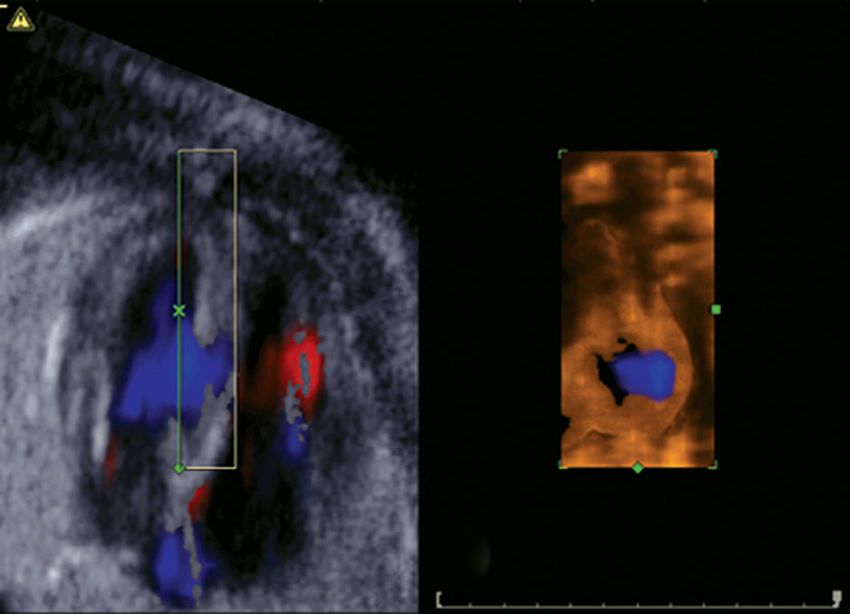
Ultrasound in fetal cardiac scanning 83
according to their spatial and temporal domain, correlated
to the internal trigger, the systolic peaks that define
the heart cycle4 (Figure 1). The resultant 40 consecutive
volumes are a reconstructed complete heart cycle that
displays in an endless loop. This cine-like file of a beating
fetal heart can be manipulated to display any acquired
scanning plane at any stage in the cardiac cycle (Figure 2).
While a complex process to describe, this reconstruction
takes place directly following the scan in a matter of
seconds; the STIC acquisition can be reviewed with the
patient still present and repeated if necessary, and saved
to the scanning machine or a network. Optimal STIC
acquisition technique for examination of the fetal heart is
thoroughly and succinctly described by Goncalves et al.5 .
In post-processing, various methodologies have been
proposed to optimize the acquisition to demonstrate the
classic planes of fetal echocardiography6,7 (Figure 3), as
well as ‘virtual planes’ that are generally inaccessible in
2D cardiac scanning8 – 11 . These views once obtained are
likewise stored in the patient’s file, in addition to the
original volume, either as static images or 4D motion
files. Any of the stored information can be shared for
expert review, interdisciplinary consultation, parental
counseling, or teaching.
STIC is an acquisition modality that can be combined
with other applications by selecting the appropriate setting
before acquisition (B-flow, color and power Doppler,
tissue Doppler, high-definition flow Doppler) or with post-
processing visualization modalities (3D volume rendering,
inversion mode, tomographic ultrasound imaging).
Multiplanar reconstruction (MPR), 3D rendering, and Figure 2 Ultrasound image showing the four-chamber view from a
tomographic ultrasound imaging (TUI) spatio-temporal image correlation acquisition in a third-trimester
fetus in systole (a) and diastole (b). By applying multiplanar
3D/4D volume sets contain a ‘block’ of information, reconstruction the operator optimizes the four-chamber view plane,
which is generally a wedge-shaped chunk of the targeted adjusting the image both spatially along the x-, y- and z-axes, and
area. In order to analyze this effectively, the operator dis- to the desired stage of the cardiac cycle. The navigation point is
placed on the interventricular septum in the A-plane; the B-plane
plays 2D planes in either MPR mode (Figure 2), or in 3D shows the septum ‘en face’, and the C-plane shows a coronal plane
volume rendering. In MPR the screen is divided into four through the ventricles.
frames, referred to as A (upper left), B and C; the fourth
frame (lower right) will show either the volume model for
reference, or the rendered image. Each of the three frames The reference dot guides the operator in navigating within
shows one of the three orthogonal planes of the volume. the volume, as it is anchored at the point of intersection
Figure 1 Schematic demonstration of STIC technology. Cycle duration, number of slices, and number of frames per slice were chosen to
simplify illustration. The scale applicable to fetal cardiac examination is discussed in the text. (a) The heart is represented by an object that
contracts in a cyclical manner (4 seconds per cycle). The shape of the object is presented at four points during the cycle. Assume that the
contraction rate is too high for scanning the whole object in conventional real-time 3D. (b) Segmental real-time scanning and reconstruction
according to position in space and phase of appearance. The object is scanned in three consecutive slices adjacent to each other. This is done
automatically by changing the angle of the internal 2D transducer within the ‘‘box’’ of the 3D transducer (1). At least one complete cycle is
recorded in real-time 2D ultrasound, thus acquiring many frames per slice. In this example four frames are recorded in each slice (2). By
simultaneous analysis of the tissue movements, the software identifies the beginning of each cycle and sets the time each frame was acquired
in respect to the beginning of the cycle. Knowing the time and position of each frame the software reconstructs the 3D shape of the complete
object in each phase of the cycle (3). The shape is constructed from frames arranged side by side according to their position in the object
(hence spatio-temporal). Though each frame composing the object was acquired in a different cycle, their phase in respect to the beginning of
the cycle is identical (hence spatio-temporal). (c) The system completes its task by creating an endless loop animation composed of the
consecutive reconstructed volumes of the cycle, resulting in a moving volume resembling real-time 3D. The procedure takes only a few
seconds; the stored reconstructed volumes are now available for analysis with post processing techniques as described in the text.
(d) Schematic demonstration of the multiple slices through the heart acquired during a single STIC scan. The dedicated transducer
automatically changes its scanning angle, either by means of a small motor in some systems, or electronically by using a phased matrix of
elements. A complete 2D cycle is acquired in each slice.
Copyright 2007 ISUOG. Published by John Wiley & Sons, Ltd. Ultrasound Obstet Gynecol 2007; 29: 81–95.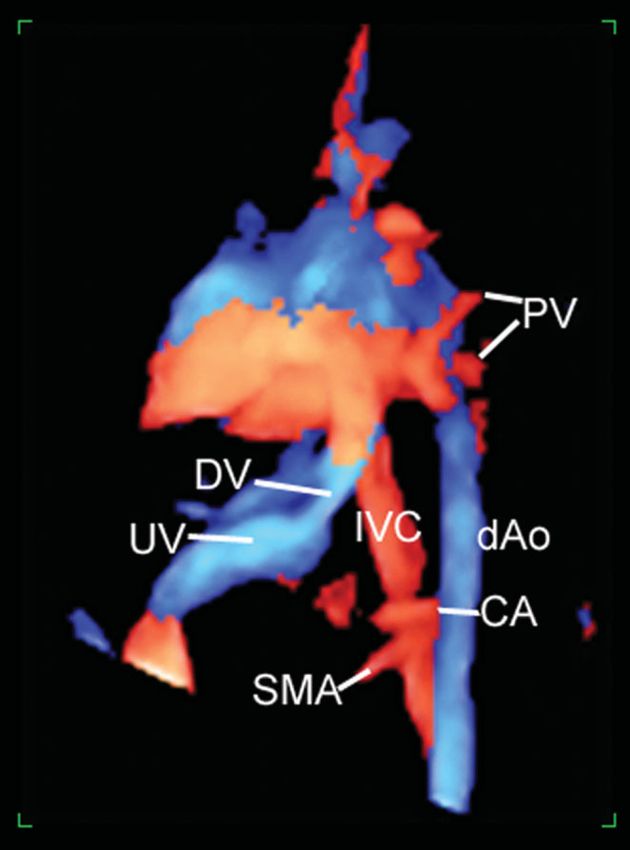
84 Yagel et al.
V
IV
T DA
SVC
AO
PA
III
II
I
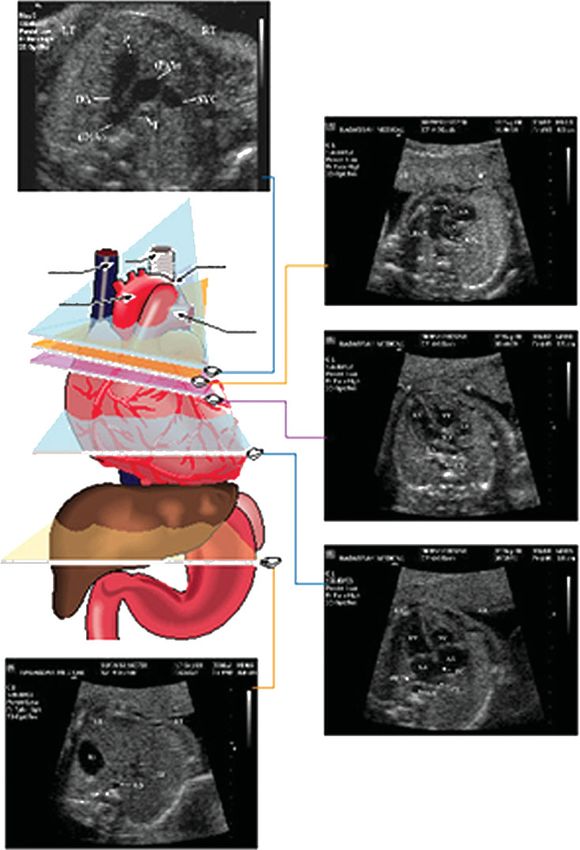
Figure 3 Diagrammatic representation and ultrasound images showing the five planes of fetal echocardiography (reprinted with permission,
from Ultrasound Obstet Gynecol 2001; 17: 367–369). AO, aorta; DA, ductus arteriosus; PA, pulmonary artery; SVC, superior vena cava;
T, trachea.
of all three planes. By moving the point the operator By comparing the A- and B-frames of the MPR
manipulates the volume to display any plane within the display, the operator can view complex cardiac anatomy
volume; if temporal information was acquired, the same in corresponding transverse and longitudinal planes
plane can be displayed at any stage of the scanned cycle. simultaneously. So, for example, an anomalous vessel
From a good STIC acquisition5 the operator can scroll that might be disregarded in cross-section is confirmed in
through the acquired volume to obtain sequentially each the longitudinal plane.
of the classic five planes6 of fetal echocardiography, and 3D rendering is another analysis capability of an
any plane may be viewed at any time-point throughout acquired volume. It is familiar from static 3D applications,
the reconstructed cardiac cycle loop. The cycle can be such as imaging the fetal face in surface rendering mode.
run or stopped frame-by-frame to allow examination of In fetal echocardiography it is readily applied to 4D
all phases of the cardiac cycle, for example opening and scanning. The operator places a bounding box around
closing of the atrioventricular valves. the region of interest within the volume (after arriving
Copyright 2007 ISUOG. Published by John Wiley & Sons, Ltd. Ultrasound Obstet Gynecol 2007; 29: 81–95.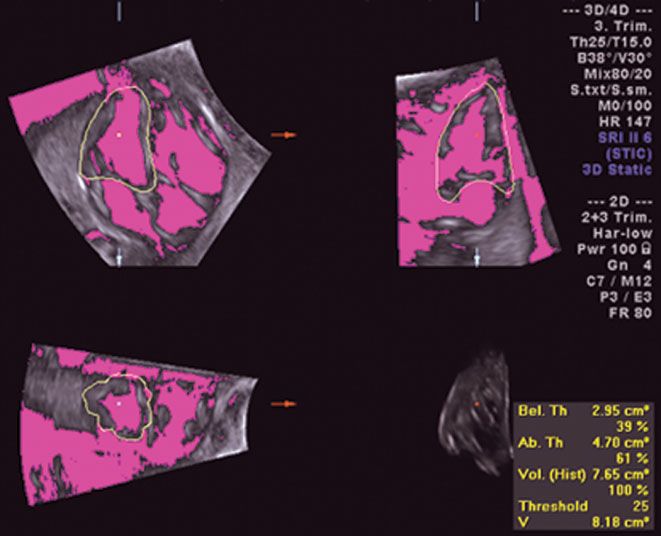
Ultrasound in fetal cardiac scanning 85
at the desired plane and time) to show a slice of the scanning to obtain a 3D volume file with color Doppler
volume whose depth reflects the thickness of the slice. information or 3DPD (one-color) volume files.
For example, with the A-frame showing a good four- Color Doppler can be used more effectively in 3D/4D
chamber view, the operator places the bounding box ultrasonography when combined with STIC acquisition12
tightly around the interventricular septum. The rendered in fetal echocardiography, resulting in a volume file that
image in the D-frame will show an ‘en face’ view of the reconstructs the cardiac cycle, as above, with color flow
septum. The operator can determine whether the plane information. This joins the Doppler flow to cardiac
will be displayed from the left or right, i.e. the septum events2 and provides all the advantages of analysis
from within the left or the right ventricle; the thickness of (MPR, rendering, TUI) with color. This combination
the slice will determine the depth of the final image, for of modalities is very sensitive for detecting intracardiac
example to show texture of the trabeculations within the Doppler flow through the cardiac cycle, for example mild
right ventricle (Figure 4). tricuspid regurgitation that occurs very early in systole or
TUI is a more recent application that extends the very briefly can be clearly seen13 .
capabilities of MPR and rendering modes. This multislice Extreme care must be taken when working with
analysis mode resembles a magnetic resonance imaging Doppler applications in post-processing, however, to
or computer-assisted tomography display. Nine parallel avoid misinterpretation of flow direction as the volume is
slices are displayed simultaneously from the plane of rotated.
interest (the ‘zero’ plane), giving sequential views from 3DPD is directionless, one-color Doppler that is most
−4 to + 4. The thickness of the slices, i.e. the distance effectively joined with static 3D scanning2 . 3DPD uses
between one plane and the next, can be adjusted by the Doppler shift technology to reconstruct the blood vessels
operator. The upper left frame of the display shows the in the VOI, isolated from the rest of the volume. Using
position of each plane within the region of interest, relative the ‘glass body’ mode in post-processing, surrounding
to the reference plane. This application has the advantage tissue is eliminated and the vascular portion of the scan
of displaying sequential parallel planes simultaneously, is available in its entirety for evaluation. The operator
giving a more complete picture of the fetal heart (Figure 5). can scroll spatially to any plane in the volume (but not
temporally: in this case, color Doppler with STIC is more
3D/4D with color Doppler, 3D power Doppler (3DPD) effective, see above). 3DPD can reconstruct the vascular
and 3D high definition power flow Doppler tree of the fetal abdomen and thorax14,15 , relieving the
operator of the necessity of reconstructing a mental picture
Color and power Doppler have been extensively applied of the idiosyncratic course of an anomalous vessel from
to fetal echocardiography; one could hardly imagine a series of 2D planes. This has been shown to aid our
performing a complete fetal echo scan today without understanding of the normal and anomalous anatomy and
color Doppler. Color or power Doppler, and the most pathophysiology of vascular lesions16 (Figure 6).
recent development, high-definition flow Doppler, can High-definition power flow Doppler, the newest
be combined with static 3D direct volume non-gated development in color Doppler applications, uses high
Figure 4 Ultrasound images showing normal interventricular septum in three-dimensional rendering mode. In frame A the bounding box is
placed tightly around the septum with the active side (green line) on the right (a). The D-frame shows the septum ‘en face’: note the rough
appearance of the septum from within the trabeculated right ventricle (b). lt, left; rt, right.
Copyright 2007 ISUOG. Published by John Wiley & Sons, Ltd. Ultrasound Obstet Gynecol 2007; 29: 81–95.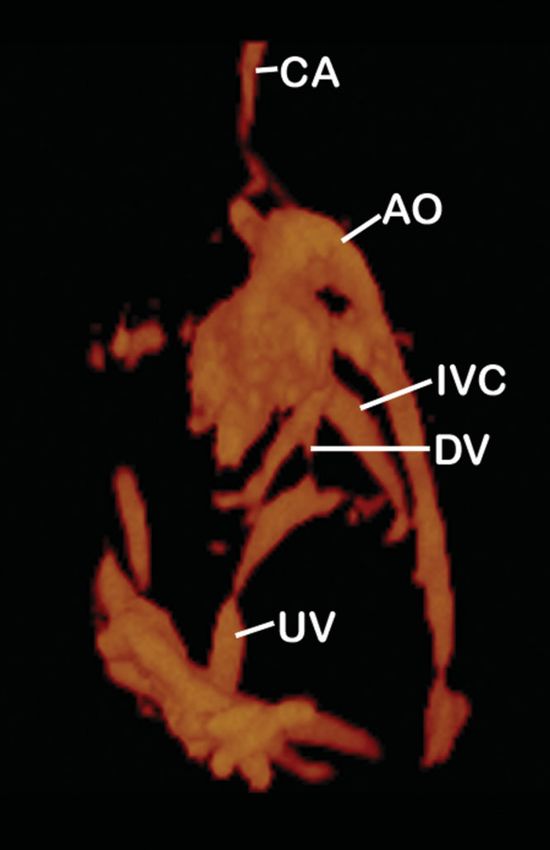
86 Yagel et al.
Figure 5 Tomographic ultrasound imaging: The −4 plane (top row, center) shows the four-chamber view while the zero plane (asterisk,
middle row, right) shows the outflow tracts view and the + 3 plane shows the great vessels (bottom, right).
resolution and a small sample volume to produce fluid-filled areas (black) in a volume and inverts their
images with two-color directional information with less presentation, i.e. fluid-filled spaces such as the cardiac
‘blooming’ of color for more realistic representation of chambers now appear white, while the myocardium has
vessel size. It depicts flow at a lower velocity than does disappeared. In fetal echocardiography it can be applied to
color or power Doppler, and has the advantage of showing create ‘digital casts’ of the cardiac chambers and vessels19 .
flow direction. It can be combined with static 3D or 4D It can also produce a reconstruction of the extracardiac
gated acquisition (STIC) and the glass-body mode, to vascular tree, similar to 3DPD. IM has the additional
produce high-resolution images of the vascular tree with advantage of showing the stomach and gall bladder as
bidirectional color coding (Figure 7). This technique is white structures, which can aid the operator in navigating
particularly sensitive for imaging small vessels. High- within a complex anomaly scan. Most recently, IM has
resolution bidirectional power flow Doppler combines been joined with STIC to quantify fetal cardiac ventricular
the flow information provided by color Doppler with the volumes, which may prove useful in the evaluation of fetal
anatomic acuity associated with power Doppler. Owing heart function.
to this modality’s sensitivity systolic and diastolic flow are
observed at the same time, for example, when used with
STIC acquisition the ductus venosus is shown to remain B-flow
filled both in systole and in diastole.
B-flow is an ‘old-new’ technology that images blood flow
without relying on Doppler shift. B-flow is an outgrowth
Inversion mode (IM) of B-mode imaging that, with the advent of faster frame
rates and computer processing, allows the direct depiction
IM is another post-processing visualization modality that of blood cell reflectors. It avoids some of the pitfalls of
can be combined with static 3D or STIC acquisition17,18 . Doppler flow studies, such as aliasing and signal drop-
IM analyzes the echogenicity of tissue (white) and out at orthogonal scanning angles. The resulting image
Copyright 2007 ISUOG. Published by John Wiley & Sons, Ltd. Ultrasound Obstet Gynecol 2007; 29: 81–95.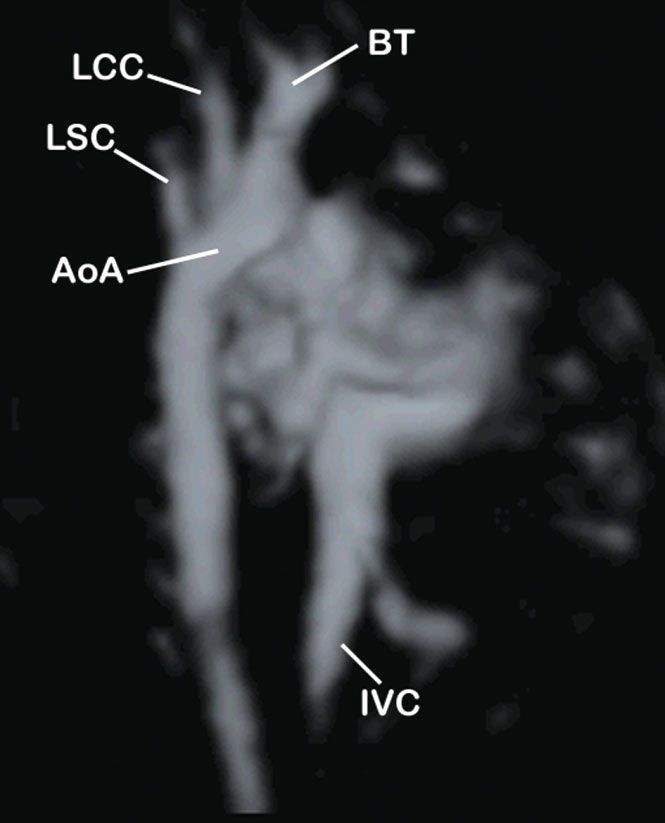
Ultrasound in fetal cardiac scanning 87
Figure 7 Spatio-temporal image correlation acquisition with high
definition power flow Doppler of the normal heart and great
vessels. CA, celiac artery; dAo, descending aorta; DV, ductus
venosus; IVC, inferior vena cava; PV, pulmonary veins; SMA,
superior mesenteric artery; UV, umbilical vein.
Figure 6 Three-dimensional power Doppler image of the heart and
major vessels. AO, aorta; CA, carotid artery; DV, ductus venosus;
IVC, inferior vena cava; UV, umbilical vein. STIC acquisition to fetal echocardiography, and various
techniques have been put forward to optimize the use of
is a live gray-scale depiction of blood flow and part of this modality.
the surrounding lumen, creating sensitive ‘digital casts’ of A well-executed STIC acquisition5 contains all the
blood vessels and cardiac chambers (Figure 8). This also necessary planes for evaluation of the five classic
makes B-flow more sensitive for volume measurement. transverse planes of fetal echocardiography6,7 . The
When applied to 3D fetal echocardiography B-flow operator can examine the fetal upper abdomen and
modality is a direct volume non-gated scanning method stomach, then scroll cephalad to obtain the familiar four-
able to show blood flow in the heart and great vessels in chamber view, the five-chamber view, the bifurcation of
real-time, without color Doppler flow information20 . the pulmonary arteries, and finally the three-vessel and
trachea view. Slight adjustment along the x- or y-axis may
be necessary to optimize the images. Performed properly,
S C R E E N I N G EX A M I N A T I O N O F T H E this methodology will provide the examiner with all the
FETAL HEART WITH 3D/4D necessary planes to conform with the guidelines. However,
ULTRASOUND it must be remembered that STIC acquisition that has been
degraded by maternal or fetal movements, including fetal
Guidelines breathing movements, will contain artifacts within the
scan volume.
Guidelines for the performance of fetal heart examina-
tions have been published by the Internatinal Society
of Ultrasound in Obstetrics and Gynecology (ISUOG)21 . Applications
These guidelines for ‘basic’ and ‘extended basic’ fetal car-
diac scanning are amenable to 3D/4D applications, and Among the most attractive facets of 3D/4D scanning is the
3D/4D can enhance both basic and extended basic fetal potential for digital archiving and sharing of examination
cardiac scans, as well as evaluation of congenital anoma- data over a network. These capabilities were applied
lies. Many research teams have applied 3D ultrasound and by Vinals et al. to increase delivery of prenatal cardiac
Copyright 2007 ISUOG. Published by John Wiley & Sons, Ltd. Ultrasound Obstet Gynecol 2007; 29: 81–95.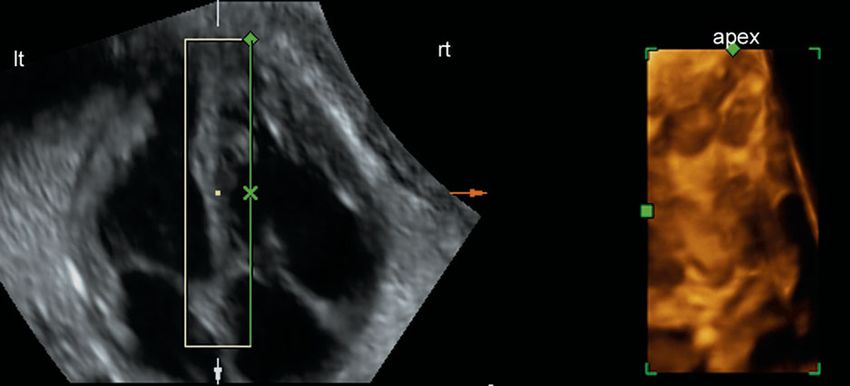
88 Yagel et al.
are in constant anatomic relationship to this plane, and a
computer-automated program could present those planes
once the appropriate volume block had been acquired9 .
Most recently, Espinoza et al. introduced a novel
algorithm combining STIC and TUI10 to image the
diagnostic planes of the fetal heart simultaneously, and
facilitate visualization of the long-axis view of the aortic
arch. However, it must be stressed again that for any
post-processing technique, if the original volume was sub-
optimal, subsequent analysis will be prone to lower image
quality and the introduction of artifacts.
Nuchal translucency screening programs will refer
approximately 3–5% of patients who are deemed to
be high risk for fetal echocardiography24,25 , increasing
demand for early targeted fetal heart scans. STIC
acquisition is amenable to younger gestational ages, as the
smaller fetal heart can be scanned in a shorter acquisition
time, thus reducing the chance of acquisition degradation
from fetal movements.
Functional evaluation of the fetal heart: ventricular
volumetry
The evaluation of fetal heart functional parameters has
long challenged fetal echocardiographers. While duplex
and color Doppler flow nomograms have been quantified
Figure 8 B-flow image of the normal heart and aortic arch, and are long-established in 2D fetal echocardiography,
showing the brachiocephalic trunk (BT), with the left common
carotid (LCC) and left subclavian (LSC) arteries seen projecting
many of the pediatric and adult measures are based on
from the aortic arch (AoA). IVC, inferior vena cava. end-systolic and end-diastolic ventricular volumes: stroke
volume, ejection fraction, and cardiac output. Without
electrical trace or clinically applicable segmentation
scanning to poorly-served areas. Local practitioners methods to determine the ventricular volume, these
in distant areas acquired and stored 3D volume sets parameters have eluded practical prenatal quantification.
at their centers; they were subsequently sent over an 3D ultrasound opens new avenues for exploration into
internet link and analyzed by expert examiners in central ventricular volumetry26,27 and mass measurement.
locations22,23 . This can have important implications in Bhat et al. used non-gated static 3D acquisition and
increasing penetration of prenatal ultrasound services in STIC to obtain mid-diastolic scans of fetal hearts and
poorly-served or outlying areas of many countries. applied virtual organ computer-aided (VOCAL) analysis
DeVore et al. presented the ‘spin’ technique8 combining to determine cavity volume. The result was multiplied by
MPR and STIC acquisition to analyze acquired volumes myocardial density (1.050 g/cm3 ) to obtain the mass28,29 .
and simplify demonstration of the ventricular outflow We recently presented30 a methodology that combines
tracts. Using this technique the operator acquires a VOI STIC acquisition with IM to determine the end-systolic
from a transverse sweep of the fetal mediastinum that and end-diastolic stages in the cardiac cycle, then applied
includes the sequential planes of fetal echocardiography. inversion mode to isolate the fluid-filled ventricular
In post-processing the outflow tracts view is imaged in the volume, which was measured using VOCAL analysis
A-plane, and outflow tracts and adjacent vessels are then (Figure 9). The resulting volumes allowed quantification
examined by placing the reference point over each vessel of stroke volume and ejection fraction30 . It was found that
and rotating the image along the x- and y-axes until the both the inversion mode and VOCAL analysis were highly
full length of each vessel has been identified8 . dependent on operator-determined threshold parameters,
Abuhamad proposed an automated approach to which affect the intensity of signal to be colored and
extracting the required planes from an acquired volume, included in the volumetry. A similar study of cardiac
coining the term ‘automated multiplanar imaging’ or mass is under way.
AMI9 . Based on the idea that the scanned 3D volume
contains all possible planes of the scanned organ, it 3D/4D ULTRASOUND IN THE DIAGNOSIS
should be possible to define the geometric planes within OF CONGENITAL HEART DISEASE
that volume that would be required to display each
of the diagnostic planes of a given organ, for example One of the great advantages of 3D/4D systems is digital
the sequential scanning planes of fetal echocardiography. storage capabilities, which allow the operator to store
Beginning with the four-chamber view, all the other planes examination volumes for later analysis, away from the
Copyright 2007 ISUOG. Published by John Wiley & Sons, Ltd. Ultrasound Obstet Gynecol 2007; 29: 81–95.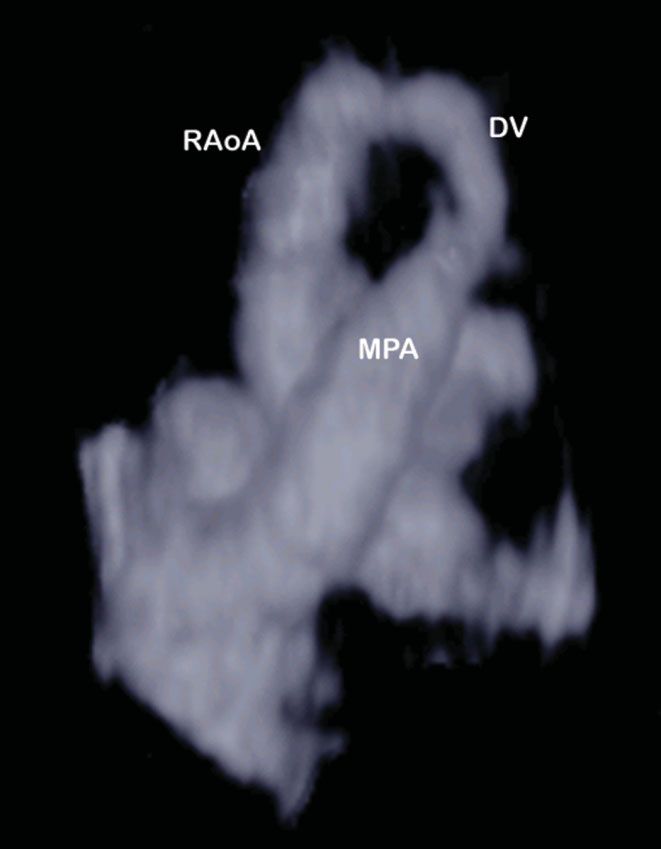
Ultrasound in fetal cardiac scanning 89
Segmental approach
The segmental approach to CHD has helped to
standardize the description of cardiac lesions. In
addition, it has contributed to an understanding of
the pathophysiology of the malformed developing fetal
heart, and subsequently to our conceptualization and
diagnostic imaging. The sequential segmental approach
essentially divides the heart into three basic segments:
the atria, the ventricles, and the great arteries. These are
divided and joined at the level of the atrioventricular
valves, and at the ventriculo-arterial junctions. The
segmental approach to the diagnosis of CHD is
comprehensively and concisely described elsewhere31 ; we
will follow this sequence in describing the application
and added value of 3D/4D in the diagnosis of CHD,
through index cases of anomalies diagnosed in our
Figure 9 Spatio-temporal image correlation acquisition combined center.
with inversion mode and virtual organ computer-aided analysis for
fetal cardiac ventricle volumetry. The resulting measurements
appear in the box, bottom right. Veins and atria: total anomalous pulmonary venous
connection and interrupted inferior vena cava with
azygos continuation
patient and time constraints of a busy clinic. Nowhere
Total anomalous pulmonary venous connection (TAPVC)
is this advantage so appreciated as in cases of congenital
is a many-faceted group of malformations affecting the
heart disease (CHD). Other professionals can be invited
pulmonary veins; the variations and classification are
to view the examination; they might be anywhere where
described in detail elsewhere32 . Essentially, in these
an internet link is available. This allows the first examiner
anomalies the pulmonary veins do not drain into the
the chance to consult with the attending physician,
left atrium but rather to various other locations: the
cardiologist, surgical or other management teams, genetic
right atrium, great veins or abdominal veins. We describe
counselors and parents. Complex malformations can be
a case of intradiaphragmatic TAPVC with drainage
elucidated for interdisciplinary discussion and for laymen.
of the pulmonary veins to the portal vein. Figure 10a
In addition, stored data from cases of CHD are invaluable
shows the use of MPR with the reference point to
teaching materials for professional education.
navigate this complex lesion. Placement of the reference
Many teams have applied 3D/4D ultrasound capa-
point in the suspected anomalous blood vessel in cross-
bilities to the diagnosis of congenital cardiovascular
section (A-frame) showed the vessel in longitudinal plane
malformations. Each of the modalities and applications
in the B-frame. This confirmed that the finding was
described above lends itself to different facets of this
not an artifact, rather the characteristic vertical vein.
complex endeavor.
3D power flow Doppler displayed the idiosyncratic
vascular tree and absence of the pulmonary veins
(Figure 10b); rotation of the image in post-processing
Virtual planes allowed overall examination of the lesion through
360◦ .
As described above, a properly executed STIC acquisition Interrupted inferior vena cava (IVC) with azygos
results in a volume ‘block’, reconstructed to reflect a continuation is shown in Figure 11. This cardinal vein
complete cardiac cycle. When this block of spatial and anomaly results from primary failure of the right
temporal image data is analyzed in post-processing, the subcardinal vein to connect to the hepatic segment
operator can access and display any plane at any time- of the IVC32 . Blood is shunted directly into the right
point in the cardiac cycle. Many of these planes are supracardinal vein (which will become the superior vena
not readily accessible in 2D ultrasound; the term ‘virtual cava (SVC)); blood from the lower body flows through the
planes’ was coined to refer to these rendered scanning azygos vein to the SVC. In this instance, B-flow acquisition
planes. The interventricular and interatrial septa (IVS, provided real-time representation of the anomalous course
IAS) planes, and the coronal atrioventricular (CAV) plane of the IVC and connection to the fetal heart. It showed
of the cardiac valves’ annuli, have been investigated the azygos vein draining into the SVC, as well as the
and applied to the evaluation of CHD11 . They were aorta, in one three-dimensional image that would be
shown to have added value in the diagnosis of ventricular impossible to obtain with 2D color Doppler scanning.
septal defect, restrictive foramen ovale, alignment of the B-flow scanning provided superior imaging of the slower
ventricles and great vessels, and evaluation of the AV blood flow in the azygos vein than was demonstrated with
valves. 3DPD.
Copyright 2007 ISUOG. Published by John Wiley & Sons, Ltd. Ultrasound Obstet Gynecol 2007; 29: 81–95.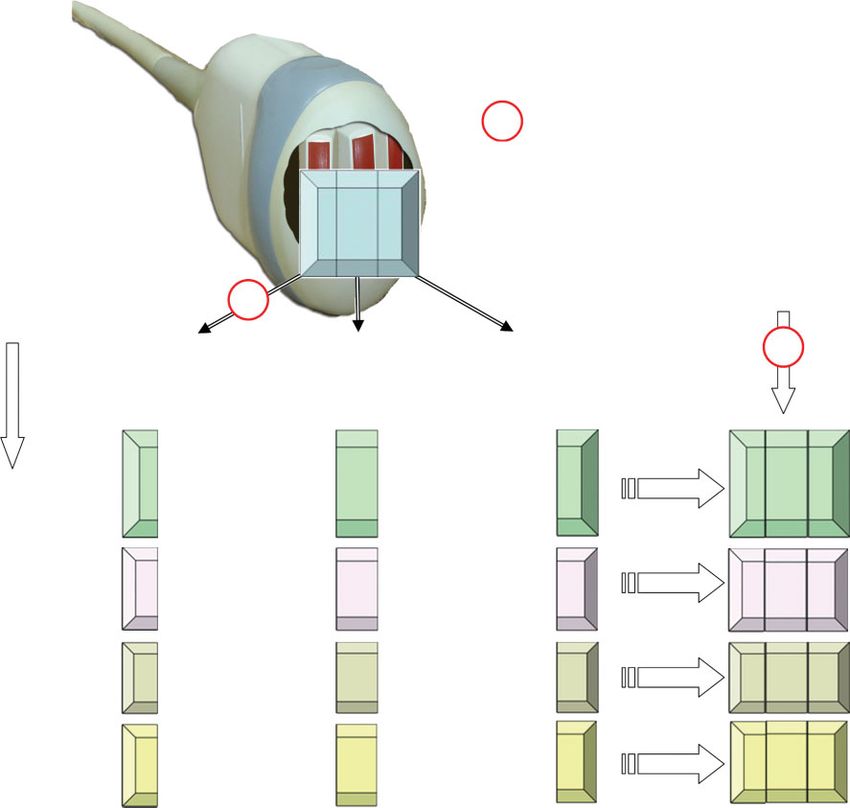
90 Yagel et al.
Figure 11 B-flow ultrasound image of the heart and great vessels in
a fetus with interrupted inferior vena cava with azygos
continuation. AoA, aortic arch; AzV, azygos vein; DV, ductus
venosus; SVC, superior vena cava.
Figure 10 (a) Spatio-temporal image correlation (STIC) acquisition
in a case of total anomalous pulmonary venous connection. The
A-plane showed raised suspicion of an anomalous vessel (caret),
which is confirmed in the B-plane (arrow). (b) The heart and great
vessels of this fetus: STIC acquisition and high definition power
flow Doppler confirmed the characteristic vertical vein (VV). Note
also the absence of pulmonary veins (compare with Figure 7). dAo,
descending aorta; IVC, inferior vena cava.
Atrioventricular (AV) junction: atrioventricular septal
defect (AVSD) and tricuspid valve stenosis
AVSD is characterized by incomplete atrial and ven-
tricular septation, forming a common atrioventricular
junction. AVSD has many forms, all of which involve an
abnormality of the AV valves. Figure 12 shows the use
of 3D rendering of a STIC volume acquired with color
Doppler to demonstrate the anomalous intracardiac flow
resulting from the AVSD.
Another group of AV valve lesions is mitral or tricuspid
valve atresia, dysplasia, or stenosis. Figure 13 shows the
CAV plane in a case of tricuspid stenosis. This ‘virtual
plane’ is obtained from a STIC volume with color Doppler,
by placing the bounding box with the superior side active Figure 12 Ultrasound image of the coronal atrioventricular plane
tightly around the level of the AV connection in the four- from spatio-temporal image correlation acquisition with color
chamber view (Frame A); the plane is slightly adjusted Doppler mapping in a case of atrioventricular septal defect (AVSD).
AO, aorta; lt, left; PA, pulmonary artery; rt, right.
along the x- and y-axes and the rendered image (Frame D)
shows the AV valves with anomalous anatomy (compare
normal CAV plane, inset). This virtual plane provides a Ventricles: ventricular septal defects (VSDs)
three-dimensional look at the AV and semilunar valves’
annuli, resembling the surgical plane seen when the heart Ventricular septal defects are perhaps the most
is opened in surgery. common – and most commonly missed – congenital heart
Copyright 2007 ISUOG. Published by John Wiley & Sons, Ltd. Ultrasound Obstet Gynecol 2007; 29: 81–95.Ultrasound in fetal cardiac scanning 91
Figure 13 Tricuspid stenosis evaluated with three-dimensional rendering and the coronal atrioventricular (CAV) plane. The bounding box is
placed tightly around the level of the atrioventricular valves in the A-frame (a); the D frame (b) clearly shows the stenotic valve (arrow).
Compare normal CAV plane in diastole, inset. ao, aortic valve; mv, mitral valve annulus; pa, pulmonary valve; tv, tricuspid valve annulus.
defect. The natural history and in-utero development of Ventriculo-arterial junctions (conotruncal anomalies):
these lesions have been described elsewhere33 . Several transposition of the great arteries and tetralogy of Fallot
groups have proposed methods for evaluating the inter-
ventricular septum34,35 . By using MPR, with the reference Transposition (or malposition or malalignment) of the
point placed on the septum with the four chamber view in great arteries (TGA) is the general name for a complex
the A-frame, the B-frame will show the septum and defect group of anomalies with widely varying anatomic and
‘en face’ (Figure 14). We recommend however the use of clinical presentations. When the sequential segmental
the bounding box in 3D rendering from STIC acquisition approach is applied to systematic diagnosis of CHD31 ,
with color Doppler. This method has the advantage of the morphology of each successive anatomic segment is
allowing the operator to place the ‘active’ side of the box assessed in turn. The morphologic right and left atria and
to the right or left (i.e. from within the left or right ven- ventricles are established; now the examiner addresses
tricle) and of giving the resulting image (in the D-frame) the ventriculo-arterial junction and the accordance or
depth, for a more detailed examination of the size and discordance of the great arteries and ventricles.
nature (and number) of the VSD(s). The addition of color 3D rendering with color Doppler has been applied to
Doppler will demonstrate blood flow across the lesion the evaluation of suspected malalignment of the great
and show at what stage in the cardiac cycle and to what vessels, by examining the CAV (‘surgical plane’) at the
degree the shunting occurs. level of the AV and semilunar valves’ annuli.
We applied B-flow scanning to the evaluation of TGA
and found that it was more effective than 3DPD or
inversion mode in visualizing the great vessels’ structure
and relationships. Figure 15 shows a case of complete d-
transposition of the great arteries. The B-flow scan clearly
showed blood flow into the ventricles and out through the
malaligned vessels, demonstrating the anatomic variant
of the anomaly and assisting our consultations with the
parents and their attending physician.
Arterial trunks: pulmonary stenosis and right aortic
arch
The use of 3D rendering of a STIC acquisition with or
without color Doppler to obtain virtual planes is discussed
above. The CAV plane is an excellent tool for the evalua-
tion of the semilunar valves. Once the CAV plane has been
Figure 14 The interventricular septum (IVS) ‘virtual plane’ with obtained, the 4D-cine option can be initiated to evaluate
color Doppler in the evaluation of ventricular septal defect. The
navigation point is placed on the septum in the A-plane (a); the blood flow across the valves through the cardiac cycle.
D-frame (b) shows the rendered IVS with flow across the defect Figure 16 shows a case of critical pulmonary stenosis with
from right to left. retrograde flow in the main pulmonary artery (MPA).
Copyright 2007 ISUOG. Published by John Wiley & Sons, Ltd. Ultrasound Obstet Gynecol 2007; 29: 81–95.92 Yagel et al.
Figure 15 B-flow ultrasound scan showing the parallel great vessels
in a case of transposition of the great vessels. Application of this
modality clearly shows the blood flow in the malaligned vessels.
AO, aorta; lt, left; PA, pulmonary artery; rt, right.
Figure 17 B-flow ultrasound scan in a case of right aortic arch
(RAoA). DV, ductus venosus; MPA, main pulmonary artery.
Functional evaluation: ventricular volumes
We recently presented30 a novel methodology that com-
bined STIC acquisition with post-processing application
of the inversion mode to quantify end-systolic and end-
diastolic ventricular volumes. We examined 100 fetuses
of 20–40 weeks’ gestation, and created nomograms of
right and left ventricle end-systolic and end-diastolic vol-
umes. The resulting measurements correlated strongly
with gestational age and estimated fetal weight. From
these volumes we were able to create nomograms for fetal
stroke volume and cardiac ejection fraction.
During the study period we applied this methodology
to saved STIC volumes of cases presenting with
cardiac anomaly or dysfunction that showed changes in
Figure 16 The coronal atrioventricular plane from spatio-temporal ventricular volume, stroke volume, or ejection fraction.
image correlation acquisition with color Doppler mapping in a case These included critical pulmonary stenosis, twin-to-
of transposition of the great arteries and pulmonary stenosis with twin transfusion syndrome with secondary pulmonary
retrograde flow in the main pulmonary artery. AO, aorta; lt, left;
M, mitral annulus; PA, pulmonary artery; rt, right; T, tricuspid
stenosis, aortic valve stenosis with hypoplastic aortic arch,
annulus. Ebstein’s anomaly, supraventricular tachycardia (SVT),
and vein of Galen aneurysm.
Our normal cases showed the effectiveness of fetal
Right aortic arch is a defect resulting from persistence heart ventricular volumetry in cardiac evaluation and
of the right dorsal aorta and involution of the distal part quantification; such volumetry is not readily available in
of the left dorsal aorta. There are two main types, with or 2D echocardiography. The pathological cases showed the
without a retroesophageal component36 . Figure 17 shows potential added value of this methodology. In the case
a case of right aortic arch diagnosed with B-flow imaging; of critical pulmonary stenosis, for example, the diagnosis
this modality showed the idiosyncratic course of the aortic was more serious than suspected by 2D echocardiography.
arch to the right of the trachea. Ventricular volumetry also provided insight into the
Copyright 2007 ISUOG. Published by John Wiley & Sons, Ltd. Ultrasound Obstet Gynecol 2007; 29: 81–95.Ultrasound in fetal cardiac scanning 93
pathophysiology of lesions such as SVT and vein of Galen plane, acoustic shadows may not be apparent. However,
aneurysm, among others30 . they may be present within the acquired volume block. It
is imperative to review suspected defects with repeated 2D
POTENTIAL PITFALLS OF 3D/4D and 3D scanning to confirm their presence in additional
ECHOCARDIOGRAPHY scanning planes.
3D/4D fetal echocardiography scanning is prone to arti-
3D rendering
facts similar to those encountered in 2D ultrasonography,
and some that are specific to 3D/4D acquisition and 3D rendering creates virtual images. It must be
post-processing. remembered that application of some algorithms designed
to smooth the image can lead to loss of data from the
STIC acquisition quality original scan. 3D rendering should always be used in
conjunction with the A-frame 2D image for comparison.
The quality of a STIC acquisition may be adversely
affected by fetal body or ‘breathing’ movements; quality is
Flow direction
improved by scanning with the fetus in a quiet state, and
using the shortest scan time possible. When reviewing An acquired volume containing Doppler flow information
a STIC acquisition, the B-frame will reveal artifacts is available for manipulation and may be sliced and
introduced by fetal breathing movements (Figure 18). rotated around the x-, y-, and z-axes for analysis.
If the B-frame appears sound, the volume is usually However, rotation of the volume with Doppler directional
acceptable, and can be used for further investigation. flow information can mislead the operator: if the
It must be stressed again that the quality of the original directions are reversed, flow data can be misinterpreted.
acquisition will affect all further stages of post-processing The operator must confirm any suspected pathological
and evaluation. flow patterns by confirming the original direction of
scanning, whether flow was toward or away from the
Original angle of insonation transducer during the acquisition scan.
The original angle at which a scan was performed will
impact on the quality of all the planes acquired. It is ACCURACY
important to achieve an optimal beginning 2D plane Several studies have compared imaging yield between 2D
before starting 3D or 4D acquisition. and 3D/4D fetal echocardiography, others have examined
the feasibility of 3D/4D and STIC in screening programs,
Acoustic shadows while others have described the application of various
3D/4D modalities to the diagnosis or evaluation of fetal
Shadowing artifacts pose a particular problem for 3D/4D cardiovascular anomalies. However, no large study has
ultrasound. When commencing scanning from the 2D examined the contribution of 3D/4D ultrasonography to
the accuracy of fetal echocardiography screening pro-
grams.
Levental et al. compared 2D and non-gated 3D
ultrasound to obtain standard cardiac views37 . Meyer-
Wittkopf et al.38 evaluated 2D and Doppler-gated 3D
ultrasound in obtaining standard echocardiography scan-
ning planes in normal hearts. They found that 3D ultra-
sound provided additional structural depth and allowed
a dynamic 3D perspective of valvar morphology and
ventricular wall motion38 .
In evaluating CHD, Meyer-Wittkopf et al.39 evaluated
gated 3D volume sets of 2D-diagnosed cardiac lesions,
and compared key views of the heart in both modalities.
They determined that 3D had added value in a small
proportion of lesions39 . Wang et al.40 compared 3D and
2D scanning of fetuses in the spine-anterior position. This
group found that only in the pulmonary outflow tract was
3D ultrasound superior to 2D.
Espinoza et al.18 examined the added value of IM in the
evaluation of anomalous venous connections. The inves-
Figure 18 Spatio-temporal image correlation acquisition in a fetus
of 26 weeks’ gestation. The A-frame shows the left ventricular tigators found that IM improved visualization of cases
outflow tract plane. Note that the B-frame, however, is degraded by of dilated azygos or hemiazygos veins and their spatial
fetal breathing artifacts (arrows). relationships with the surrounding vascular structures.
Copyright 2007 ISUOG. Published by John Wiley & Sons, Ltd. Ultrasound Obstet Gynecol 2007; 29: 81–95.94 Yagel et al.
Most recently, Benacerraf et al.41 compared acquisition tracts using three-dimensional ultrasound. Ultrasound Obstet
and analysis times for 2D and 3D fetal anatomy scanning Gynecol 2004; 24: 72–82.
9. Abuhamad A. Automated multiplanar imaging: a novel
at 17–21 weeks’ gestation. 3D ultrasound compared approach to ultrasonography. J Ultrasound Med 2004; 23:
favorably with 2D in mean scanning time and accuracy 573–576.
of fetal biometry. 10. Espinoza J, Kusanovic JP, Goncalves LF, Nien JK, Hassan S,
The data archiving and networking capabilities of Lee W, Romero R. A novel algorithm for comprehensive fetal
3D/4D fetal echocardiography with STIC acquisition open echocardiography using 4-dimensional ultrasonography and
tomographic imaging. J Ultrasound Med 2006; 25: 947–956.
up new avenues for disseminating fetal echocardiography
11. Yagel S, Benachi A, Bonnet D, Dumez Y, Hochner-Celnikier D,
programs to distant or poorly served areas. This can have Cohen SM, Valsky DV, Fermont L. Rendering in fetal cardiac
important public health implications in these populations. scanning: the intracardiac septa and the coronal atrioventricular
Michailidis et al.42 and Vinals et al.22,23 have shown the valve planes. Ultrasound Obstet Gynecol 2006; 28: 266–274.
feasibility and success of programs based on 3D/4D exam 12. Goncalves LF, Romero R, Espinoza J, Lee W, Treadwell M,
Chintala K, Brandl H, Chaiworapongsa T. Four-dimensional
volumes acquired in one center, and reviewed by experts
ultrasonography of the fetal heart using color Doppler
in a center connected by internet link. spatiotemporal image correlation. J Ultrasound Med 2004; 23:
473–481.
13. Messing B, Porat S, Imbar T, Valsky DV, Anteby EY, Yagel S.
CONCLUSIONS Mild tricuspid regurgitation: a benign fetal finding at various
stages of pregnancy. Ultrasound Obstet Gynecol 2005; 26:
In coming years, studies will direct 3D/4D capabilities 606–609.
to the evaluation of fetal cardiac functional parameters. 14. Chaoui R, Kalache KD, Hartung J. Application of three-
This may provide insights into the physiological effects of dimensional power Doppler ultrasound in prenatal diagnosis.
Ultrasound Obstet Gynecol 2001; 17: 22–29.
fetal structural or functional cardiac defects, or maternal
15. Chaoui R, Hoffmann J, Heling KS. Three-dimensional (3D) and
diseases such as diabetes, on the developing fetus. 4D color Doppler fetal echocardiography using spatio-temporal
To the best of our knowledge, no large study image correlation (STIC). Ultrasound Obstet Gynecol 2004;
has been performed to date to examine whether the 23: 535–545.
addition of 3D/4D methods to fetal echocardiography 16. Sciaky-Tamir Y, Cohen SM, Hochner-Celnikier D, Valsky DV,
screening programs increases the detection rate of cardiac Messing B, Yagel S. Three-dimensional power Doppler (3DPD)
ultrasound in the diagnosis and follow-up of fetal vascular
defects. This technology has reached the stage when its anomalies. Am J Obstet Gynecol 2006; 194: 274–281.
reproducibility and added value in screening accuracy 17. Goncalves LF, Espinoza J, Lee W, Mazor M, Romero R. Three-
should be tested in large prospective studies, not only by and four-dimensional reconstruction of the aortic and ductal
teams or in centers that have made 3D/4D their specialty, arches using inversion mode: a new rendering algorithm for
but among the generality of professionals performing fetal visualization of fluid-filled anatomical structures. Ultrasound
Obstet Gynecol 2004; 24: 696–698.
echocardiography.
18. Espinoza J, Goncalves LF, Lee W, Mazor M, Romero R.
A novel method to improve prenatal diagnosis of abnormal
systemic venous connections using three- and four-dimensional
REFERENCES ultrasonography and ‘inversion mode’. Ultrasound Obstet
1. DeVore GR, Falkensammer P, Sklansky MS, Platt LD. Spatio- Gynecol 2005; 25: 428–434.
temporal image correlation (STIC): new technology for 19. Goncalves LF, Espinoza J, Lee W, Nien JK, Hong JS, Santolaya-
evaluation of the fetal heart. Ultrasound Obstet Gynecol 2003; Forgas J, Mazor M, Romero R. A new approach to fetal
22: 380–387. echocardiography: digital casts of the fetal cardiac chambers
2. Deng J. Terminology of three-dimensional and four-dimen- and great vessels for detection of congenital heart disease.
sional ultrasound imaging of the fetal heart and other moving J Ultrasound Med 2005; 24: 415–424.
body parts. Ultrasound Obstet Gynecol 2003; 22: 336–344. 20. Volpe P, Campobasso G, Stanziano A, De Robertis V, Di
3. Goncalves LF, Lee W, Chaiworapongsa T, Espinoza J, Paolo S, Caruso G, Volpe N, Gentile M. Novel application
Schoen ML, Falkensammer P, Treadwell M, Romero R. Four- of 4D sonography with B-flow imaging and spatio-temporal
dimensional ultrasonography of the fetal heart with spatiotem- image correlation (STIC) in the assessment of the anatomy
poral image correlation. Am J Obstet Gynecol 2003; 189: of pulmonary arteries in fetuses with pulmonary atresia and
1792–1802. ventricular septal defect. Ultrasound Obstet Gynecol 2006; 28:
4. Falkensammer P. Spatio-temporal image correlation for volume 40–46.
ultrasound. Studies of the fetal heart. GE Healthcare: Zipf, 21. International Society of Ultrasound in Obstetrics & Gynecology.
Austria, 2005. Cardiac screening examination of the fetus: guidelines for
5. Goncalves LF, Lee W, Espinoza J, Romero R. Examination of performing the ‘basic’ and ‘extended basic’ cardiac scan.
the fetal heart by four-dimensional (4D) ultrasound with spatio- Ultrasound Obstet Gynecol 2006; 27: 107–113.
temporal image correlation (STIC). Ultrasound Obstet Gynecol 22. Vinals F, Poblete P, Giuliano A. Spatio-temporal image correla-
2006; 27: 336–348. tion (STIC): a new tool for the prenatal screening of congenital
6. Yagel S, Cohen SM, Achiron R. Examination of the fetal heart heart defects. Ultrasound Obstet Gynecol 2003; 22: 388–394.
by five short-axis views: A proposed screening method for 23. Vinals F, Mandujano L, Vargas G, Giuliano A. Prenatal diag-
comprehensive cardiac evaluation. Ultrasound Obstet Gynecol nosis of congenital heart disease using four-dimensional spatio-
2001; 17: 367–369. temporal image correlation (STIC) telemedicine via an Internet
7. Yagel S, Arbel R, Anteby EY, Raveh D, Achiron R. The three link: a pilot study. Ultrasound Obstet Gynecol 2005; 25: 25–31.
vessels and trachea view (3VT) in fetal cardiac scanning. 24. Hyett JA, Perdu M, Sharland GK, Snijders RJM, Nicolaides KH.
Ultrasound Obstet Gynecol 2002; 20: 340–345. Using fetal nuchal translucency to screen for major congenital
8. DeVore GR, Polanco B, Sklansky MS, Platt LD. The ‘spin’ cardiac defects at 10–14 weeks of gestation: population based
technique: a new method for examination of the fetal outflow cohort study. Br Med J 1999; 318: 81–85.
Copyright 2007 ISUOG. Published by John Wiley & Sons, Ltd. Ultrasound Obstet Gynecol 2007; 29: 81–95.Ultrasound in fetal cardiac scanning 95
25. Hyett JA, Perdu NL, Sharland GK, Snijders RJM, Nico- 33. Birk E, Silverman NH. Intracardiac shunt malformations. In
laides KH. Increased nuchal translucency at 10–14 weeks of Fetal Cardiology, Yagel S, Silverman NH, Gembruch U (eds).
gestation as a marker for major cardiac defects. Ultrasound Martin Dunitz: London, 2003; 207 & ff.
Obstet Gynecol 1997; 10: 242–246. 34. Paladini D, Russo MG, Vassallo M, Tartaglione A. The ‘in-
26. Meyer-Wittkopf M, Cole A, Cooper SG, Schmidt S, Sholler GF. plane’ view of the inter-ventricular septum. A new approach
Three-dimensional quantitative echocardiographic assessment to the characterization of ventricular septal defects in the fetus.
of ventricular volume in healthy human fetuses and in fetuses Prenat Diagn 2003; 23: 1052–1055.
with congenital heart disease. J Ultrasound Med 2001; 20: 35. Yagel S, Valsky DV, Messing B. Detailed assessment of fetal
317–327. ventricular septal defect with 4D color Doppler ultrasound
27. Esh-Broder E, Ushakov FB, Imbar T, Yagel S. Application of using spatio-temporal image correlation technology. Ultrasound
free-hand three-dimensional echocardiography in the evaluation Obstet Gynecol 2005; 25: 97–98.
of fetal cardiac ejection fraction: a preliminary study. 36. Moore KL, Persaud TVN. The cardiovascular system. In The
Ultrasound Obstet Gynecol 2004; 23: 546–551. developing human: Clinically oriented embryology (6th edn).
28. Bhat AH, Corbett V, Carpenter N, Liu N, Liu R, Wu A, W. B. Saunders: Philadelphia, PA, 1998; 349–404.
Hopkins G, Sohaey R, Winkler C, Sahn CS, Sovinsky V, Li X, 37. Levental M, Pretorius DH, Sklansky MS, Budorick NE, Nel-
Sahn DJ. Fetal ventricular mass determination on three- son TR, Lou K. Three-dimensional ultrasonography of normal
dimensional echocardiography: studies in normal fetuses and fetal heart: comparison with two-dimensional imaging. J Ultra-
validation experiments. Circulation 2004; 110: 1054–1060. sound Med 1998; 17: 341–348.
29. Bhat AH, Corbett VN, Liu R, Carpenter ND, Liu NW, Wu AM, 38. Meyer-Wittkopf M, Rappe N, Sierra F, Barth H, Schmidt S.
Hopkins GD, Li X, Sahn DJ. Validation of volume and mass Three-dimensional (3-D) ultrasonography for obtaining the four
assessments for human fetal heart imaging by 4-dimensional and five-chamber view: comparison with cross-sectional (2-D)
spatiotemporal image correlation echocardiography: in vitro fetal sonographic screening. Ultrasound Obstet Gynecol 2000;
balloon model experiments. J Ultrasound Med 2004; 23: 15: 397–402.
1151–1159. 39. Meyer-Wittkopf M, Cooper S, Vaughan J, Sholler G. Three-
30. Messing B, Rosenak D, Valsky DV, Cohen SM, Hochner- dimensional (3D) echocardiographic analysis of congenital
Celnikier D, Yagel S. 3D inversion mode combined with spatio- heart disease in the fetus: comparison with cross-sectional (2D)
temporal image correlation (STIC): A novel technique for fetal fetal echocardiography. Ultrasound Obstet Gynecol 2001; 17:
heart ventricle volume quantification. (abstract) Ultrasound 485–492.
Obstet Gynecol 2006; 28: 397. 40. Wang PH, Chen GD, Lin LY. Imaging comparison of basic
31. Carvalho JS, Ho SY, Shinebourne EA. Sequential segmental cardiac views between two- and three-dimensional ultrasound
analysis in complex fetal cardiac abnormalities: a logical in normal fetuses in anterior spine positions. Int J Cardiovasc
approach to diagnosis. Ultrasound Obstet Gynecol 2005; 26: Imaging 2002; 18: 17–23.
105–111. 41. Benacerraf BR, Shipp TD, Bromley B. Three-dimensional US of
32. Yagel S, Kivilevitch Z, Achiron R. The fetal venous system: the fetus: volume imaging. Radiology 2006; 238: 988–996.
normal embryology, anatomy, and physiology and the 42. Michailidis GD, Simpson JM, Karidas C, Economides DL.
development and appearance of anomalies. In Fetal Cardiology, Detailed three-dimensional fetal echocardiography facilitated
Yagel S, Silverman NH, Gembruch U (eds). Martin Dunitz: by an Internet link. Ultrasound Obstet Gynecol 2001; 18:
London, 2003; 321–332. 325–328.
Copyright 2007 ISUOG. Published by John Wiley & Sons, Ltd. Ultrasound Obstet Gynecol 2007; 29: 81–95.You can also read