Virchow-Robin Spaces at MR Imaging1 - Neurotalk
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Note: This copy is for your personal non-commercial use only. To order presentation-ready
copies for distribution to your colleagues or clients, contact us at www.rsna.org/rsnarights.
EDUCATION EXHIBIT 1071
Virchow-Robin Spaces
at MR Imaging1
Robert M. Kwee, MD ● Thomas C. Kwee, MD
TEACHING
POINTS
See last page Virchow-Robin (VR) spaces surround the walls of vessels as they
course from the subarachnoid space through the brain parenchyma.
Small VR spaces appear in all age groups. With advancing age, VR
spaces are found with increasing frequency and larger apparent sizes.
At visual analysis, the signal intensity of VR spaces is identical to that
of cerebrospinal fluid with all magnetic resonance imaging sequences.
Dilated VR spaces typically occur in three characteristic locations:
Type I VR spaces appear along the lenticulostriate arteries entering the
basal ganglia through the anterior perforated substance. Type II VR
spaces are found along the paths of the perforating medullary arteries
as they enter the cortical gray matter over the high convexities and ex-
tend into the white matter. Type III VR spaces appear in the midbrain.
Occasionally, VR spaces have an atypical appearance. They may be-
come very large, predominantly involve one hemisphere, assume bi-
zarre configurations, and even cause mass effect. Knowledge of the
signal intensity characteristics and locations of VR spaces helps differ-
entiate them from various pathologic conditions, including lacunar in-
farctions, cystic periventricular leukomalacia, multiple sclerosis, cryp-
tococcosis, mucopolysaccharidoses, cystic neoplasms, neurocysticerco-
sis, arachnoid cysts, and neuroepithelial cysts.
©
RSNA, 2007
Abbreviations: CSF ⫽ cerebrospinal fluid, FLAIR ⫽ fluid-attenuated inversion recovery, GAG ⫽ glycosaminoglycan, MS ⫽ multiple sclerosis,
VR ⫽ Virchow-Robin
RadioGraphics 2007; 27:1071–1086 ● Published online 10.1148/rg.274065722 ● Content Codes:
1From the Department of Radiology, University Medical Center Utrecht, Heidelberglaan 100, 3584 CX Utrecht, the Netherlands. Received July 25,
2006; revision requested October 24 and received November 30; accepted December 4. All authors have no financial relationships to disclose. Ad-
dress correspondence to R.M.K. (e-mail: rmkwee@gmail.com).
©
RSNA, 2007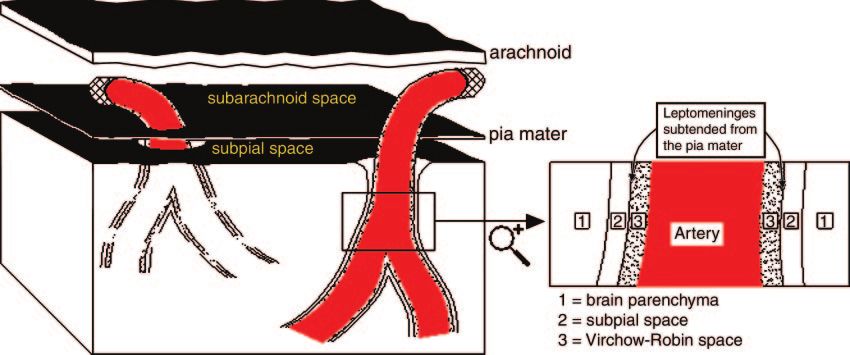
1072 July-August 2007 RG f Volume 27 ● Number 4
Introduction
The Virchow-Robin (VR) space is named after
Rudolf Virchow (German pathologist, 1821–
1902) (1) and Charles Philippe Robin (French
anatomist, 1821–1885) (2). VR spaces, or
perivascular spaces, surround the walls of vessels
as they course from the subarachnoid space
through the brain parenchyma. VR spaces are
commonly seen at magnetic resonance (MR) im-
aging and may sometimes be difficult to differen-
tiate from pathologic conditions. Knowledge of
their signal intensity characteristics and localiza-
tion helps in this differentiation, which is impor-
tant for correct patient management.
The purpose of this article is to provide an in-
depth overview of the MR imaging features of VR
spaces. Specific topics outlined are the micro-
scopic anatomy of VR spaces, dilated VR spaces,
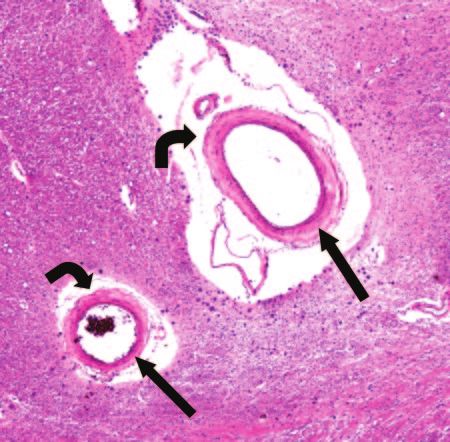
prevalence, and normal and atypical appearance Figure 1. Photomicrograph (original magnification,
of VR spaces. Subsequently, differential diagnos- ⫻20; hematoxylin-eosin stain) of a coronal section
through the anterior perforated substance shows two
tic considerations are discussed.
arteries (straight arrows) with surrounding VR spaces
(curved arrows).
Anatomy
VR spaces surround the walls of arteries, arte-
Teaching rioles, veins, and venules as they course from the space. The inner layer of leptomeninges closely
Point subarachnoid space through the brain paren- invests the adventitia of the vessel wall. The outer
chyma (Fig 1) (1–5). Electron microscopy and layer abuts on the glia limitans of the underlying
tracer studies have given insight into the location brain and is continuous with the pia mater on the
of VR spaces and clarified that the subarachnoid surface of the brain and the anterior perforated
space does not communicate directly with the VR substance. Veins in the basal ganglia have no
spaces (3–5). outer layer of leptomeninges (similar to cortical
Arteries in the cerebral cortex are coated by a veins), which suggests that their VR spaces are
layer of leptomeninges that is subtended from the continuous with the subpial space (5).
pia mater; by this anatomic arrangement, the VR Interstitial fluid within the brain parenchyma
spaces of the intracortical arteries are in direct drains from the gray matter of the brain by diffu-
continuity with the VR spaces around arteries in sion through the extracellular spaces and by bulk
the subarachnoid space (Fig 2). The lack of a flow along VR spaces. There is evidence from
similar coating of leptomeningeal cells around tracer studies and from pathologic analysis of the
veins in the cerebral cortex suggests that VR human brain that VR spaces carry solutes from
spaces around veins are in continuity with the the brain and are, in effect, the lymphatic drain-
subpial space (4). age pathways of the brain (6).
In contrast to arteries in the cerebral cortex,
arteries in the basal ganglia are surrounded by not Dilated VR Spaces
one but two distinct coats of leptomeninges, sepa- Dilatation of VR spaces was described by Durant-
rated by a VR space that is continuous with the Fardel (7) in 1843. These dilatations are regular
VR space around arteries in the subarachnoid cavities that always contain a patent artery. The
mechanisms underlying expanding VR spaces areRG f Volume 27 ● Number 4 Kwee and Kwee 1073
Figure 2. Drawing shows a cortical artery with a surrounding VR space crossing from the subarach-
noid and subpial spaces through the brain parenchyma. The magnified view on the right shows the ana-
tomic relationship between the artery, VR space, subpial space, and brain parenchyma.
still unknown. Different theories have been postu- The prevalence of VR spaces at MR imaging is
lated: segmental necrotizing angiitis of the arteries also dependent on the applied technique. Heavier
or another unknown condition causing perme- T2-weighted imaging results in better visualiza-
ability of the arterial wall (8 –10), expanding VR tion of VR spaces (23). In addition, the use of
spaces resulting from disturbance of the drainage thinner sections will demonstrate more VR spaces
route of interstitial fluid due to cerebrospinal fluid as well (15,24). Also, high-field-strength MR im-
(CSF) circulation in the cistern (11,12), spiral aging is expected to have an increased clinical
elongation of blood vessels and brain atrophy re- impact in the near future; the current magnetic
sulting in an extensive network of tunnels filled field (ⱕ1.5 T) is likely to be switched to 3 or 4 T.
with extracellular water (9,13), gradual leaking of The anticipated higher signal-to-noise ratio at
the interstitial fluid from the intracellular com- higher magnetic field strengths may successfully
partment to the pial space around the metarteri- improve spatial resolution and image contrast
ole through the fenestrae in the brain parenchyma (25–27), leading to better visualization (and in-
(14), and fibrosis and obstruction of VR spaces creased prevalence) of VR spaces on MR images.
along the length of arteries and consequent im-
pedance of fluid flow (5). Appearance at MR Imaging
Prevalence Signal Intensity Characteristics
Small VR spaces (⬍2 mm) appear in all age Visually, the signal intensities of the VR spaces Teaching
Teaching groups. With advancing age, VR spaces are found are identical to those of CSF with all pulse se- Point
Point with increasing frequency and larger apparent size quences. However, when signal intensities are
(⬎2 mm) (15). Some studies found a correlation measured, the VR spaces prove to have signifi-
between dilated VR spaces and neuropsychiatric cantly lower signal intensity than the CSF-con-
disorders (16 –19), recent-onset multiple sclerosis taining structures within and around the brain
(MS) (20), mild traumatic brain injury (21), and
diseases associated with microvascular abnormali-
ties (22).1074 July-August 2007 RG f Volume 27 ● Number 4
Figure 3. Bilateral type I VR spaces in a 6-year-old boy. (a) Axial proton-density–
weighted image (repetition time msec/echo time msec ⫽ 2375/100) shows hyperintense ar-
eas (arrows) in the anterior perforated substance on both sides. (b) Axial fluid-attenuated
inversion-recovery (FLAIR) image (6606/100) obtained at the same level shows that these
areas have CSF-like content (arrows). The signal intensity of the surrounding brain paren-
chyma is normal. (c, d) Diffusion-weighted image (2574/81; b factor ⫽ 1000 sec/mm2) (c)
and corresponding apparent diffusion coefficient map (d) show no restricted diffusion in
these areas (arrows).
(28), a finding consistent with the fact that the ages. VR spaces show no restricted diffusion on
VR spaces represent entrapments of interstitial diffusion-weighted images because they are com-
fluid. This difference in signal intensity can also municating compartments. T1-weighted images
be explained by partial volume effects, since a VR with substantial flow sensitivity may show high
space with accompanying vessel is smaller than signal intensity due to inflow effects, thereby
the contemporary volume of a voxel on MR im- helping confirm that one is indeed dealing with
VR spaces (29). VR spaces do not enhance with
contrast material. In patients with small to mod-
erate dilatations of the VR spaces (2–5 mm), theRG f Volume 27 ● Number 4 Kwee and Kwee 1075
Figure 4. Bilateral type I VR spaces in a
53-year-old woman. Coronal T1-weighted
image (500/30) shows symmetrical hypoin-
tense areas (arrows) in the anterior perfo-
rated substance.
Figure 5. Type II VR spaces in a 73-year-old woman. (a) Axial proton-density–weighted
image (2376/100) shows multiple hyperintense foci in the centrum semiovale in both hemi-
spheres. (b) On an axial FLAIR image (6614/100) obtained at the same level, the VR spaces
are seen as hypointense dots without any surrounding high signal intensity. Note the two
small lesions with a hypointense center and a hyperintense rim (arrows) in the left hemi-
sphere; these lesions are not VR spaces but old lacunar infarctions.
surrounding brain parenchyma generally has nor- striate arteries change direction from a lateral to a
mal signal intensity (30,31). dorsomedial path and are grouped closely to-
gether. A proximal VR space, containing several
Locations and Morphology vessels, is the resulting physiologic finding (33).
Teaching Dilated VR spaces typically occur in three charac- The second type (type II) can be found along
Point teristic locations. The first type (type I) is fre- the path of the perforating medullary arteries as
quently seen on MR images and appears along they enter the cortical gray matter over the high
the lenticulostriate arteries entering the basal gan- convexities and extend into the white matter (Figs
glia through the anterior perforated substance 5, 6) (15,32).
(Figs 3, 4) (15,32). Here, the tortuous lenticulo-1076 July-August 2007 RG f Volume 27 ● Number 4
Figure 6. Type II
dilated VR spaces in
a 6-year-old boy.
(a) Axial T2-
weighted image
(2620/100) shows
linear to punctate
hyperintense areas
around the occipital
horns, especially on
the left side (arrow).
(b) FLAIR image
(7572/100) obtained
at the same level
shows no abnormal
signal intensity (ar-
row), in accordance
with the fact that
these areas are true
VR spaces.
Figure 7. Type III
VR space in a 25-
year-old man. (a) Ax-
ial proton-density–
weighted image
(2620/100) shows a
hyperintense spot in
the brainstem (ar-
row). (b) Axial
FLAIR image (7292/
120) obtained at the
same level shows that
the spot has CSF-like
content without ab-
normal surrounding
signal intensity (ar-
row). These findings
confirm that the spot
is a VR space.
The third type (type III) appears in the mid- cumferential arteries originating from the upper
brain. In the lower midbrain, VR spaces at the basilar artery or proximal posterior cerebral artery
pontomesencephalic junction surround the pen- (23,34,35).
etrating branches of the collicular and accessory VR spaces are mostly seen as well-defined oval,
collicular arteries (Figs 7, 8). They are mainly rounded, or tubular structures, depending on the
located between the cerebral peduncles in the plane in which they are intersected. They have
axial plane and correspond to the level of the ten- smooth margins, commonly appear bilaterally,
torial margin as seen in coronal sections. In the and usually measure 5 mm or less (32).
upper midbrain, where the VR spaces are visible
at the mesencephalodiencephalic junction, they Atypical VR Spaces
appear along the posterior (interpeduncular) It is reported that clusters of type II enlarged VR
thalamoperforating artery or the paramedian mes- spaces may predominantly involve one hemi-
encephalothalamic artery and short and long cir- sphere (36). There are even reports that describe
the solely unilateral appearance of enlarged VR
spaces in the high convexity (37,38).RG f Volume 27 ● Number 4 Kwee and Kwee 1077
Figure 8. Type III VR spaces in a 68-year-old man. (a) Axial proton-density–weighted image (2382/100) shows
multiple punctate hyperintense areas in the brainstem (arrow). (b) Close-up T2-weighted image (4615/120) clearly
shows the fine punctate pattern. (c) Axial FLAIR image (6609/100) shows the CSF-like content of the dots (arrow).
No surrounding high signal intensity is seen. The typical configuration and the fact that no high signal intensity is
seen on the FLAIR image confirm that the dots are VR spaces.
Figure 9. Giant VR spaces in the mesencephalothalamic region in a 19-year-old man. (a, b) Axial (a) and sagit-
tal (b) T2-weighted images (5970/120) show a multicystic lesion in the mesencephalothalamic region. The lesion
extends from the left cerebral peduncle to the left thalamus. The content of the cysts is CSF-like. The adjacent brain
parenchyma has normal signal intensity. No solid components are identified. (c) Axial gadolinium-enhanced T1-
weighted image (478/18) shows no enhancement. The process has caused obstruction of the sylvian aqueduct, result-
ing in hydrocephalus. The size of the lesion and the degree of hydrocephalus were unchanged compared with the ap-
pearance on MR images obtained 2 years earlier.
Occasionally, VR spaces appear markedly en- VR spaces. These spaces most often appear as
Teaching larged, cause mass effect, and assume bizarre cys- clusters of variably sized cysts and are most com-
Point tic configurations that may be misinterpreted as mon in the mesencephalothalamic region (Fig 9),
other pathologic processes, most often a cystic in the territory of the paramedial mesencephalo-
neoplasm. As most of these giant VR spaces bor- thalamic artery, and in the cerebral white matter.
der a ventricle or subarachnoid space, reports of Giant VR spaces in the mesencephalothalamic
such cases (39 – 41) have offered an extensive dif- region may cause hydrocephalus by direct com-
ferential diagnosis that includes cystic neoplasms, pression of the third ventricle or the sylvian aque-
parasitic cysts, cystic infarctions, nonneoplastic duct (Fig 9), requiring surgical intervention
neuroepithelial cysts, and deposition disorders (8,11,42– 47).
such as mucopolysaccharidosis. Salzman et al
(42) presented a series of 37 patients with giant1078 July-August 2007 RG f Volume 27 ● Number 4
Figure 10. Chronic lacunar infarction of the pons in a 59-year-old man. (a) Axial proton-
density–weighted image (2200/100) shows a hyperintense lesion in the pons (arrow).
(b) Axial FLAIR image (6614/100) shows that the lesion has a hypointense center with a
hyperintense rim (arrow), an appearance that reflects gliosis.
Figure 11. Acute and chronic lacunar infarctions in a 66-year-old man. (a) Axial proton-density–weighted image
(2385/100) shows multiple high-signal-intensity lesions bilaterally in the basal ganglia, internal capsule, and thalamus
(arrows). The signal intensity of the periventricular white matter is abnormally increased. (b) Axial FLAIR image
(6608/100) shows multiple small high-signal-intensity lesions and hypointense lesions surrounded by hyperintense
rims in the same region (arrows). (c) Apparent diffusion coefficient map shows a recent infarction in the posterior
limb of the right internal capsule (arrow).
In one-half of cases, giant VR spaces that occur mal signal intensity stems from reactive gliosis
in the white matter may have surrounding signal surrounding the enlarged VR spaces and is not an
intensity abnormality on T2-weighted or FLAIR ominous finding (47).
images (42). This may be viewed as a worrisome
finding and in some cases has prompted the per- Differential
formance of tissue biopsy. However, the abnor- Diagnostic Considerations
In this section, the top differential diagnoses of
dilated VR spaces are discussed. MR imaging
characteristics of each disease entity are summa-RG f Volume 27 ● Number 4 Kwee and Kwee 1079
Figure 12. Cystic periventricular leukomalacia in a 3-year-old boy with a history of perina-
tal asphyxia who had delayed motor and mental development and epilepsy. (a) Axial proton-
density–weighted image (2611/100) shows hyperintense lesions predominantly in the right
peritrigonal area (straight arrow) but also in the left peritrigonal area (curved arrow). These
lesions could be mistaken for type II VR spaces. (b) Coronal FLAIR image (11,000/140)
shows gliosis around the cystic lesions (arrows), a characteristic finding in end-stage cystic
periventricular leukomalacia.
rized, and clues to differentiate them from normal Lacunar infarctions can be differentiated from
VR spaces are given. VR spaces by signal intensity characteristics. An
acute lacunar infarction (12 hours up to 7 days)
Lacunar Infarctions appears as a small high-signal-intensity region on
Lacunar infarctions are small infarctions lying in T2-weighted and FLAIR images and as a hypoin-
deeper noncortical parts of the cerebrum and tense area on T1-weighted images. High signal
brainstem. They are caused by occlusion of pen- intensity is seen on diffusion-weighted images
etrating branches that arise from the middle cere- with corresponding low signal intensity on the
bral, posterior cerebral, and basilar arteries and apparent diffusion coefficient map (Fig 11). En-
less commonly from the anterior cerebral and ver- hancement is variable.
tebral arteries (48,49). Sites of predilection are A chronic lacunar infarction is better defined
the basal ganglia, thalamus, internal and external and has high signal intensity on T2-weighted im-
capsule, ventral pons, and periventricular white ages and low signal intensity on T1-weighted im-
matter (Figs 10, 11) (48). ages. On FLAIR images, a hyperintense lesion or
In the upper two-thirds of the anterior perfo- a lesion with a hypointense center and a hyperin-
rated substance and basal ganglia, cavities in tense rim reflecting gliosis is seen (Figs 10, 11).
brain specimens usually appear to be lacunar in- Diffusion-weighted images are normal. Enhance-
farctions. Large VR spaces found in the inferior ment may persist up to 8 weeks after the acute
third of the anterior perforated substance and event (51).
basal ganglia are invariably VR spaces around
branches of lenticulostriate arteries (type I VR Cystic Periventricular Leukomalacia
spaces) (32). Periventricular leukomalacia, usually seen in pre-
Lacunar infarctions tend to be larger than VR mature infants, is a leukoencephalopathy result-
spaces and often exceed 5 mm. However, no con- ing from a pre- or perinatal hypoxic-ischemic
sistent cutoff value with high diagnostic accuracy event. In the acute stage, white matter undergoes
has been reported in the literature, to our knowl- vascular congestion and coagulative necrosis.
edge. In contrast to VR spaces, lacunar infarc- Cavitation then occurs within necrotic regions.
tions are generally not symmetric (30,32,33,50). End-stage periventricular leukomalacia has a typi-
It is difficult to distinguish lacunar infarctions cal appearance at MR imaging (Fig 12): T2-
from VR spaces by means of shape. However, weighted and FLAIR images show abnormally
wedge-shaped holes are more likely to be lacunar
infarctions (50).1080 July-August 2007 RG f Volume 27 ● Number 4
Figure 13. Ovoid MS lesion of the centrum semiovale in a 49-year-old man. Axial proton-
density–weighted (2624/100) (a) and FLAIR (7291/120) (b) images show a hyperintense
lesion (arrow) in the right centrum semiovale. Other MS lesions were located behind the left
occipital horn and in the basal ganglia and brainstem.
increased signal intensity in the periventricular
white matter. There is marked loss of periven-
tricular white matter, predominantly in the peri-
atrial regions, and compensatory focal ventricular
enlargement adjacent to regions of abnormal
white matter signal intensity. The involvement
tends to be symmetrical. Corpus callosal thinning
can be seen as a secondary manifestation. There
is relative sparing of the overlying cortical mantle.
In more severe cases, cavitated infarcts have re-
placed the immediate periventricular white matter
(52,53). These cystic components have surround-
ing gliosis, easily depicted on FLAIR images,
which distinguishes them from enlarged VR
spaces (Fig 12).
Multiple Sclerosis Figure 14. Cryptococcosis in a 58-year-old
MS lesions may be located anywhere in the cen- woman with headaches and fever who was
tral nervous system. Lesions in the periventricular seropositive for human immunodeficiency
and juxtacortical white matter correspond to the virus. Parasagittal T2-weighted image (5963/
location of type II VR spaces. In addition, indi- 120) shows multiple dilated VR spaces in
the region of the basal ganglia (arrowheads).
vidual MS plaques often appear as ovoid lesions,
C neoformans was cultured from the CSF.
mimicking the shape of dilated VR spaces (Fig
13). However, MS lesions are usually arranged
like fingers pointing away from the walls of the images. T2-weighted and FLAIR images demon-
lateral ventricles (Dawson fingers) and can easily strate hyperintense lesions. Both solid and ring
be distinguished from enlarged VR spaces by sig- enhancement may occur. Enhancement is depen-
nal intensity characteristics. In the acute stage, dent on the current degree of inflammation (54).
MS lesions are isointense or mildly hypointense
to brain parenchyma on T1-weighted images. In Cryptococcosis
the chronic phase, they have a hypointense center Cryptococcosis is an opportunistic fungal infec-
with a mildly hyperintense rim on T1-weighted tion caused by Cryptococcus neoformans, affecting
the central nervous system in human immunode-RG f Volume 27 ● Number 4 Kwee and Kwee 1081
Figure 15. Hurler syndrome (mucopolysaccharidosis type I) in a 2-year-old boy with typi-
cal external features of this syndrome. A classic Hurler mutation with severe ␣-l-iduronidase
deficiency was demonstrated. (a) Axial proton-density–weighted image (3835/150) shows
dilated VR spaces in both hemispheres (arrowheads). (b) Coronal FLAIR image (6381/100)
shows increased signal intensity in the surrounding brain parenchyma (arrows); this finding
indicates that the spaces are not normally dilated VR spaces. There is also increased CSF
space frontally.
ficiency virus–seropositive patients and in patients hyperintense, making it possible to differentiate
with other immunocompromised states. Central them from normal VR spaces. Contrast enhance-
nervous system infection can be either meningeal ment is uncommon (58). On diffusion-weighted
or parenchymal. Infection usually starts as menin- images, there may be restricted diffusion in some
gitis, most pronounced at the base of the brain of the lesions due to the high viscosity of their
(55,56). The infection often provokes little in- contents.
flammatory reaction, owing to the host’s immu-
nity and to the immunosuppressive effect of the Mucopolysaccharidoses
organism’s capsule (55–57). Infection of the me- The mucopolysaccharidoses are inherited disor-
ninges may spread to the adjacent brain through ders of metabolism characterized by enzyme defi-
the subarachnoid space or along the ependymal ciency and inability to break down glycosamino-
surface. glycan (GAG), which results in the accumulation
As the infection spreads along the VR spaces, of toxic intracellular substrate. Clinical features
they may become distended with mucoid, gelati- are mental and motor retardation, macrocephaly,
nous material that originates from the organism’s and musculoskeletal deformities. The urinary
capsule (56). Therefore, cryptococcosis should be GAG level is elevated. Brain atrophy and abnor-
considered in the differential diagnosis in any malities of the white matter may be present.
immunocompromised patient with dilated VR Typically, the VR spaces are dilated by accu-
spaces. Larger collections of organisms and gelati- mulated GAG, which results in a cribriform ap-
nous capsular material in the VR spaces have pearance of the white matter, corpus callosum,
been termed gelatinous pseudocysts (55,56). and basal ganglia on T1-weighted images. Oc-
Mass lesions representing cryptococcomas may casionally, arachnoid cysts (due to meningeal
occur, particularly in the deep gray matter (55). GAG deposition) are seen. On T2-weighted and
Imaging findings are primarily manifestations FLAIR images, the dilated VR spaces are isoin-
of meningitis. Hydrocephalus often develops as a tense to CSF (Fig 15). However, the surrounding
result of the acute meningeal exudate and may white matter may show increased signal intensity,
also occur in the course of the infection because representing gliosis, edema, or de- or dysmyelina-
of meningeal adhesions. Punctate hyperintense tion (Fig 15). The latter helps in differentiating
areas representing dilated VR spaces or crypto- them from normal VR spaces. In addition, MR
coccomas are frequently seen in the basal ganglia,
thalami, and midbrain on T2-weighted images
(Fig 14) (55,56). On FLAIR images they are also1082 July-August 2007 RG f Volume 27 ● Number 4
Figure 16. Desmoplastic pilocytic astrocytoma of the right thalamus, cerebral peduncle, and brainstem in a 15-
year-old girl. (a, b) Axial proton-density–weighted (2374/100) (a) and FLAIR (6614/100) (b) images show a large
mass with solid (arrow) and cystic (arrowheads) components. (c) Axial gadolinium-enhanced T1-weighted image
(598/18) shows inhomogeneous enhancement of the solid component (arrow) and rim enhancement of the cystic
components (arrowheads). Obstruction of the third ventricle has caused hydrocephalus.
spectroscopy shows a broad peak around 3.7 ppm Neurocysticercosis
(higher than the chemical shift of myoinositol), Cysticercosis is the most common parasitic infec-
considered to contain signals from accumulated tion of the central nervous system, caused by the
GAG (59 – 61). larval stage of the pork tapeworm Taenia solium.
Fluid-filled oval cysts with an internal scolex (cys-
Cystic Neoplasms ticerci) may be located in the brain parenchyma
Giant dilatations of the VR spaces may cause (gray-white matter junction, but also in the basal
mass effect and assume bizarre configurations ganglia, cerebellum, and brainstem), subarach-
that may be misinterpreted as a cystic brain tu- noid space, ventricles, or spinal cord.
mor (39 – 42). However, cystic brain tumors often MR imaging findings of neurocysticercosis are
have solid components, may enhance with con- variable, depending on the stage of evolution of
trast material, mostly show surrounding edema, the infection. Lesions can be seen at different
and have contents that usually are not equal to stages in the same patient.
CSF, as can be seen on FLAIR images (Fig 16). In the initial vesicular stage, a cystic lesion is
They generally exhibit low signal intensity on dif- isointense to CSF with all MR sequences, resem-
fusion-weighted images with corresponding high bling an enlarged VR space. However, a discrete
apparent diffusion coefficient values (62– 64). eccentric scolex (hyperintense to CSF) may be
When the lesions in question occur in a character- seen (Fig 17). In general, the lesions do not en-
istic location along the path of a penetrating hance in this stage.
vessel, follow CSF signal intensity with all se- In the colloidal vesicular stage, the cyst is
quences, do not enhance with contrast material, mildly hyperintense to CSF. Mild to marked sur-
and have normal adjacent brain parenchyma, rounding edema may be seen. A thick cyst wall
their appearance is virtually always pathogno- enhances, including the scolex.
monic of giant VR spaces (Fig 9) (42). Still, dif- In the granular nodular stage, a thickened re-
ferentiation between giant VR spaces and cystic tracted cyst wall is seen, which may have nodular
brain tumors is sometimes difficult and follow-up or ring enhancement. Edema decreases.
MR imaging may be useful. In the nodular calcified stage, the lesion is
shrunken and completely calcified, appearing hy-
pointense with all MR sequences. Gradient-echoRG f Volume 27 ● Number 4 Kwee and Kwee 1083
Figure 17. Parenchymal neurocysticercosis
in the vesicular stage in a 17-year-old boy.
Axial T1-weighted image (605/18) shows a
Figure 19. Neuroepithelial cyst of the thala-
cystic lesion with an eccentrically located
mus in a 53-year-old woman with migraine
scolex (arrow), a finding pathognomonic of
headaches. Axial FLAIR image (7291/120)
neurocysticercosis.
shows a multiloculated cyst with CSF-like
signal intensity in the right thalamus (arrow).
The adjacent brain parenchyma has normal
signal intensity. Note that this lesion could
also be an enlarged VR space. A final diagno-
sis can be made with certainty only after
pathologic study.
tentorial locations for an arachnoid cyst are the
middle cranial fossa, the perisellar cisterns (Fig
18), and the subarachnoid space over the con-
vexities. On MR images, arachnoid cysts appear
as well-defined nonenhancing masses that are
isointense to CSF with all sequences, including
diffusion-weighted imaging (68). They can be
differentiated from enlarged VR spaces by their
typical location.
Neuroepithelial Cysts
Neuroepithelial cysts are rare and benign lesions,
mostly asymptomatic. Their etiology is controver-
Figure 18. Arachnoid cyst in the perisellar sial but developmental anomalies are likely. Le-
cistern area in a 16-year-old girl. Axial FLAIR sions are spherical to ovoid, measure up to several
image (7292/120) shows a well-defined, centimeters in size, and may have mass effect.
round cyst with CSF-like content in the su-
They are lined with thin epithelium and have a
prasellar cistern (arrow).
CSF-like content. On the basis of pathologic
studies, neuroepithelial cysts are regarded as
sequences are very useful to demonstrate the cal- ependymal in origin (69). Neuroepithelial cysts
cified scolex (65– 67). may involve the lateral ventricles or fourth ven-
tricle, with which they do not communicate (in-
Arachnoid Cysts traventricular cysts). They can also be found
Arachnoid cysts represent intra-arachnoid CSF– within the cerebral hemispheres, thalamus
containing cysts that do not communicate with (Fig 19), midbrain, pons (Fig 20), and cerebellar
the ventricular system. The most common supra-1084 July-August 2007 RG f Volume 27 ● Number 4
Figure 20. Neuroepithelial cyst of the cerebral peduncle and pons in a 60-year-old woman
with epilepsy. Axial T1-weighted (30/13) (a) and coronal FLAIR (11,000/140) (b) images
show a cyst with CSF-like content in the left cerebral peduncle (arrow). The adjacent tissue
has normal signal intensity. The cyst has a diameter of 15.7 mm as measured on the coronal
FLAIR image (b). This benign lesion probably represents a neuroepithelial cyst, although it
could also be a huge VR space.
Figure 21. Choroidal fissure cyst in a
1-week-old boy. Axial T1-weighted spec-
tral presaturation inversion-recovery image
(5094/30) shows a medial temporal lobe
cyst with CSF-like content arising in the
choroidal fissure (arrow).
vermis and in the medial temporal lobe in or near
the choroidal fissure (choroidal fissure cysts) (Fig
21) (70,71).
MR imaging confirms the CSF-like signal be-
havior of the cyst with all sequences and allows
exclusion of adjacent brain edema, soft-tissue
mass, and gliosis in or around the cyst. There is
no enhancement with contrast material (70,71).
Differentiation between neuroepithelial cysts and
enlarged VR spaces can be made with certainty
only by pathologic study.
Conclusions References
1. Virchow R. Ueber die Erweiterung kleinerer Ge-
VR spaces surround the walls of the vessels as faesse. Archiv Pathol Anat Physiol Klin Med 1851;
they course from the subarachnoid space through 3:427– 462.
the brain parenchyma. They can be seen on MR 2. Robin C. Recherches sur quelques particularités
images in all age groups. They may become mark- de la structure des capillaires de l’encephale.
edly enlarged. Knowledge of their signal intensity J Physiol Homme Anim 1859;2:537–548.
3. Hutchings M, Weller RO. Anatomical relation-
characteristics and localization helps in differenti- ships of the pia mater to cerebral blood vessels in
ating them from different pathologic conditions. man. J Neurosurg 1986;65:316 –325.
4. Zhang ET, Inman CB, Weller RO. Interrelation-
ship of the pia mater and the perivascular (Vir-
chow-Robin) spaces in the human cerebrum. J
Anat 1990;170:111–123.RG f Volume 27 ● Number 4 Kwee and Kwee 1085
5. Pollock H, Hutchings M, Weller RO, Zhang ET. 22. Patankar TF, Mitra D, Varma A, Snowden J,
Perivascular spaces in the basal ganglia of the hu- Neary D, Jackson A. Dilatation of the Virchow-
man brain: their relationship to lacunes. J Anat Robin space is a sensitive indicator of cerebral mi-
1997;191:337–346. crovascular disease: study in elderly patients with
6. Schley D, Carare-Nnadi R, Please CP, Perry VH, dementia. AJNR Am J Neuroradiol 2005;26:
Weller RO. Mechanisms to explain the reverse 1512–1520.
perivascular transport of solutes out of the brain. J 23. Saeki N, Sato M, Kubota M, et al. MR imaging of
Theor Biol 2006;238:962–974. normal perivascular space expansion at midbrain.
7. Durant-Fardel M. Traite du ramollissement du AJNR Am J Neuroradiol 2005;26:566 –571.
cerveau. Paris, France: Balliere, 1843. 24. Song CJ, Kim JH, Kier EL, Bronen RA. MR im-
8. Poirier J, Barbizet J, Gaston A, Meyrignac C. Tha- aging and histologic features of subinsular bright
lamic dementia: expansive lacunae of the thalamo- spots on T2-weighted MR images: Virchow-Robin
paramedian mesencephalic area— hydrocephalus spaces of the extreme capsule and insular cortex.
caused by stenosis of the aqueduct of Sylvius [in Radiology 2000;214:671– 677.
French]. Rev Neurol (Paris) 1983;139:349 –358. 25. Takahashi M, Uematsu H, Hatabu H. MR imag-
9. Benhaiem-Sigaux N, Gray F, Gherardi R, Roucay- ing at high magnetic fields. Eur J Radiol 2003;46:
rol AM, Poirier J. Expanding cerebellar lacunes 45–52.
due to dilatation of the perivascular space associ- 26. Uematsu H, Dougherty L, Takahashi M, et al. A
ated with Binswanger’s subcortical arteriosclerotic direct comparison of signal behavior between 4.0
encephalopathy. Stroke 1987;18:1087–1092. and 1.5 T: a phantom study. Eur J Radiol 2003;
10. Hughes W. Origin of lacunes. Lancet 1965;2:19 – 45:154 –159.
21. 27. Sasaki M, Inoue T, Tohyama K, Oikawa H, Ehara
11. Homeyer P, Cornu P, Lacomblez L, Chiras J, S, Ogawa A. High-field MRI of the central ner-
Derouesne C. A special form of cerebral lacunae: vous system: current approaches to clinical and
expanding lacunae. J Neurol Neurosurg Psychiatry microscopic imaging. Magn Reson Med Sci 2003;
1996;61:200 –202. 2:133–139.
12. Mascalchi M, Salvi F, Godano U, et al. Expand- 28. Ozturk MH, Aydingoz U. Comparison of MR sig-
ing lacunae causing triventricular hydrocephalus: nal intensities of cerebral perivascular (Virchow-
report of two cases. J Neurosurg 1999;91:669 – Robin) and subarachnoid spaces. J Comput Assist
674. Tomogr 2002;26:902–904.
13. Awad IA, Johnson PC, Spetzler RF, Hodak JA. 29. Hirabuki N, Fujita N, Fujii K, Hashimoto T, Ko-
Incidental subcortical lesions identified on mag- zuka T. MR appearance of Virchow-Robin spaces
netic resonance imaging in the elderly. II. Post- along lenticulostriate arteries: spin-echo and two-
mortem pathological correlations. Stroke 1986;17: dimensional fast low-angle shot imaging. AJNR
1090 –1097. Am J Neuroradiol 1994;15:277–281.
14. Adachi M, Hosoya T, Haku T, Yamaguchi K. Di- 30. Braffman BH, Zimmerman RA, Trojanowski JQ,
lated Virchow-Robin spaces: MRI pathological Gonatas NK, Hickey WF, Schlaepfer WW. Brain
study. Neuroradiology 1998;40:27–31. MR: pathologic correlation with gross and histo-
15. Heier LA, Bauer CJ, Schwartz L, Zimmerman pathology. 1. Lacunar infarction and Virchow-
RD, Morgello S, Deck MD. Large Virchow-Robin Robin spaces. AJR Am J Roentgenol 1988;151:
spaces: MR-clinical correlation. AJNR Am J Neu- 551–558.
roradiol 1989;10:929 –936. 31. Demaerel P, Wilms G, Baert AL, Van den Bergh
16. Rollins NK, Deline C, Morriss MC. Prevalence V, Sainte T. Widening of Virchow-Robin spaces.
and clinical significance of dilated Virchow-Robin AJNR Am J Neuroradiol 1996;17:800 – 801.
spaces in childhood. Radiology 1993;189:53–57. 32. Jungreis CA, Kanal E, Hirsch WL, Martinez AJ,
17. Machado MA Jr, Matos AS, Goyanna F, Barbosa Moossy J. Normal perivascular spaces mimicking
VA, Vieira LC. Dilatation of Virchow-Robin lacunar infarction: MR imaging. Radiology 1988;
spaces in patients with migraine [in Portuguese]. 169:101–104.
Arq Neuropsiquiatr 2001;59:206 –209. 33. Pullicino PM, Miller LL, Alexandrov AV, Ostrow
18. MacLullich AM, Wardlaw JM, Ferguson KJ, Starr PT. Infraputaminal ‘lacunes’: clinical and patho-
JM, Seckl JR, Deary IJ. Enlarged perivascular logical correlations. Stroke 1995;26:1598 –1602.
spaces are associated with cognitive function in 34. Elster AD, Richardson DN. Focal high signal on
healthy elderly men. J Neurol Neurosurg Psychia- MR scans of the midbrain caused by enlarged
try 2004;75:1519 –1523. perivascular spaces: MR-pathologic correlation.
19. Taber KH, Shaw JB, Loveland KA, Pearson DA, AJR Am J Roentgenol 1991;156:157–160.
Lane DM, Hayman LA. Accentuated Virchow- 35. Duvernoy HM. Human brainstem vessels. Berlin,
Robin spaces in the centrum semiovale in children Germany: Springer-Verlag, 1978; 16 – 66.
with autistic disorder. J Comput Assist Tomogr 36. Ogawa T, Okudera T, Fukasawa H, et al. Unusual
2004;28:263–268. widening of Virchow-Robin spaces: MR appear-
20. Achiron A, Faibel M. Sandlike appearance of Vir- ance. AJNR Am J Neuroradiol 1995;16:1238 –
chow-Robin spaces in early multiple sclerosis: a 1242.
novel neuroradiologic marker. AJNR Am J Neuro- 37. Sawada M, Nishi S, Hashimoto N. Unilateral ap-
radiol 2002;23:376 –380. pearance of markedly dilated Virchow-Robin
21. Inglese M, Bomsztyk E, Gonen O, Mannon LJ, spaces. Clin Radiol 1999;54:334 –336.
Grossman RI, Rusinek H. Dilated perivascular
spaces: hallmarks of mild traumatic brain injury.
AJNR Am J Neuroradiol 2005;26:719 –724.1086 July-August 2007 RG f Volume 27 ● Number 4
38. Shiratori K, Mrowka M, Toussaint A, Spalke G, 56. Tien RD, Chu PK, Hesselink JR, Duberg A,
Bien S. Extreme, unilateral widening of Virchow- Wiley C. Intracranial cryptococcosis in immuno-
Robin spaces: case report. Neuroradiology 2002; compromised patients: CT and MR findings in 29
44:990 –992. cases. AJNR Am J Neuroradiol 1991;12:283–289.
39. Davis G, Fitt GJ, Kalnins RM, Mitchell LA. In- 57. Wehn SM, Heinz ER, Burger PC, Boyko OB. Di-
creased perivascular spaces mimicking frontal lobe lated Virchow-Robin spaces in cryptococcal men-
tumor. J Neurosurg 2002;97:723. ingitis associated with AIDS: CT and MR find-
40. Romi F, Tysnes OB, Krakenes J, Savoiardo M, ings. J Comput Assist Tomogr 1989;13:756 –762.
Aarli JA, Bindoff L. Cystic dilation of Virchow- 58. Miszkiel KA, Hall-Craggs MA, Miller RF, et al.
Robin spaces in the midbrain. Eur Neurol 2002; The spectrum of MRI findings in CNS cryptococ-
47:186 –188. cosis in AIDS. Clin Radiol 1996;51:842– 850.
41. Cakirer S. MR imaging findings in tumefactive 59. Lee C, Dineen TE, Brack M, Kirsch JE, Runge
perivascular spaces. Acta Radiol 2003;44:673– VM. The mucopolysaccharidoses: characterization
674. by cranial MR imaging. AJNR Am J Neuroradiol
42. Salzman KL, Osborn AG, House P, et al. Giant 1993;14:1285–1292.
tumefactive perivascular spaces. AJNR Am J Neu- 60. Matheus MG, Castillo M, Smith JK, Armao D,
roradiol 2005;26:298 –305. Towle D, Muenzer J. Brain MRI findings in pa-
43. Kanamalla US, Calabro R, Jinkins JR. Cavernous tients with mucopolysaccharidosis types I and II
dilatation of mesencephalic Virchow-Robin spaces and mild clinical presentation. Neuroradiology
with obstructive hydrocephalus. Neuroradiology 2004;46:666 – 672.
2000;42:881– 884. 61. Takahashi Y, Sukegawa K, Aoki M, et al. Evalua-
44. Papayannis CE, Saidon P, Rugilo CA, et al. Ex- tion of accumulated mucopolysaccharides in the
panding Virchow Robin spaces in the midbrain brain of patients with mucopolysaccharidoses by
causing hydrocephalus. AJNR Am J Neuroradiol (1)H-magnetic resonance spectroscopy before and
2003;24:1399 –1403. after bone marrow transplantation. Pediatr Res
45. Rohlfs J, Riegel T, Khalil M, et al. Enlarged 2001;49:349 –355.
perivascular spaces mimicking multicystic brain 62. Tien RD, Felsberg GJ, Friedman H, Brown M,
tumors: report of two cases and review of the lit- MacFall J. MR imaging of high-grade cerebral
erature. J Neurosurg 2005;102:1142–1146. gliomas: value of diffusion-weighted echoplanar
46. Longatti PL, Fiorindi A, Carteri A, Caroli F, Mar- pulse sequences. AJR Am J Roentgenol 1994;162:
tinuzzi A. Expanding cerebral cysts (lacunae): a 671– 677.
treatable cause of progressive midbrain syndrome. 63. Noguchi K, Watanabe N, Nagayoshi T, et al. Role
J Neurol Neurosurg Psychiatry 2003;74:393–394. of diffusion-weighted echo-planar MRI in distin-
47. House P, Salzman KL, Osborn AG, MacDonald guishing between brain abscess and tumour: a pre-
JG, Jensen RL, Couldwell WT. Surgical consider- liminary report. Neuroradiology 1999;41:171–
ations regarding giant dilations of the perivascular 174.
spaces. J Neurosurg 2004;100:820 – 824. 64. Desprechins B, Stadnik T, Koerts G, Shabana W,
48. Fisher CM. Lacunes: small, deep cerebral infarcts. Breucq C, Osteaux M. Use of diffusion-weighted
Neurology 1965;15:774 –784. MR imaging in differential diagnosis between in-
49. Fisher CM. Lacunar strokes and infarcts: a review. tracerebral necrotic tumors and cerebral abscesses.
Neurology 1982;32:871– 876. AJNR Am J Neuroradiol 1999;20:1252–1257.
50. Bokura H, Kobayashi S, Yamaguchi S. Distin- 65. do Amaral LL, Ferreira RM, da Rocha AJ, Fer-
guishing silent lacunar infarction from enlarged reira NP. Neurocysticercosis: evaluation with ad-
Virchow-Robin spaces: a magnetic resonance im- vanced magnetic resonance techniques and atypi-
aging and pathological study. J Neurol 1998;245: cal forms. Top Magn Reson Imaging 2005;16:
116 –122. 127–144.
51. Regli L, Regli F, Maeder P, Bogousslavsky J. Mag- 66. Dumas JL, Visy JM, Belin C, Gaston A, Goldlust
netic resonance imaging with gadolinium contrast D, Dumas M. Parenchymal neurocysticercosis:
agent in small deep (lacunar) cerebral infarcts. follow-up and staging by MRI. Neuroradiology
Arch Neurol 1993;50:175–180. 1997;39:12–18.
52. Baker LL, Stevenson DK, Enzmann DR. End- 67. Noujaim SE, Rossi MD, Rao SK, et al. CT and
stage periventricular leukomalacia: MR evalua- MR imaging of neurocysticercosis. AJR Am J
tion. Radiology 1988;168:809 – 815. Roentgenol 1999;173:1485–1490.
53. Flodmark O, Lupton B, Li D, et al. MR imaging 68. Van Tassel P, Cure JK. Nonneoplastic intracranial
of periventricular leukomalacia in childhood. AJR cysts and cystic lesions. Semin Ultrasound CT
Am J Roentgenol 1989;152:583–590. MR 1995;16:186 –211.
54. Pretorius PM, Quaghebeur G. The role of MRI in 69. Andrews BT, Halks-Miller M, Berger MS, Rosen-
the diagnosis of MS. Clin Radiol 2003;58:434 – blum ML, Wilson CB. Neuroepithelial cysts of the
448. posterior fossa: pathogenesis and report of two
55. Mathews VP, Alo PL, Glass JD, Kumar AJ, cases. Neurosurgery 1984;15:91–95.
McArthur JC. AIDS-related CNS cryptococcosis: 70. Guermazi A, Miaux Y, Majoulet JF, Lafitte F,
radiologic-pathologic correlation. AJNR Am J Chiras J. Imaging findings of central nervous sys-
Neuroradiol 1992;13:1477–1486. tem neuroepithelial cysts. Eur Radiol 1998;8:618 –
623.
71. Sherman JL, Camponovo E, Citrin CM. MR im-
aging of CSF-like choroidal fissure and parenchy-
mal cysts of the brain. AJNR Am J Neuroradiol
1990;11:939 –945.RG Volume 27 • Volume 4 • July-August 2007 Kwee and Kwee Virchow-Robin Spaces at MR Imaging Robert M. Kwee, MD, and Thomas C. Kwee, MD RadioGraphics 2007; 27:1071–1086 ● Published online 10.1148/rg.274065722 ● Content Codes: Page 1072 VR spaces surround the walls of arteries, arterioles, veins, and venules as they course from the subarachnoid space through the brain parenchyma (Fig 1) (1–5). Page 1073 Small VR spaces (2 mm) (15). Page 1073 Visually, the signal intensities of the VR spaces are identical to those of CSF with all pulse sequences. Page 1075 Dilated VR spaces typically occur in three characteristic locations. Page 1077 Occasionally, VR spaces appear markedly enlarged, cause mass effect, and assume bizarre cystic configurations that may be misinterpreted as other pathologic processes, most often a cystic neoplasm.
You can also read

















































