January 2019- Thyroid Awareness Month - New Castle Presbytery
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
January 2019- Thyroid Awareness Month
A note from the author---
Happy New Year NCP Friends! I hope everyone enjoyed their holiday season
with friends and family. This month, I wanted to feature a topic that hits really close to
home for me—thyroid disease. I have many friends, family, and patients that have been
diagnosed with thyroid disease, but everyone’s experience is slightly different. I want to
begin this article by telling you a story.
About 9 years ago, I was in nursing school and came home one weekend to my
mom complaining about her throat being sore. After asking her more questions, she
described the sensation as most uncomfortable at night when it felt like someone was
“choking her.” The new nurse inside of me immediately examined her neck, as I had just
been taught in school, and I immediately felt a huge lump in the front of her neck, on
both sides of her windpipe. I told her that based on my classes, it seemed as though it
was her thyroid gland and that she had a goiter (which is an enlargement of the thyroid
gland, as you will learn more about below). Of course, she was scared and concerned,
and after visiting her doctor, getting blood work, and going to a specialist, we learned
that she had hypothyroidism and that it runs in families. Now, many years later, her
condition is well controlled with medication, diet, and exercise, and she has learned a lot
about the importance of her thyroid gland on the health of her ENTIRE body. Also, all of
her blood relatives have been able to keep an eye on their thyroid glands as well,
thanks to her proactive approach to her own health and wellness, and her active part in
health promotion.
What is your Thyroid Gland?
Your thyroid gland is a small gland, normally weighing less than one ounce, located in
the front of the neck. It is made up of two halves, called lobes, that lie along the
windpipe (trachea) and are joined together by a narrow band of thyroid tissue, known as
the isthmus.
The thyroid is situated just below your "Adams apple" or larynx.
During development (inside the womb) the thyroid gland
originates in the back of the tongue, but it normally migrates to
the front of the neck before birth. Sometimes it fails to migrate
properly and is located high in the neck or even in the back of
the tongue (lingual thyroid). This is very rare. At other times it
may migrate too far and ends up in the chest (this is also rare).
Although relatively small, the thyroid gland plays a huge role in
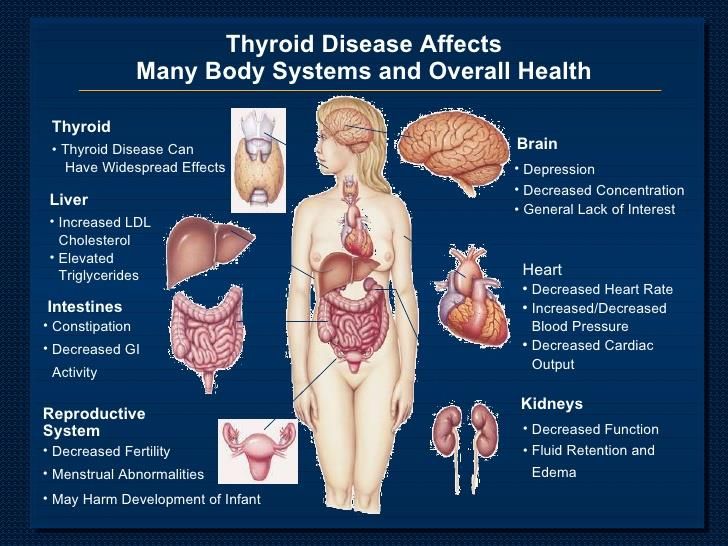
our body, influencing the function of many of the body’s most important organs,
including the heart, brain, liver, kidneys and skin. Ensuring that the thyroid gland is
healthy and functioning properly is vitally important to the body's overall well-being.
What does my Thyroid Gland DO?
The function of the thyroid gland is to take iodine, found in many foods, and convert it
into thyroid hormones:thyroxine (T4) and triiodothyronine (T3).Thyroid cells are the only
cells in the body which can absorb iodine. These cells combine iodine and the amino
acid tyrosine to make T3 and T4. T3 and T4 are then released into the blood stream
and are transported throughout the body where they control metabolism (conversion of
oxygen and calories to energy).
Every cell in the body depends upon
thyroid hormones for regulation of their
metabolism. The normal thyroid gland
produces about 80% T4 and about 20%
T3, however, T3 possesses about four
times the hormone "strength" as T4.
The thyroid gland is under the control of the pituitary gland,
a small gland the size of a peanut at the base of the brain
(shown here in orange). When the level of thyroid
hormones (T3 & T4) drops too low, the pituitary gland
produces Thyroid Stimulating Hormone (TSH) which
stimulates the thyroid gland to produce more hormones.
Under the influence of TSH, the thyroid will manufacture
and secrete T3 and T4 thereby raising their blood levels.
The pituitary senses this and responds by decreasing its
TSH production. One can imagine the thyroid gland as a
furnace and the pituitary gland as the thermostat.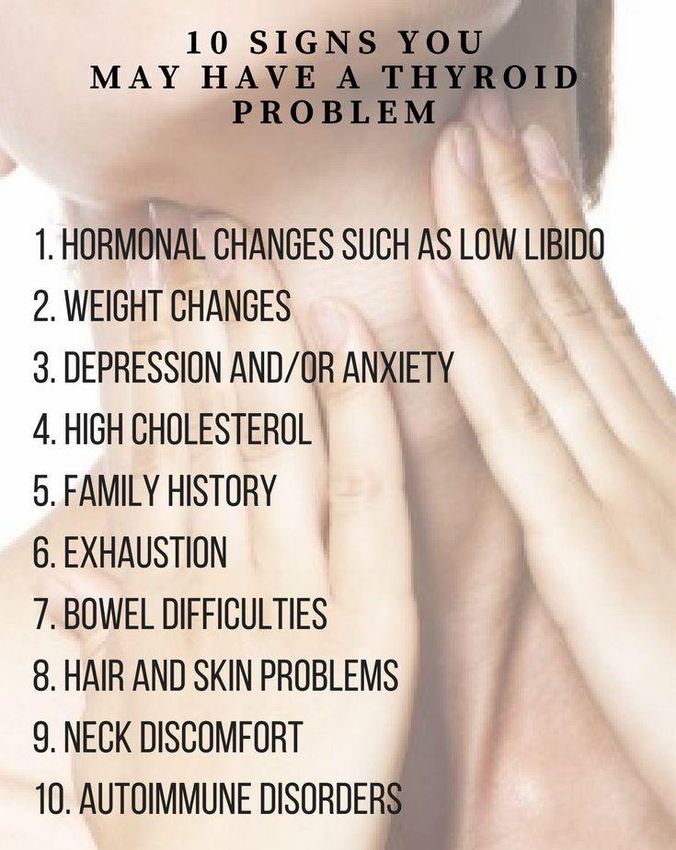
Thyroid hormones are like heat. When the heat gets back to the thermostat, it turns the thermostat off. As the room cools (the thyroid hormone levels drop), the thermostat turns back on (TSH increases) and the furnace produces more heat (thyroid hormones). The pituitary gland itself is regulated by another gland, known as the hypothalamus (shown in the picture above in light blue). The hypothalamus is part of the brain and produces TSH Releasing Hormone (TRH) which tells the pituitary gland to stimulate the thyroid gland (release TSH). One might imagine the hypothalamus as the person who regulates the thermostat since it tells the pituitary gland at what level the thyroid should be set. How Common is Thyroid Disease? Thyroid disease is more common than diabetes or heart disease. Thyroid disease is a fact of life for as many as 30 million Americans – and more than half of those people remain undiagnosed. Women are five times more likely than men to suffer from hypothyroidism (when the gland is not producing enough thyroid hormone). Aging is just one risk factor for hypothyroidism.
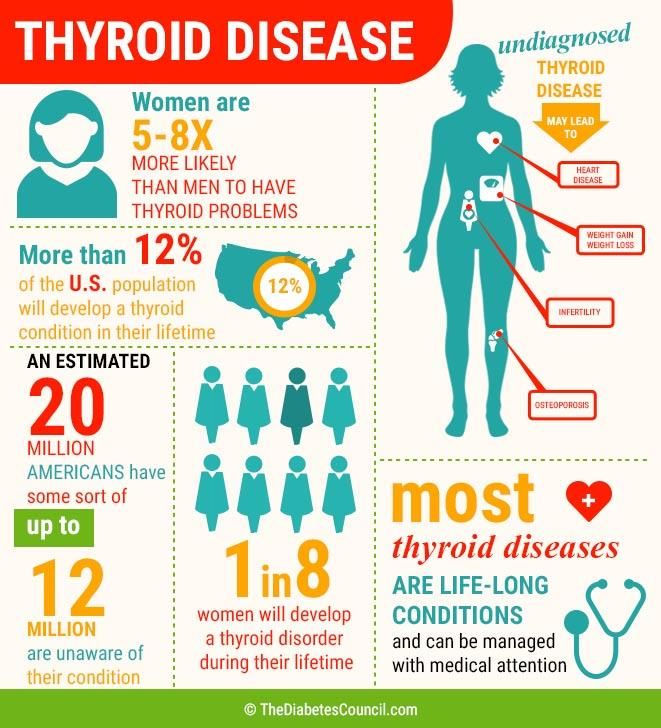
How important is my thyroid in my overall well-being? The thyroid gland produces thyroid hormone, which controls virtually every cell, tissue and organ in the body. If your thyroid is not functioning properly, it can produce too much thyroid hormone, which causes the body’s systems to speed up (hyperthyroidism); or it can create too little thyroid hormone, which causes the body’s systems to slow down (hypothyroidism). Untreated thyroid disease may lead to elevated cholesterol levels and subsequent heart disease, as well as infertility and osteoporosis. Research also shows that there is a strong genetic link between thyroid disease and other autoimmune diseases, including types of diabetes, arthritis and anemia. Simply put, if your thyroid gland isn’t working properly, neither are you. How does the Thyroid Gland Impact Your ENTIRE Body? Excerpted from The Harvard Medical School Guide to Overcoming Thyroid Problems by Dr. Jeffrey R. Garber, published by McGraw-Hill. Think of your thyroid as a car engine that sets the pace at which your body operates. An engine produces the required amount of energy for a car to move at a certain speed. In the same way, your thyroid gland manufactures enough thyroid hormone to prompt your cells to perform a function at a certain rate. Just as a car can’t produce energy without gas, your thyroid needs fuel to produce thyroid hormone. This fuel is iodine. Iodine comes from your diet and is found in iodized table salt, seafood, bread and milk. Your thyroid extracts this necessary ingredient from
your bloodstream and uses it to make two kinds of thyroid hormone: thyroxine, also called T4 because it contains four iodine atoms, and triiodothyronine, or T3, which contains three iodine atoms. T3 is made from T4 when one atom is removed, a conversion that occurs mostly outside the thyroid in organs and tissues where T3 is used the most, such as the liver, the kidneys and the brain. Once T4 is produced, it is stored within the thyroid’s vast number of microscopic follicles. Some T3 is also produced and stored in the thyroid. When your body needs thyroid hormone, it is secreted into your bloodstream in quantities set to meet the metabolic needs of your cells. The hormone easily slips into the cells in need and attaches to special receptors located in the cells’ nuclei. Your car engine produces energy, but you tell it how fast to go by stepping on the accelerator. The thyroid also needs some direction; it gets this from your pituitary gland, which is located at the base of your brain. No larger than a pea, the pituitary gland is sometimes known as the “master gland” because it controls the functions of the thyroid and the other glands that make up the endocrine system. Your pituitary gland sends messages to your thyroid gland, telling it how much thyroid hormone to make. These messages come in the form of thyroid- stimulating hormone (TSH). TSH levels in your bloodstream rise or fall depending on whether enough thyroid hormone is produced to meet your body’s needs. Higher levels of TSH prompt the thyroid to produce more thyroid hormone. Conversely, low TSH levels signal the thyroid to slow down production. The pituitary gland gets its information in several ways. It is able to read and respond directly to the amounts of T4 circulating in the blood, but it also responds to the hypothalamus, which is a section of the brain that releases its own hormone, thyrotropin-releasing hormone (TRH). TRH stimulates TSH production in the pituitary gland. This network of communication between the hypothalamus, the pituitary gland, and the thyroid gland is referred to as the hypothalamic-pituitary-thyroid axis (HPT axis).
Thyroid Disorders Through the hormones it produces, the thyroid gland influences almost all of the metabolic processes in your body. Thyroid disorders can range from a small, harmless goiter (enlarged gland) that needs no treatment to life-threatening cancer. The most common thyroid problems involve abnormal production of thyroid hormones. Too much thyroid hormone results in a condition known as hyperthyroidism. Insufficient hormone production leads to hypothyroidism. Although the effects can be unpleasant or uncomfortable, most thyroid problems can be managed well if properly diagnosed and treated. The Chemical Imbalance The HPT axis is a highly efficient network of communication. Normally, the thyroid doles out just the right amount of hormone to keep your body running smoothly. TSH levels remain fairly constant, yet they respond to the slightest changes in T4 levels and vice versa. But even the best networks are subject to interference. When outside influences such as disease, damage to the thyroid or certain medicines break down communication, your thyroid might not produce enough hormone. This would slow down all of your body’s functions, a condition known as hypothyroidism or
underactive thyroid. Your thyroid could also produce too much hormone sending your systems into overdrive, a condition known as hyperthyroidism or overactive thyroid. These two conditions are most often features of an underlying thyroid disease. When considering thyroid disease, doctors ask two main questions: First, is the thyroid gland inappropriately producing an abnormal amount of thyroid hormone? And second, is there a structural change in the thyroid, such as a lump—known as a nodule —or an enlargement—known as a goiter? Though one of these characteristics does not necessarily imply that the other is present, many thyroid disorders display both. Hypothyroidism- The Car is Out of Gas Sometimes the thyroid can’t meet your body’s demands for thyroid hormone, even though TSH levels increase. As your body slows down, you may feel cold, tired and even depressed. You may gain weight, even though you’re eating less. There could be a number of reasons why your thyroid is not performing well. For example, if your body isn’t getting enough iodine, your thyroid can’t make enough thyroid hormone, but it will try to respond to rising TSH levels by working harder and harder anyway. This can cause your thyroid to become enlarged and develop into a goiter that looks like a protrusion or large swelling in your neck. Goiters used to be
common, but they have become much less common in developed countries because of iodine-fortified foods. In other cases, your thyroid comes under attack by your body’s own immune system. Normally, substances called antibodies protect you from dangerous bacteria and viruses. But in this condition, known as Hashimoto’s thyroiditis, your antibodies mistake your thyroid for a foreign invader. Hashimoto’s thyroiditis involves the presence of two types of antibodies called antithyroid peroxidase (anti-TPO) and antithyroglobulin (anti-TG) antibodies. These antibodies play a role in the destruction of the thyroid by the immune system. Over time, your defenseless thyroid, inflamed and scarred, surrenders and fails. Ailments like Hashimoto’s thyroiditis that result from an abnormal immune response are called autoimmune diseases. Hashimoto’s thyroiditis is but one form of thyroiditis —an inflammation of the thyroid—that causes hypothyroidism. Hyperthyroidism- The Car is Revved Up Sometimes your thyroid keeps churning out more thyroid hormone, even when your pituitary gland completely shuts down TSH production, a clear signal that your body has had enough. Yet the thyroid appears oblivious to the lack of signals and continues to

produce too much, pushing your metabolism into overdrive and speeding up your body’s processes. This is hyperthyroidism. If you’re hyperthyroid, your pulse may be racing, you feel irritable and overheated, and you have trouble sleeping. You may lose weight in spite of a good appetite and experience anxiety and nervousness. As with hypothyroidism, you may develop a goiter; in this case, your thyroid enlarges because your thyroid is working so hard overproducing thyroid hormone. A toxic multinodular goiter is to blame for hyperthyroidism in many people over 60 years old. This occurs when the thyroid enlarges and develops nodules, which are essentially lumps of thyroid cells that form as part of the thyroid. Nodules may develop on the outer surface of the gland where the doctor can feel them during an examination. If they develop inside the gland, however, they may not be apparent to the touch. Nodules throw off communication between the thyroid and the pituitary gland because they independently produce thyroid hormone and do not depend on TSH to produce hormone. A type of single nodule, called a solitary toxic adenoma, causes hyperthyroidism in the same way—by producing thyroid hormone at its own whim, regardless of the messages from the pituitary gland. Not all nodules cause thyroid imbalance. There are different kinds of single nodules that can range from the size of a pea, or even smaller, to the size of a plum, or even bigger. Most are completely harmless and don’t affect thyroid function in the least. These include fluid-containing nodules called cysts and adenomas, which are solid but equally harmless. A very small percentage of nodules are cancerous. Cancerous
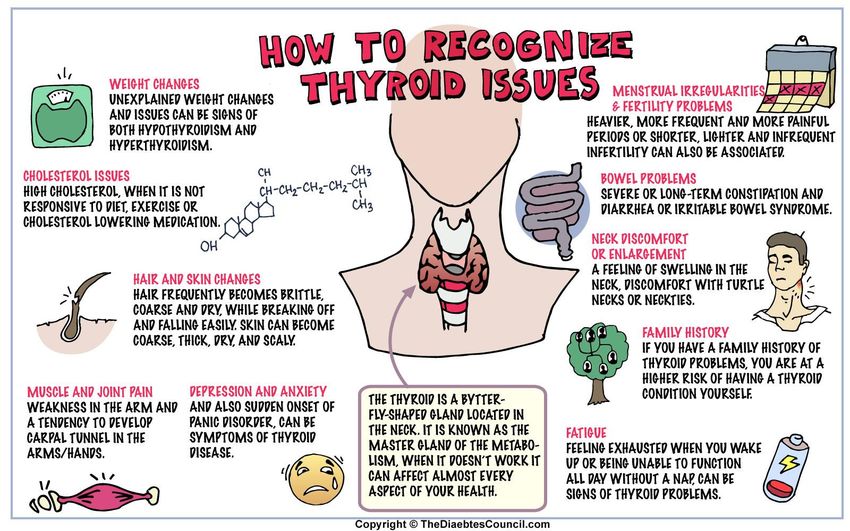
nodules do not directly affect thyroid function and therefore do not cause an overactive or underactive thyroid. Another cause of a revved-up thyroid is Graves’ disease, an autoimmune disease that is the most common cause of hyperthyroidism in the United States. As with Hashimoto’s thyroiditis, antibodies attack the thyroid, but in this case they stimulate the thyroid to overproduce thyroid hormone. The kinds of antibodies present in Graves’ disease are known as thyrotropin receptor antibodies (TRAb), including one kind known as thyroid- stimulating immunoglobulins (TSIs). They work by mimicking TSH, attaching to the TSH receptor on the thyroid gland and confusing the thyroid into producing too much hormone. In addition to symptoms of hyperthyroidism, some people with Graves’ disease develop thyroid eye disease. Its features vary from case to case and may be characterized by swollen, bulging, red eyes; widely open eyelids; and double vision. In its most severe form, diminished visual acuity may be present. How do you know if you have a thyroid problem? First, you must understand how to recognize the symptoms and risk factors of thyroid disease. Since many symptoms may be hidden or mimic other diseases and conditions, the best way to know for sure is to ask your doctor for a TSH (thyroid-stimulating hormone) test, a simple blood test to verify your thyroid gland’s condition. Also, take a minute and perform a self Neck Check. And because thyroid disease often runs in families, examinations of your family members and a review of their medical histories may reveal other individuals with thyroid problems.
What are some of the reasons to consider a thyroid evaluation?
Family history: A familiar place to look for thyroid disorder signs and symptoms
is your family tree. If you have a first-degree relative (a parent, sibling or child)
with thyroid disease, you would benefit from thyroid evaluation. Women are much
more likely to be thyroid patients than men; however, the gene pool runs through
both.
Prescription medications: If you are taking Lithium or Amiodarone, you should
consider a thyroid evaluation.
Radiation therapy to the head or neck: If you have had any of the following
radiation therapies, you should consider a thyroid evaluation: radiation therapy
for tonsils, radiation therapy for an enlarged thymus, or radiation therapy for
acne.
Chernobyl: If you lived near Chernobyl at the time of the 1986 nuclear accident,
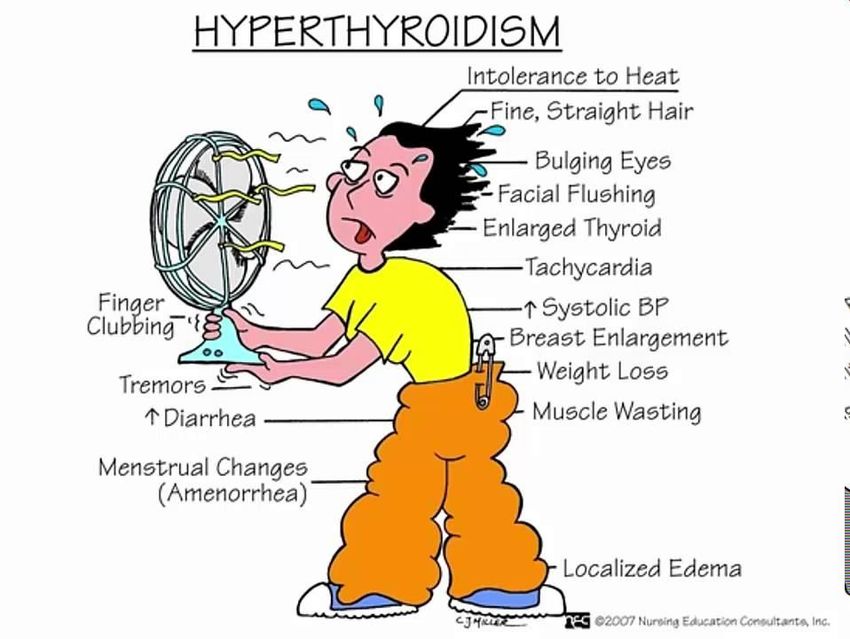
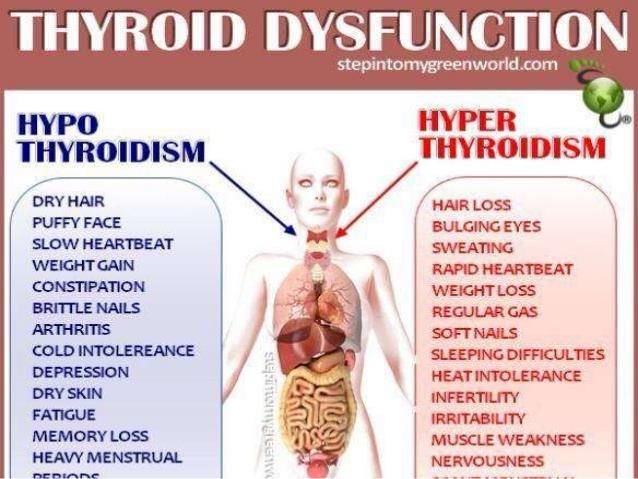
you should consider a thyroid evaluation.Symptoms of Thyroid Disease Hyperthyroidism Symptoms The symptoms of hyperthyroidism can include: Fast heart rate (usually over 100 beats per minute) Feeling anxious or irritable Weight loss Trembling hands Loss of head hair Fingernails separating from nail bed Intolerance to warm temperatures and increased sweating Muscle weakness – especially in upper arms and thighs Loose and frequent bowel movements Protrusion of the eyes, with or without blurred vision
Hypothyroidism Hypothyroidism (under active thyroid) is the most common thyroid problem. The symptoms of hypothyroidism can include: Constant fatigue Forgetfulness Difficulty learning Puffy face Dry, brittle hair and nails Dry, itchy skin Constipation Sore muscles Weight gain Heavy or irregular menstrual cycle If you have symptoms of thyroid disease, your doctor can order a blood test to check TSH levels. TSH levels that are too low or too high can indicate a problem with the thyroid and further testing will be done to confirm the diagnosis and cause. Treatments
for thyroid disorder will depend on the type of thyroid disorder (hypo or hyperthyroidism)
and the cause.
What causes Thyroid Problems?
All types of hyperthyroidism are due to an overproduction of thyroid hormones, but the
condition can occur in several ways:
Graves' disease: The production of too much thyroid hormone.
Toxic adenomas: Nodules develop in the thyroid gland and begin to secrete thyroid
hormones, upsetting the body's chemical balance; some goiters may contain several
of these nodules.
Subacute thyroiditis: Inflammation of the thyroid that causes the gland to "leak"
excess hormones, resulting in temporary hyperthyroidism that generally lasts a few
weeks but may persist for months.
Pituitary gland malfunctions or cancerous growths in the thyroid gland:
Although rare, hyperthyroidism can also develop from these causes.
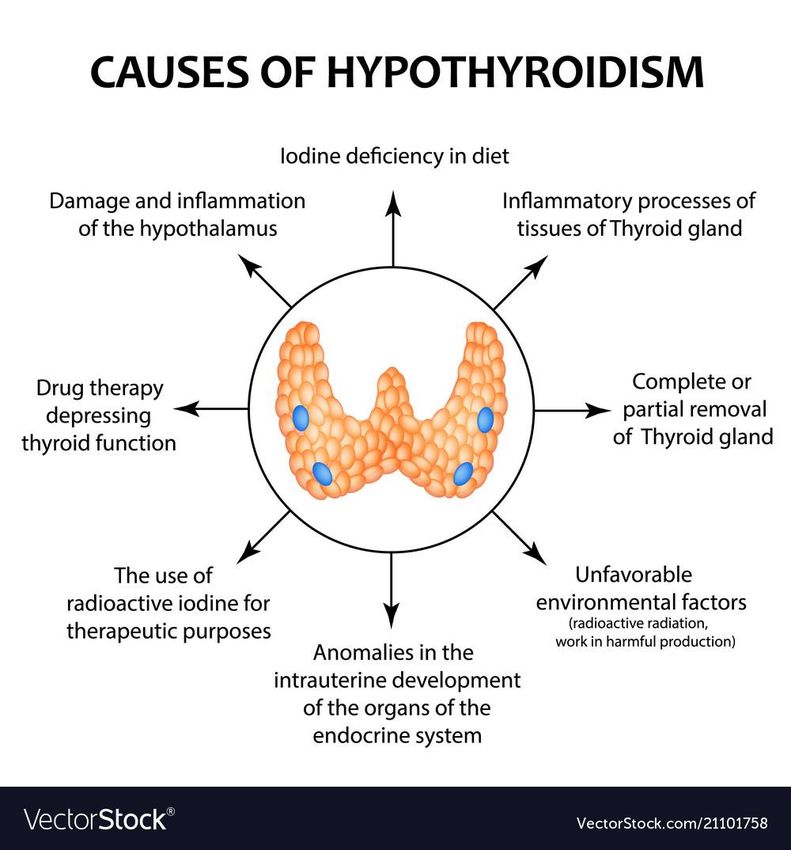
Hypothyroidism, by contrast, stems from an underproduction of thyroid hormones. Since
your body's energy production requires certain amounts of thyroid hormones, a drop in
hormone production leads to lower energy levels. Causes of hypothyroidism include:
Hashimoto's thyroiditis : In this autoimmune disorder, the body attacks thyroid
tissue. The tissue eventually dies and stops producing hormones.
Removal of the thyroid gland: The thyroid may have been surgically removed or
chemically destroyed.
Exposure to excessive amounts of iodide: Cold and sinus medicines, the heart
medicine amiodarone, or certain contrast dyes given before some X-rays may
expose you to too much iodine. You may be at greater risk for developing
hypothyroidism if you have had thyroid problems in the past. This drug has also been
implicated as a cause of hypothyroidism.
Untreated for long periods of time, hypothyroidism can bring on a myxedema coma, a rare
but potentially fatal condition that requires immediate hormone treatment.
Thyroid Cancer
Cancer of the thyroid gland is quite rare and occurs in about 5% of thyroid nodules. You
might have one or more thyroid nodules for several years before they are determined to be
cancerous. People who have received radiation treatment to the head and neck earlier in
life, possibly as a remedy for acne, tend to have a higher-than-normal risk of developing
thyroid cancer.
Hypothyroidism in Babies
Hypothyroidism poses a special danger to newborns and infants. A lack of thyroid hormones
in the system at an early age can lead to the development of cretinism (mental retardation)
and dwarfism (stunted growth). Most infants now have their thyroid levels checked routinely
soon after birth. If they are hypothyroid, treatment begins immediately. In infants, as in
adults, hypothyroidism can be due to these causes: A pituitary disorder A defective thyroid Lack of the gland entirely A hypothyroid infant is unusually inactive and quiet, has a poor appetite, and sleeps for excessively long periods of time. Diagnosing Thyroid Disease Your doctor may prescribe one test at first, or a variety of tests to confirm the diagnosis of a thyroid disorder. Every patient is different and it is important to have an open dialogue with your doctor about the tests being ordered, as well as the results. Here is some helpful information while preparing for your tests: Do I need to stop taking my thyroid pills for these tests? You may already be taking a type of “pill” for your thyroid gland when your doctor indicates that you need one of the following tests (whether you have just been diagnosed, you have known about your thyroid disease diagnosis, or you are displaying clear symptoms of thyroid disease prior to an official diagnosis). If you are having any type of blood test to measure your thyroid levels or any type of thyroid scan or biopsy, as your doctor about whether or not you should continue taking your medication, or stop taking it for a certain period of time prior to these tests.
Since Euthyrox or Synthroid (and most other thyroid pills) behave exactly as normal
human thyroid hormone, they are not rapidly cleared from the body as other
medications are. Most thyroid pills have a half life of 6.7 days which means they must
be stopped for four to five weeks (five half lives) before accurate thyroid testing is
possible. An exception to the long half life of thyroid medication is Cytomel - a thyroid
pill with a half life of only forty-eight hours. Therefore it is possible to change a person's
thyroid replacement to Cytomel for one month to allow time for his regular pills to clear
the body. Cytomel is then stopped for ten days (five half lives) and the appropriate test
can then be done. Usually patients, even those who have no remaining thyroid function,
tolerate being off thyroid replacement only ten days quite well.
Blood Tests
The first test your doctor will typically prescribe is taking a blood sample, which can
show the measurements of thyroid hormones in your bloodstream. Depending on the
amount of certain types of thyroid hormones in your bloodstream at any given time allow
the doctor to determine if your thyroid gland is secreting too little, too much, or not
enough thyroid hormones.
Here are some common types of thyroid hormone blood tests that your doctor may refer
to:
TSH - measures thyroid-stimulating hormone. It is the most accurate measure of
thyroid activity.
T3 and T4 - measure different thyroid hormones.
TSI - measures thyroid-stimulating immunoglobulin.
Antithyroid antibody test - measures antibodies (markers in the blood).
Understanding the Results of the Blood Test
Your doctor can diagnose hyperthyroidism and hypothyroidism by testing the levels
of thyroid hormones in your blood. The tests measure hormones from the thyroid itself, as
well as thyroid-stimulating hormone (TSH), a chemical released by the pituitary gland that
triggers your thyroid.When you are hypothyroid, you have higher TSH levels because your body is trying to tell your thyroid to make more hormones. The reverse is true with hyperthyroidism: TSH levels are below normal and thyroid hormone levels are high. One uncommon type of thyroid cancer can be diagnosed through a blood test that measures levels of a hormone called calcitonin that's needed to build bones. Iodine Uptake Scan This test is a means of measuring thyroid function is to measure how much iodine is taken up by the thyroid gland (RAI uptake). Remember, cells of the thyroid normally absorb iodine from our blood stream (obtained from foods we eat) and use it to make thyroid hormone. Doctors often use this to identify the cause of hyperthyroidism. It tracks the amount of iodide absorbed by the thyroid gland. We get this mineral from the foods we eat. It's a key ingredient of thyroid hormone, so the amount of iodide your thyroid absorbs is a good way to tell how much hormone the gland is making. First, the doctor places a device over your neck to measure how much background radioactivity there is. Then, you swallow a small amount of radioactive iodide in a liquid or as a capsule. After a time, usually 4-6 hours and at most 24 hours, she takes another measurement to see how much of the radioactive iodide has gathered in your thyroid. When the gland has a lot of iodide, the doctor may do a radioactive iodide uptake scan. She'll use a special film to make a picture that shows the exact location of the radioactive iodide in your thyroid. Iodide collecting in nodules suggests that they're responsible for the extra hormone. If the scan shows that the iodide is spread throughout the gland, the whole thyroid is involved. Hypothyroid patients usually take up too little iodine and hyperthyroid patients take up too much iodine. The test is performed by giving a dose of radioactive iodine on an empty stomach. The iodine is concentrated in the thyroid gland or excreted in the urine over the next few hours. The amount of iodine that goes into the thyroid gland can be measured by a "Thyroid Uptake". Of course, patients who are taking thyroid medication will not take up as much iodine in their thyroid gland because their own thyroid gland is turned off and is not functioning. At other times the gland will concentrate iodine normally but will be unable to convert the iodine into thyroid hormone; therefore, interpretation of the iodine uptake is usually done in conjunction with blood tests. Thyroid Scan Taking a "picture" of how well the thyroid gland is functioning requires giving a radioisotope to the patient and letting the thyroid gland concentrate the isotope (just like the iodine uptake scan above). Therefore, it is usually done at the same time that the iodine uptake test is performed. Although other isotopes, such as technetium, will be concentrated by the thyroid gland; these isotopes will not measure iodine uptake which is what we really want to know because the production of thyroid hormone is dependent upon absorbing
iodine. It has also been found that thyroid nodules that concentrate iodine are rarely
cancerous; this is not true if the scan is done with technetium. Therefore, all scans are
now done with radioactive iodine. Both of the scans above show normal sized thyroid
glands, but the one on the left has a "HOT" nodule in the lower aspect of the right lobe,
while the scan on the right has a "COLD" nodule in the lower aspect
of the left lobe (outlined in red and yellow). Pregnant women should
not have thyroid scans performed because the iodine can cause
development troubles within the baby's thyroid gland.
Two types of thyroid scans are available. A camera scan is performed
most commonly which uses a gamma camera operating in a fixed
position viewing the entire thyroid gland at once. This type of scan
takes only five to ten minutes. In the 1990's, a new scanner called a
Computerized Rectilinear Thyroid (CRT) scanner was introduced. The
CRT scanner utilizes computer technology to improve the clarity of thyroid scans and
enhance thyroid nodules. It measures both thyroid function and thyroid size. A life-sized
1:1 color scan of the thyroid is obtained giving the size in square centimeters and the
weight in grams. The precise size and activity of nodules in relation to the rest of the
gland is also measured. CTS of the normal thyroid gland In addition to making thyroid
diagnosis more accurate, the CRT scanner improves the results of thyroid biopsy. The
accurate sizing of the thyroid gland aids in the follow-up of nodules to see if they are
growing or getting smaller in size. Knowing the weight of the thyroid gland allows more
accurate radioactive treatment in patients who have Graves' disease.
Thyroid Scans are used for the following reasons:
Identifying nodules and determining if they are "hot" or "cold".
Measuring the size of the goiter prior to treatment.
Follow-up of thyroid cancer patients after surgery.
Locating thyroid tissue outside the neck, i.e. base of the tongue or in the chest.Thyroid Ultrasound
Nodules that appear suddenly are typically fluid-filled sacs. Your doctor can check them with
an ultrasound exam. Thyroid ultrasound refers to the use of high frequency sound waves
to obtain an image of the thyroid gland and identify nodules. It tells if a nodule is "solid"
or a fluid-filled cyst, but it will not tell if a nodule is benign or malignant. Ultrasound
allows accurate measurement of a nodule's size and can determine if a nodule is getting
smaller or is growing larger during treatment.
Depending on a nodule's size, how it looks on ultrasound, and your chances for
getting thyroid cancer, your doctor may do an aspiration or biopsy, Ultrasound aids in
performing thyroid needle biopsy by improving accuracy if the nodule cannot be felt
easily on examination. She'll take a tissue sample of the nodule and examine it. Further
tests will show if the nodule has the potential to become cancerous.
Thyroid Antibodies
The body normally produces antibodies to foreign substances such as bacteria;
however, some people are found to have antibodies against their own thyroid tissue. A
condition known as Hashimoto's Thyroiditisis associated with a high level of these
thyroid antibodies in the blood. Whether the antibodies cause the disease or whether
the disease causes the antibodies is not known; however, the finding of a high level of
thyroid antibodies is strong evidence of this disease. Occasionally, low levels of thyroid
antibodies are found with other types of thyroid disease. When Hashimoto's thyroiditis
presents as a thyroid nodule rather than a diffuse goiter, the thyroid antibodies may not
be present.
Thyroid Needle Biopsy
This has become the most reliable test to differentiate the "cold" nodule that is cancer
from the "cold" nodule that is benign ("hot" nodules are rarely cancerous). It provides
information that no other thyroid test will provide. While not perfect, it will provide
definitive information in 75% of the nodules biopsied.Treatment of Thyroid Disease For thyroid disorders stemming from the over- or under-production of thyroid hormones, you want to try to restore the hormone levels to their proper balance. Hyperthyroidism needs treatment that will slow down the making of thyroid hormone, while hypothyroidism needs hormone replacement. Drugs and surgery are usually effective ways to adjust hormone levels. Other treatments, including diet supplements, herbal remedies, and special exercises, may relieve some of the discomfort and help the thyroid gland work better. Before she decides which treatment is best for you, your doctor will consider your particular thyroid condition as well as your age, general health, and past medical issues. Subacute Thyroiditis Treatment Although subacute thyroiditis can bring on temporary hyperthyroidism, this condition doesn't require medical treatment. You can take acetaminophen or aspirin for any pain from the inflamed thyroid. (Children under age 19 shouldn't take aspirin because it's been linked to Reye's syndrome.) If over-the-counter drugs don't help, your doctor may prescribe anti-inflammatory drugs like prednisone or dexamethasone for a short time. Hyperthyroidism Treatment Thyroid hormone production can be slowed or stopped completely with: Radioactive iodide treatment
Anti-thyroid medication Surgery If your doctor decides that radioactive treatment is best, you'll swallow a tablet or liquid with enough radioactive iodide to damage the cells of your thyroid gland so they can't make hormones. Sometimes you'll need more than one treatment to cut back hormone production to a normal level. Many people develop hypothyroidism as a result of this procedure. After you start using anti-thyroid medications, your symptoms should begin to disappear in about 6-8 weeks. But you'll typically need to keep taking the medication for about a year. At that time, your doctor will check to see if you can stop. You'll need regular checkups once you're off the medicine to make sure your hormone levels stay balanced. Doctors don't usually do surgery unless you're pregnant (and can’t take anti-thyroid medicine) or have a large goiter or cancerous nodule. Hypothyroidism Treatment Someone with hypothyroidism will have to take thyroid hormone replacement for the rest of his/her life. No surgery, drugs, or complementary medicine can boost your thyroid once it slows down. Doctors generally prescribe man-made forms of thyroid hormone, such as levothyroxine. Side effects are rare, but some people have nervousness or chest pain while taking these drugs. Adjusting the dose of medication usually gets rid of any unpleasant effects. Let your doctor know about everything you're taking, because some things could affect how well the medication works: Diabetes Antidepressants Estrogen in hormone replacement therapy or birth control The blood-thinning drug warfarin The heart drug digitalis Supplements and products with magnesium, aluminum, iron, or soy
Thyroid Cancer Treatment
The first way to treat thyroid cancer is usually by removing either the cancerous tissue
or the whole thyroid gland, a surgical procedure known as a thyroidectomy.
If the cancer has spread, any other affected tissue, such as the lymph glands in the
neck, will be removed, too.
Complementary and Alternative Medicine
Some people try other therapies to cleanse the body, restore immune function, and
balance the production and release of hormones. You should talk to your doctor if you're
interested in these other methods to make sure they won't harm you or interfere with
your treatment.
A naturopath may use homeopathic mixtures, herbs, preparations based on traditional
Chinese medicine (which links thyroid problems to emotional distress),
and acupuncture to remove blocks to your ''life force energy.'' Naturopaths are
authorized to treat thyroid disease in some states, but in others, it's illegal. While they
may help with the stress associated with thyroid disease, there are no good studies
showing that these therapies are effective for treating thyroid disorders.
Chiropractors use spinal manipulation to treat symptoms of thyroid disorders by easing
muscle tension and improving blood circulation.
Diet and Nutrition
Protein, calcium, magnesium, and iodine help your thyroid work. Make sure you're
getting plenty of all the B vitamins, vitamin A, and vitamin C.
If you don't have enough iodine in your system, taking selenium can cause hypothyroidism.
Avoid these products:
Pseudoephedrine (found in over-the-counter cold remedies) can cause
nervousness, insomnia, headache, and high blood pressure. Alkaloids, including caffeine, morphine, and quinine, can raise your blood
pressure and heart rate.5 Things to Do If Your Thyroid Hormone Medication Isn't Working If you're still feeling depressed, tired and the scale won't budge, you'd be surprised how these small tweaks can get your TSH levels normalized. For about one in seven of the 10 to 12 million Americans with an underactive thyroid gland, conventional treatment with the synthetic thyroid hormone levothyroxine just isn’t enough.1 If you continue to feel sick, tired, depressed or have symptoms like stubborn weight gain, it’s worth talking with your doctor about the best solution for treating your hypothyroidism. But in the meantime, these tips might be just what you need to help you get the most out of your levothyroxine: #1. Time levothyroxine for optimal absorption. For best absorption into your bloodstream, levothyroxine should be taken on an empty stomach—30 to 60 minutes before breakfast, or three or more hours after dinner. Taking levothyroxine with or too soon before or after a meal or snack could reduce absorption to 64%, from a high of 80% when you’re fasting, according to the American Thyroid Association (ATA). 3Just changing your timing could bring your thyroid levels back into a normal range. In one older but often-cited Italian study 4 of four people whose thyroid numbers were not in control despite taking thyroid hormone, researchers found that they all took their medication just 15-20 minutes before breakfast. Changing their routine, so they took thyroid hormone 60 minutes before their morning meal, improved their numbers within a month. Take it with water. In another Italian study, coffee interfered with absorption. 5 And don’t take antacids or supplements containing calcium or iron with four hours of your levothyroxine. #2. Practice patience and ask for tests. Some people start feeling more energetic and alert within a week or two of starting thyroid hormone – but not everyone. It could take a month or two to feel better. And you may have to see your doctor several times for tests of your blood levels of thyroid stimulating hormone (TSH) and adjustments to your levothyroxine dose to get it just right. #3. Don't switch back-and-forth between brand-name and generic levothyroxine. Switching from a brand-name to generic thyroid hormone, or vice-versa could affect your TSH levels—even if the dose is the same. 7 The US Food and Drug Administration requires that all levothyroxine preparations deliver 95-105% of the potency on the label. But, the ATA notes, even tiny variations could make a difference. That’s why the group’s guidelines recommend sticking with the drug type (generic or brand name) to keep your TSH levels steady. (Ask for it at every refill.) If you’ve made a switch and have concerns, have your doctor retest your TSH level, the ATA, American Association of Clinical Endocrinologists, and The Endocrine Society have recommended in a joint statement. #4. Consider adding T3, but know that it might not help. Stories about the purported wonders of synthetic triiodothyronine (T3) for hypothyroid symptoms are all over the internet—but don’t believe everything you read. Some endocrinologists
recommend that people whose hypothyroidism symptoms persist despite normal TSH levels try adding T3 to their levothyroxine therapy. T3 is the body’s active form of the thyroid hormone thyroxine. Enzymes in organs like the liver, brain, and heart convert thyroxine (T4) into T3 and the thyroid gland produces some as well. For most people with hypothyroidism, the body converts levothyroxine into T3. But there’s evidence this doesn’t always happen. Early research from Chicago’s Rush University suggests that a genetic mutation could be responsible, preventing enzymes from making the conversion. But more studies are needed. Meanwhile, many experts maintain this unproven combo therapy isn’t ready for prime time. The ATA’s 2014 guidelines say it shouldn’t be used routinely because long-term studies have yet to prove it has benefits, while the European Thyroid Association (ETA) since 2012 has considered it an “experimental treatment modality” for people whose fatigue, depression, weight gain and other hypothyroidism symptoms haven’t waned even though taking levothyroxine alone has moved their TSH levels into the normal range. Testing T3 levels in people with lingering symptoms is also controversial. In one new study, published in April 2017 in the European Thyroid Journal, researchers found that combination therapy helped 24 out of 37 people in this situation. But it didn’t seem to matter whether they had low T3 levels beforehand or if their levels rose during treatment. If you’re curious about T3, talk it over with your doctor. It’s also wise to check that your health insurance covers testing and treatment. #5. Skip “natural” thyroid medications and supplements. Many supplements claim to “support” thyroid health—but some are laced with thyroid hormones not listed on the label. Adding them to your medication could mean you’re getting too much. In a 2013 study of 10 top-selling thyroid-support products sold on the internet, researchers from Germany’s Landstuhl Regional Medical Center and from the Walter Reed Army National Military Medical Center in Bethesda, MD, found that nine were laced with T3, T4 or both in a variety of amounts. Ingredient labels listed animal thyroid tissue for some while others only listed herbs such as ashwagandha, guggul, and Coleus forskohlii. The researchers concluded that drugs were added to the supplements. 12Supplements, including types containing a seaweed called kelp, may also contain dangerously high levels of iodine. And natural thyroid supplements may contain gland tissue from the thyroid, liver, heart, pancreas and other animal organs—raising a small but serious risk for exposure to prions, which are agents that could transmit the brain disease Creutzfeldt–Jakob. Resources https://www.ihs.gov/newsroom/announcements/2018-announcements/national-thyroid- awareness-month/
https://www.webmd.com/women/guide/understanding-thyroid-problems-basics#1 http://thyroidawareness.com/ https://www.thyroid.org/january-thyroid-awareness/ https://medlineplus.gov/thyroiddiseases.html https://www.endocrineweb.com/conditions/thyroid/all http://thyroidawareness.com/neck-check
You can also read

















































