TARGETED DRUG DELIVERY FOR LIVER CANCER: Ghent ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
TARGETED DRUG DELIVERY FOR LIVER CANCER: experimental evaluation of the flow and Sir-spheres distribution in a patient specific model CHARLOTTE CLAEREBOUT Student number: 01509279 Supervisors: Prof. Dr. Ir. Charlotte Debbaut, Prof. Dr. Ir. Patrick Segers Counsellors: Ghazal Adeli Koudehi, Tim Bomberna A dissertation submitted to Ghent University in partial fulfilment of the requirements for the degree of Master of Medicine in Medicine Academic year: 2018 – 2020
Acknowledgment First and foremost, I would like to express my gratitude to my promotors prof. Charlotte Debbaut and prof. Patrick Segers. I would like to thank especially prof. Debbaut for her guidance and support throughout this master thesis. I would also like to thank Ghazal Adeli Koudehi whom I could always contact for questions and tips. I also would like to thank Jurgen Deviche for his guidance. In addition I would sincerely like to thank Tim Bomberna for all his help and work. He was always readily available for questions and help. I would also like to thank my father, Edwin Claerebout, for his support and guidance. I also want to thank him, Nathalie De Wilde and Stijn Casaert of the Faculty of Veterinary Medicine from Ghent University in Merelbeke (Belgium) for their help. Last but not least, I would like to thank my family and friends. I could not have done this without their support, encouragement, understanding and love. I

Deze pagina is niet beschikbaar omdat ze persoonsgegevens bevat. Universiteitsbibliotheek Gent, 2021. This page is not available because it contains personal information. Ghent University, Library, 2021.

Table of contents Contents Acknowledgment ............................................................................................................................................. I Table of contents............................................................................................................................................. II Abstract ........................................................................................................................................................... 1 Samenvatting .................................................................................................................................................. 2 1 Introduction............................................................................................................................................. 3 1.1 Hepatocellular carcinoma ............................................................................................................... 3 1.1.1 Epidemiology ........................................................................................................................... 3 1.1.2 Risk factors .............................................................................................................................. 3 1.1.3 Pathogenesis ........................................................................................................................... 5 1.1.4 Symptoms ................................................................................................................................ 5 1.1.5 Surveillance ............................................................................................................................. 5 1.1.6 Diagnosis ................................................................................................................................. 6 1.1.7 Treatment................................................................................................................................ 7 1.2 Search for optimizing the transarterial embolotherapy ............................................................... 18 1.3 Goal of this master thesis .............................................................................................................. 21 2 Methods ................................................................................................................................................ 21 2.1 Data of the cirrhotic liver .............................................................................................................. 21 2.1.1 Vascular corrosion casting and Micro-CT imaging ................................................................ 22 2.2 Geometry segmentation ............................................................................................................... 22 2.3 Creation of the 3D printed model ................................................................................................. 23 2.4 Lab experiments ............................................................................................................................ 25 2.4.1 Experimental setup ............................................................................................................... 25 2.4.2 Experimental method............................................................................................................ 26 3 Results ................................................................................................................................................... 28 3.1 Flow distribution ........................................................................................................................... 28 3.1.1 Setup without a tumor .......................................................................................................... 28 3.1.2 Setup with a large tumor in the left lobe .............................................................................. 31 3.2 Particle distribution ....................................................................................................................... 34 3.2.1 Setup without a tumor .......................................................................................................... 35 3.2.2 Setup with a large tumor in the left lobe .............................................................................. 37 II
3.3 Comparison between experimental particle and flow distribution .............................................. 39 4 Discussion .............................................................................................................................................. 41 4.1 Limitations of the experimental setup .......................................................................................... 41 4.2 Comparison between experimental and computational flow and particle distribution .............. 42 4.2.1 Comparison between experimental and computational flow distribution .......................... 42 4.2.2 Comparison between experimental and computational particle distribution ..................... 43 4.3 Comparison between experimental particle and flow distribution .............................................. 45 4.4 Points for improvement ................................................................................................................ 46 5 Conclusion ............................................................................................................................................. 48 References ..................................................................................................................................................... 49 Attachments .................................................................................................................................................... a III
Abstract Hepatocellular carcinoma (HCC) is the third most common cause of cancer-related deaths and has a rapidly growing incidence. HCC is most commonly staged according the Barcelona Clinic Liver Cancer (BCLC) staging system and divides HCC in five cancer stages (very early stage, early stage, intermediate stage, advanced stage, and end stage). Transarterial embolization therapy is the preferred treatment for patients with intermediate-stage HCC. The normal hepatic parenchyma has a dual blood supply, with predominant supply from the portal vein and less from the hepatic artery. HCC tumors have an almost complete supply from the hepatic artery, which means that transarterial therapies can target the tumors more specifically while sparing normal parenchyma. In the transarterial therapy, a selective catheter delivers particles (vaso-occlusive materials, chemotherapeutic agents, radioembolizers, etc.) into the tumor supplying arteries. Although transarterial therapies show improvement of the prognosis of intermediate HCC, the treatment still needs to be optimized. One of the challenges to increase the efficiency of transarterial therapies is to target only the target tumor, without targeting the healthy liver parenchyma. A personalized intervention with pretreatment computational modelling could be used to simulate the particle distribution in the patient-specific hepatic vasculature and determine the effect of certain parameters on this particle distribution. The aim of this master thesis is to evaluate the accuracy of the computational prediction of the particle distribution and the effect of two parameters on the particle trajectory and distribution in the liver. The two evaluated parameters were the tumor burden and the method of particle administration. The two different manners of particle administration were injecting the particles in a side branch of the hepatic artery and mixing the particles in the main reservoir through which the particles flowed through the experimental set-up together with the water. By creating three-dimensional reconstructions and a 3D print of the arterial vascularity of the patient’s liver, the experimental flow and particle distribution in this 3D model were considered in 4 different cases (2 cases without a tumor: one with particle injection and one with particles in the main reservoir, and 2 cases with a large tumor in the left lobe: one with particle injection and one with particles in the main reservoir). Afterwards the experimental flow and particle distribution were compared to each other and to the computational flow and particle distribution from Tim Bomberna’s master thesis. The results show that the tumor burden has a major impact on the flow and particle distribution while the method of particle administration doesn’t have a significant impact on the particle distribution. Furthermore, the computational prediction of the particle distribution showed to be an accurate tool for predicting the particle trajectories which can help choosing the correct radial position of the catheter tip to selectively target the tumor. 1

Samenvatting Hepatocellulair carcinoom (HCC) is de derde meest voorkomende oorzaak van kanker gerelateerde sterfte en heeft een snel toenemende incidentie. HCC wordt meestal gestadiëerd volgens het Barcelona Clinic Liver Cancer (BCLC) stadiëringssysteem en verdeelt HCC in vijf kanker stadia (zeer vroeg stadium, vroeg stadium, intermediair stadium, vergevorderd stadium en eindstadium). Transarteriële embolisatie therapie is de voorkeursbehandeling voor patiënten met intermediair HCC. Het normale leverparenchym heeft een dubbele bloedtoevoer, met overheersende toevoer vanuit de poortader en minder vanuit de leverslagader. HCC-tumoren hebben een bijna volledige toevoer uit de leverslagader, wat betekent dat transarteriële therapieën de tumor specifieker kunnen treffen terwijl ze het normale parenchym sparen. Bij de transarteriële therapie levert een selectieve katheter deeltjes (vaso-occlusieve materialen, chemotherapeutische middelen, radio-embolizers, enz.) in de bloedvaten die de tumor voorzien. Hoewel transarteriële therapieën een verbetering van de prognose van intermediaire HCC laten zien, moet de behandeling nog worden geoptimaliseerd. Een van de uitdagingen om de efficiëntie van transarteriële therapieën te verhogen, is om te zorgen dat ze zich alleen op de doeltumor treffen, zonder het gezonde leverparenchym te treffen. Een gepersonaliseerde interventie met computermodellering vóór de behandeling kan worden gebruikt om de deeltjesverdeling in de patiëntspecifieke lever vasculatuur te simuleren en het effect van bepaalde parameters op deze deeltjesverdeling te bepalen. Het doel van deze masterproef is om de nauwkeurigheid van de computervoorspelling van de deeltjesverdeling en het effect van twee parameters op het deeltjestraject en -verdeling in de lever te evalueren. De twee geëvalueerde parameters waren de tumorgraad (grootte en aantal) en de methode voor het toedienen van deeltjes. De twee verschillende methoden voor het toedienen van deeltjes waren het injecteren van de deeltjes in een zijtak van de leverslagader enerzijds en het mengen van de deeltjes in het hoofdreservoir waardoor de deeltjes samen met het water door de experimentele opstelling stroomden anderzijds. Door driedimensionale reconstructies en een 3D-print van de arteriële vasculatuur van de lever van de patiënt te maken, werden de experimentele stroom- en deeltjesverdeling in dit 3D-model in 4 verschillende gevallen beschouwd (2 gevallen zonder tumor: één met deeltjesinjectie en één met deeltjes in het hoofdreservoir en 2 gevallen met een grote tumor in de linker lob: één met deeltjesinjectie en één met deeltjes in het hoofdreservoir). Daarna werden de experimentele stroom- en deeltjesverdeling met elkaar vergeleken en met de computer stroom- en deeltjesverdeling uit de masterproef van Tim Bomberna. 2
De resultaten laten zien dat de tumorbelasting een grote invloed heeft op de stroom en de deeltjesverdeling, terwijl de methode voor het toedienen van deeltjes geen significante invloed heeft op de deeltjesverdeling. Verder bleek de computer voorspelling van de deeltjesverdeling een nauwkeurig hulpmiddel voor het voorspellen van de deeltjestrajecten die kunnen helpen bij het kiezen van de juiste radiale positie van de kathetertip om selectief op de tumor te richten. 1 Introduction 1.1 Hepatocellular carcinoma 1.1.1 Epidemiology Hepatocellular carcinoma (HCC) is the third most common cause of cancer-related deaths (with an average of 700.000 deaths a year) and the sixth most common cancer worldwide (3, 4). It is the most common primary hepatic malignancy (90% of primary liver cancers) with rapidly growing incidence in Europe and the USA (4-8). In Europe the incidence rates go from less than 5/100.000 cases in Western Europe to 10/100.000 cases in Southern Europe. In North America, the incidence rates are similar to Southern Europe. The incidence of HCC in the United States is 35.000 cases per year (8). Around 3/100.000 persons in the USA have HCC (9). The incidence rates of HCC are the highest in Asia and Sub-Saharan Africa, with 20-35/100.000 cases. An important factor in the cause of these high incidence rates is the high prevalence of hepatitis B infection (8). The majority of HCC patients are diagnosed at intermediate or advanced stages which means that curative therapy (such as transplantation, ablation or surgical resection) is no longer possible (5- 7). For patients with unresectable HCC, there is currently no clinically proven standard for treatment (6). Unfortunately, most patients with a very advanced stage of HCC, which is untreatable, die within 3 to 6 months (3). 1.1.2 Risk factors The most common underlying cause of HCC is liver cirrhosis. Underlying cirrhosis is related in 75% to 85% of HCC (4). Cirrhosis can be caused by multiple conditions, from which chronic viral hepatitis, non-alcoholic fatty liver disease (NAFLD), alcoholic liver disease, and hemochromatosis are the most frequent (8, 10). In eastern Asia and sub-Saharan Africa, where 80% of the hepatocellular carcinoma cases occur, the main risk factors are aflatoxin B1 exposure (a fungal carcinogen present in food) and chronic hepatitis B (4). Hepatitis B virus infection (HBV) is a DNA virus that can induce insertional mutagenesis (8). The incidence of hepatocellular carcinoma in patients with hepatitis B increases with duration of infection (HBV infected cirrhotic patients have an annual risk of HCC development of 2%) (8), severity of the liver disease, and viral load. Occult hepatitis B infection also increases 3

the risk of HCC through DNA damage induced by virus integration (4). In Europe, the USA, and Japan, the main risk factors are hepatitis C virus (HCV) infection and excessive alcohol intake (4). Chronic alcohol abuse is a risk factor for the development of alcoholic fatty liver disease. Chronic alcohol abuse and diabetes have a synergistic effect with hepatitis B or C infections to induce HCC (11). HCV-infected cirrhotic patients have an annual risk of HCC development of 3-7% (8). Coinfection of either hepatitis B virus or hepatitis C virus with HIV (human immunodeficiency virus) may be associated with rapidly progressive liver disease, and cirrhosis development increases the risk of hepatocellular carcinoma (4). In the United States, the incidence and mortality of HCC have been increasing for the past 3 decades, with hepatitis C infection being the main cause. Hepatitis C virus infection, intravenous drug abuse and NAFLD cause an increase of the incidence rates of HCC across the globe (4). Moreover, the leading cause of HCC in developed countries is expected to become NAFLD. The incidence of NAFLD is rising, parallel to the rising epidemic of metabolic syndrome. Metabolic syndrome, diabetes and obesity are risk factors for the development of NAFLD. In cirrhotic NAFLD, male gender, underlying diabetes, hypertension and age over 70 are risk factors for developing HCC. NAFLD also contributes to non-cirrhotic HCC (12, 13). Men with a high baseline body-mass index have a five times higher liver cancer mortality than men with a normal body-mass index (4). Also hemochromatosis (associated to HFE1 gene mutations) is involved in the risk of developing NAFLD and HCC. Presumably, the iron overload leads to hepatic inflammation, fibrosis and carcinogenesis (8, 12). Furthermore, is HCC less common associated with autoimmune hepatitis, alpha-1 antitrypsin deficiency, cholestatic liver disorders and Wilson’s disease (8, 9). Autoimmune hepatitis is a chronic disorder with progressive liver injury (which can progress to cirrhosis) as the result of a cell- mediated immunologic attack directed against liver cells. Alpha-1 antitrypsin deficiency is another inherited disorder that causes abnormal folding of the alpha-1 antitrypsin protein. The abnormal folded protein is not secreted from the liver. How the retained protein leads to liver disease is not known. Wilson’s disease is also an inherited disorder with an accumulation of copper in the liver due to failure to excrete excess amounts of copper. Examples of cholestatic diseases are gallstone or malignant obstruction of the bile ducts, and primary biliary cholangitis (8). Tobacco is another cofactor contributing to the development of HCC. Infection with andeno-associated virus 2 is associated with HCC without underlying cirrhosis (8, 9). Other factors associated with an increased risk are older age, male sex, increased alfa-fetoprotein level, persistent increase in alanine aminotransferase level and progressive impairment of liver function (3). The incidence of HCC rises with age and reaches a maximum at 65-70 years old. HCC 4
is 2.5 times more frequent in male then female (8). Normally, alpha-fetoprotein (a glycoprotein) serum levels are very low (typically 10ng/ml), but can be elevated in patients with HCC, liver disease, germ-cell tumors, and liver regeneration (14). 1.1.3 Pathogenesis The complex multistep process for the development of HCC is the result of the accumulation of somatic genomic alterations in driver and passenger genes along with epigenetic modifications. This explains the extensive molecular heterogeneity of HCC. The process involves sustained inflammatory damage with necrosis and regeneration of the hepatocytes combined with fibrotic deposition (4). The development of HCC starts with low-grade dysplastic nodules which develop to high-grade dysplastic nodules which can eventually transform into early-stage HCC (8). The risk of HCC is elevated in cirrhotic patients and increases in parallel to progressive liver function deterioration (4). 1.1.4 Symptoms Unless the cancer is detected at an early stage, the symptoms of HCC are similar to the symptoms of cancer and liver failure (3). HCC can give following symptoms: jaundice, weight loss, abdominal pain, abdominal fullness, and nausea. Tense ascites and pain on palpation of the liver can suggest Budd-Chiari syndrome caused by HCC invasion of the hepatic veins (9). The symptoms of chronic liver disease are jaundice, hepatomegaly, abdominal vein dilatation, gynecomastia, peripheral edema, palmar erythema, and splenomegaly (mainly due to portal hypertension), and hematemesis (due to underlying portal hypertension causing esophageal variceal bleeding) (9). Symptoms indicate an already advanced stage of HCC with a median life expectancy 40 years if Asian, aged >20 years if African or family history of HCC). Surveillance is not recommended in the presence of advanced cirrhosis (Child-Pugh class C) because it prevents the application of potentially curative therapies. Patients on the waiting list for liver transplantation should be screened for HCC no matter what their liver functional status is. This is to detect tumors that exceed the conventional criteria for transplantation (8). The recommended method of surveillance is an ultrasonography every 6 months (with a sensitivity of 65-80% and a specificity of >90%). When a nodule of
with CT), and lack of data on accuracy. Where visualization with ultrasound is difficult (patients with obesity and fatty liver), CT and MRI may be used (8). An objective, non-invasive, and reproducible alternative for surveillance and early diagnosis of HCC are serum tumor markers. Unfortunately, the use of alfa-fetoprotein (AFP) levels can identify patients with HCC with only a sensitivity around 60% and a specificity around 80%. AFP levels of 400ng/ml or higher are remarkably suspicious, but not diagnostic for HCC (8). The combination of ultrasonography and APF increases the detection rates but also the cost and false-positive findings. The accuracy of other tumor markers (such as glypican 3, lectin-bound alfa- fetoprotein, Golgi protein, des-gamma carboxyprothrombin, and Dickkopf) is not known (4, 8). 1.1.6 Diagnosis As liver cirrhosis is the most common underlying cause of HCC, it has worldwide been accepted as the precondition of the non-invasive diagnostic criteria for HCC. Liver cirrhosis has a high specificity explaining its important role in the non-invasive diagnosis of HCC (15). Patients with HCC can be diagnosed based on findings from imaging (non-invasive) or biopsy (invasive) analyses. HCC can be detected with high levels of specificity by radiological analyses (i.e. MRI or CT) in patients with liver cirrhosis, which makes biopsy no longer necessary for many patients (3). If the lesion is 2 cm or more and shows vascular uptake in the arterial phase and washout in the portal, venous or delayed phases at CT (radiological hallmarks of HCC), the radiological diagnosis is achieved with a specificity of 95-100% and biopsy is not necessary. For lesions of 1-2 cm that show the radiological hallmarks, the diagnosis needs to be confirmed by two imaging techniques (CT and MRI). For nodules smaller than 1 cm only ultrasound follow-up at 3-4 months is recommended because they are unlikely to be HCC. Although the specificity of the used agents is suboptimal, contrast-enhanced MRI might help in the diagnosis of HCC (8). In patients without cirrhosis, or if radiology is not diagnostic for HCC (mainly with early-stage HCC lesions), biopsy and pathological diagnosis is required. Biopsy has a sensitivity of 70-90% for all tumor sizes, but diminishes to
To confirm the diagnosis of HCC immunohistochemical analyses of glypican 3, heat shock protein 70, glutamine synthetase, and clathrin heavy chain may be used as they have a 100% specificity, but they cannot replace the need for an expert pathologist to diagnose HCC because of their suboptimal sensitivity (3, 4). 1.1.7 Treatment 1.1.7.1 Staging The treatment options and prognosis of HCC are based on the stage of the disease at the time of diagnosis (5, 7). Because the TNM (tumor–lymph node–metastasis) system is not useful for HCC, another staging system is needed (3, 5-7, 12). The morbidity and mortality of patients with HCC is significantly influenced by the frequent underlying chronic liver disease, or liver failure. Therefore, staging approaches that include metabolic markers and functional parameters have been shown to be clinically more useful and practical (5). The most commonly used HCC staging system is the Barcelona Clinic Liver Cancer (BCLC) staging system. This staging system determines the cancer stage based on severity of liver disease, tumor burden, the patients performance status, and cancer related symptoms (3, 5-7, 12). HCC is divided in five cancer stages according to the BCLC staging system (see Figure 1.1): stage 0 (very early stage: Child-Pugh A, solitary lesion
tumor and the underlying cirrhosis simultaneously. There are restricted criteria for liver transplantation and the standard criteria are the Milan criteria (a single nodule ≤5 cm or up to three nodules ≤3 cm). They provide the best post-liver transplantation survival in hepatocellular carcinoma (5-year survival of >70% and a recurrence rate of
Figure 1.1: BCLC staging and treatment strategy. ECOG PS=Eastern Cooperative Oncology Group Performance Status (4). Unfortunately, tumor recurrence occurs in 70% of the cases at 5 years. Tumor recurrence includes as well de novo tumors within the oncogenic liver as true recurrence due to dissemination. For these patients, liver transplantation is the most effective treatment option to prevent intrahepatic recurrence (4). Another option for recurrent HCC is considered to be repeated hepatectomy. Since there are multiple limiting factors for repeating surgery’s utility in HCC (such as postoperative adhesion, insufficient liver remnant and change of intrahepatic structure), effective and less invasive treatment alternatives (such as locoregional therapies) are needed (16). There are different types of locoregional therapies for HCC: percutaneous ablation and transarterial therapy (5-7). Ablation causes tumor necrosis by injection of chemical agents (most commonly used is ethanol) or temperature modification (laser, radiofrequency, cryoablation, or microwave) (4). Previously, transarterial embolization therapies were only used for patients with unresectable HCC and stage B disease. Currently, they play an increasingly important role in earlier stage 9
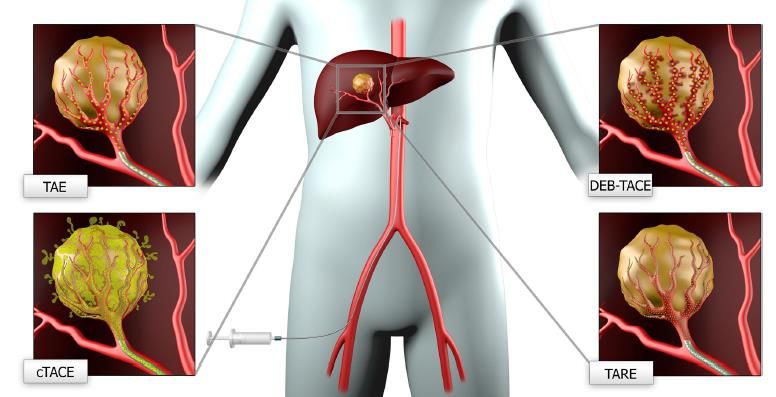
patients. In addition to surgery, they can control local disease and serve as a palliative treatment of patients with unresectable HCC (5-7). They may also be used for down-staging the tumor, defined as the reduction of the HCC burden with the aim of meeting the acceptable criteria for transplantation or resection (3). 1.1.7.2.1 TRANSARTERIAL EMBOLOTHERAPY The drug-delivery and treatment efficacy can be greatly improved by targeted drug delivery. Furthermore it can lower treatment costs and diminishes side effects (19). The normal hepatic parenchyma has a dual blood supply, with predominant supply from the portal vein and less from the hepatic artery. HCC tumors, however, have an almost complete supply from the hepatic artery. This suggests that transarterial therapies can target the tumors more specifically while sparing normal parenchyma. There are different types of transarterial embolotherapy: transarterial or bland embolization, chemoembolization, and radioembolization as shown in Figure 1.2 (5-7). Figure 1.2: The different types of transarterial embolotherapy. TAE: transarterial or bland embolization, cTACE: conventional transarterial chemoembolization, DEB-TACE: drug-eluting beads transarterial chemoembolization, TARE: transarterial radioembolization (5). There are several contraindications to embolotherapy, namely: acute illness, decompensated cirrhosis, poor functional status, major systemic comorbidities, and an unfavorable anatomy (7). Furthermore, an active systemic infection, leukopenia, an uncorrectable bleeding disorder, severe renal insufficiency, a previous shock related to contrast media, and hepatic encephalopathy are absolute contraindications to embolotherapy (5). The evaluation of patients for embolotherapy contains detailed physical, history and laboratory tests and imaging data to appraise hepatic function, vascular anatomy, generalized functional status and tumor burden (7). 10
To implement this targeted drug delivery methodology into clinical practice, the Computational Medical Magagement Program has been developed. It consists of three stages: the first stage is the patient evaluation, the second stage is the computer modeling, and the last stage is the clinical implementation. The patient evaluation stage consist of classification of the tumor, choosing the best treatment route, obtaining the patient’s geometry and flow conditions. In the computer modeling stage, computational case studies determine the best injection region and interval. The final stage consists of the optimal catheter positioning and injection. Afterwards, the efficacy of the treatment is evaluated (19). To evaluate the effect of the locoregional therapies on the tumor, the measurement of changes in tumor diameter is inaccurate. The locoregional techniques cause tumor necrosis but without direct effect on the size of the tumor. In addition, the assessment of tumor necrosis is needed and evaluated by the absence of contrast uptake during the arterial phase. The evaluation of the effect of the locoregional therapies is measured by the modified response evaluation criteria in solid tumors (mRECIST) and the European association for the study of the liver (EASL) criteria (4). 1.1.7.2.1.1 TRANSARTERIAL OR “BLAND” EMBOLIZATION In transarterial embolization (TAE), vaso-occlusive materials (such as gelatin sponge, ethiodized oil, cyanoacrylate glue, polyvinyl alcohol (PVA), and microspheres; with 50 μm PVA or 40–120 μm microspheres most currently used) without addition of any cytotoxic agents are delivered into the tumor supplying arteries by a selective catheter. This causes occlusion of the terminal arterioles and ischemic necrosis of the tumor (5, 7). The caused ischemia can trigger peritumoral angiogenesis which can lead to paradoxical tumor growth and metastatic spread (6, 18). Currently, TAE is not considered in the official treatment guidelines for HCC. Comparing symptomatic treatment with TAE in patients with unresectable HCC, showed that in HCC population with BCLC stage A–B, TAE is associated with a slower growth of the tumor. However TAE does not have an impact on the survival of patients with non-surgical HCC (5, 20). 1.1.7.2.1.2 CHEMOEMBOLIZATION In this paragraph, the methodology of transarterial chemoembolization (TACE), the absolute and relative contra-indications for TACE, the effect of TACE on HCC and the most frequent adverse event for TACE, namely post-embolization syndrome, are discussed. Transarterial chemoembolization (TACE) involves the transarterial delivery of both embolic and chemotherapeutic agents to the tumor, which causes cytotoxicity and ischemia. Rapid washout of the chemotherapeutic drug is prevented by the embolization of the vascular supply of the tumor 11
what also leads to ischemic tumor necrosis. This mechanism ensures a better locoregional diffusion into the targeted tumor tissues, while minimizing systemic toxicity (5, 6). TACE blocks the primary blood vessels of the tumor which causes a local anoxic environment. This can lead to recurrence and metastasis by the activation of vascular endothelial growth factor and vascularization (18). There are two types of TACE: conventional TACE (cTACE) and TACE by drug-eluting beads (DEB- TACE) (7). Conventional TACE (cTACE) consists of an intra-arterial infusion of a water-in-oil emulsion of a chemotherapeutic agent cocktail with Lipiodol (Lipiodol® Ultra-Fluid, Guerbet) followed by embolic particles. The chemotherapeutic agents include doxorubicin, idarubicin, cisplatin, epirubicin and mitomycin-C. For single drug cTACE, doxorubicin is the most commonly used (at a dose from 30 to 75 mg/m2, to a maximum of 150 mg), but also combination drug cTACE has been described (5, 7, 21, 22). Lipiodol serves as a micro-embolic agent and tumor-seeking drug carrier. It is taken up by and entrapped in the tumor cells for 8-12 months, while it only stays 4 weeks inside non-tumoral liver parenchyma. Lipiodol diminishes the drug washout from the tumor cells and causes ischemic necrosis (5). The release of the chemotherapeutic agent from the Lipiodol emulsion is with a half- life of approximately 1 hour (21). The most commonly used embolizing agents are gelatin sponge particles (gelfoam) with a diameter of 1mm and polyvinyl alcohol particles (PVA) with a diameter of 45 to 150 microns (10). The DEBs (drug-eluting beads) are non-resorbable embolic microspheres that can carry cytotoxic drugs (doxorubicin or epirubicin) and gradually release the drug over time at the targeted lesion to increase tumor exposure to chemotherapy and reduce systemic drug exposure. There are two types of DEB-TACE microspheres: the DC Beads (Biocompatibles UK Ltd.) are PVA-based microspheres and range from 75 to 900 µm in size, while the Hepa-Sphere microspheres (Merit Medical Systems, Inc.) are superabsorbent polymer based and range from 120 to 800 µm in size (5). The drug release kinetics from the microspheres varies based on the concentration of the drug, the osmolarity of the tumor bed and the size of the microspheres (6). The 100-300 µm microspheres have half-lives of drug-elution of 150h and the 700-900µm microspheres have half-lives of drug- elution of 1730h (21). There is no recommendation for which DEBs should be used as there are currently no RCT’s (randomized control trials) that compare the different DEB microspheres (22). There are some absolute and relative contra-indications for TACE including tumor diameter >10 cm and impairment of liver function. Therefore, not all patients with intermediate-stage HCC can be treated with TACE (3). Asymptomatic patients with a solitary or limited multifocal HCC without 12
extrahepatic spread or vascular invasion and well-preserved liver function are the best candidates for TACE (3). TACE shows improved survival over symptomatic treatment for HCC patients (P=0.01) (6, 23). For intermediate stage HCC, cTACE showed a median overall survival of 20 months while best supportive care showed a median overall survival of 16 months (22). There is still no general standardization for the TACE procedures. The optimal chemotherapeutic/embolic agents and the retreatment strategies including standardization of treatment schedule and indications still need to be determined (5). Prognostic factors for TACE patients were alpha-fetoprotein level, portal vein tumor thrombosis, and the number of TACE procedures (23). DEB-TACE and cTACE have similar clinical indications and contraindications. Although DEB- TACE is better tolerated and more reproducible, it has no meaningful clinical benefits or no increase in survival compared to cTACE (3, 5). Despite DEB-TACE was correlated with a better safety profile than cTACE, DEB-TACE didn’t show superiority in treatment efficacy, time to disease progression, or survival over cTACE (P>0.05) (24). DEB-TACE failed to show superiority over cTACE in terms of survival, safety, and tumor response in several meta-analysis and comparative studies (22). There was no statistical difference of severe adverse events between cTACE and DEB-TACE patients (P=0.36). cTACE did cause more often post-embolisation syndrome and thus a longer hospital stay (p=0.001), but global costs didn’t show significantly difference between cTACE and DEB-TACE (23). Although cTACE shows persuasive clinical results, the evidence for clinical efficacy has not yet been well assessed in randomized clinical trials. There is no standardization to make uniform comparison of the data among the current studies available. There is also an increased difficulty in comparison of different centers due to the fact that numerous staging systems, inclusion criteria and exclusion criteria are used. This all makes the interpretation of the results challenging (6). The most frequent adverse event for TACE is post-embolization syndrome (22, 25). It is characterized by fever, nausea, vomiting, and pain (22). Post embolization syndrome can vary in severity, ranging from only pain, fever and short-term elevation in serum bilirubin, to irreversible liver failure (26). 1.1.7.2.1.3 RADIOEMBOLIZATION In this paragraph, the following points are discussed: the methodology of transarterial radioembolization (TARE), the pretreatment examinations before undergoing TARE, the contra- 13
indications for TARE, the effect of TARE on HCC, the most frequent adverse events for TARE and the validated predictors of recurrence of the tumor after radioembolization. Transarterial radioembolization (TARE) delivers radionuclide loaded microspheres to arteries that supply the tumor to reach tumoricidal radiation doses while sparing the normal liver parenchyma. The most commonly used radionuclide is Yttrium-90. It is a pure bèta-emitter with a short half-life (2.67 days or 64.2 h) and a limited capacity to penetrate tissues (from 2.5 to 11 mm), a radiation dose of up to 170 Gy can be administered (3, 5, 7, 9). Another recently introduced radionuclide is Holmium-166. Holmium-166 emits low-energy gamma rays and bèta radiation. The emitted low gamma rays makes these microspheres visible by single-photon emission computed tomography/computed tomography (SPECT/CT). Besides, the holmium-166 microspheres are also visible with MRI. Holmium-166 can penetrate soft tissue with a mean beta particle range of 2,5 mm and a maximum of about 9 mm. Holmium-166 has a half-life of 26,8 hours (27, 28). In the Holmium Embolization Particles for Arterial Radiotherapy (HEPAR) trial, it was determined that the maximum tolerated radiation dose is 60 Gy. To attain an equal radiation-absorbed dose, there is more activity needed when using holmium-166 microspheres than when using yttrium-90 microspheres, because of the shorter half-life and differences in energy spectra. After delivery of the holmium-166 microspheres, about 90% of the radiation is released within the first four days. When using yttrium- 90 microspheres, 90% of the radiation is released within the first eleven days (27). There are two types of Yttrium-90 loaded microspheres (see Table 1.1): glass microspheres (TheraSphere; BTG Corporation) and resin microspheres (SIR-Spheres; Sirtex Medical) (3, 5, 9). Resin microspheres have a diameter of 20-60 µm, a density of 1,6 g/cm3, and consist of biocompatible resin-based microspheres. Glass microspheres have a diameter of 20-30 µm, a density of 3,3 g/cm3, and have a higher activity per sphere (2500Bq per sphere) than resin microspheres (50Bq per sphere) (9, 27). This indicates that a smaller number of glass microspheres are needed to reach a tumoricidal dose, thus have less embolic effects than the SIR-Spheres (5, 9). An advantage of the SIR-Spheres could be a better distribution of the radioactivity over a larger surface, because the same dose is released by a greater number of particles. However, both types of microspheres have resulted in similar outcomes and efficacies (5). The recently developed third type of microsphere for radioembolization are Holmium microspheres. These microspheres contain holmium-166, incorporated in a matrix of poly-L-lactic acid (PLLA), instead of yttrium-90 and are commercially available in Europe as QuiremSpheres (Quirem Medical BV, Deventer, the Netherlands). These microspheres have a diameter of 15-60 µm and a density of 1,4g/cm3. Given 14
that the density of holmium-166 microspheres is the closest to the density of blood, could benefit the intravascular flow dynamics and distribution of these microspheres (27-29). Table 1.1: Microsphere characteristics (27). Table 1.2: Treatment and pretreatment microsphere characteristics (30). Before patients undergo TARE, they have to undergo a history and physical examination (including Eastern Cooperative Oncology Group performance status (ECOG)), arteriography/macroaggregated albumin (MAA) lung shunting study, clinical laboratory tests (including a hepatic panel and serum alfa-fetoprotein) and imaging (including chest computed tomography (CT), abdominal CT or magnetic resonance (MR) scan and bone scan) (9). To assist the dosimetry planning, pre-delivery angiographic mapping procedures are performed. They determine the hepatopulmonary shunt fraction and the enteric collaterals within the anticipated arterial treatment zone (7). Therefore pretreatment aortic, celiac trunk, and superior mesenteric angiography to assess the hepatic vasculature, portal vein patency, the presence of arterioportal shunting, and surrounding structures is performed. Incomplete treatment and/or treatment failure can be caused by not recognizing a vessel supplying the tumor. In addition, adverse events may occur when microspheres are injected through non-target vessels. To avoid non-target radiation, splanchnic and pulmonary shunting is assessed. Arteriovenous shunts occur 15
relatively much in HCC. When a sufficient doses of microspheres is administered in arteriovenous shunts that bypass the tumor capillary bed and enter the lungs, a radiation pneumonitis can be caused (9). Besides the assessment of the hepatopulmonary shunting and gastrointestinal deposition, this pretreatment is also used to determine the location of the microcatheter in the artery and the injection force. Still, the particle distribution in the liver can vary between this pretreatment and the actual treatment which can result in radiation-induced complications because some parameters who can vary, may influence the distribution of the particles in the liver (31). As pretreatment a scout dose of about 150.000 99mTc-macroaggragated albumin (99mTc-MAA) particles (see Table 1.2) is administrated in cause of radioembolization with Yttrium-90 microspheres. When treatment with Holmium-166 microspheres a scout dose of about 3 million holmium-166 particles is administrated. The shape and size of these holmium-166 scout dose microspheres are equal to the holmium-166 microspheres used for therapy but with limited embolization effect and limited radioactivity (around 250 MBq). The activity of the scout dose of Holmium-166 microspheres is safe but still sufficient to be visualized using SPECT/CT. This causes that these microspheres can predict the intrahepatic biodistribution and the lung shunting better than the 99mTc-MAA. Also extrahepatic depositions can be detected by the holmium-166 scout dose. The holmium-166 scout dose can reliably determine the dose to the tumor and healthy liver prior to treatment. This technique could lead to more personalized medicine. Until now, the holium- 166 scout dose is not yet commercially available and has only been used in clinical studies. Because holmium-166 emits a primary gamma photon, radioactive contaminations by holmium- 166 microspheres could be more easily discovered than radioactive contamination by yttrium-90 microspheres (27, 28). For undergoing TARE, patients should have an ECOG score less than or equal to 2, be able to ambulate for more than half of the day and a bilirubin less than or equal to 2 mg/dl. Patients with multinodular/bilobar disease, excessive tumor burden and limited hepatic function are generally excluded (9). Patients with excessive hepatopulmonary shunting and technically inevitable gastrointestinal deposition based on 99m TcMMA-scan are also excluded (5). Patients with extensive portal invasion are usually excluded. But an individual decision should be made because some patients with good liver function and branch portal invasion may be considered for radioembolisation. Patients with good liver function (Child-Pugh A and normal bilirubin) and low tumor burden are the best candidates for radioembolization, especially if only 1 lobe is affected (11). Contraindications for radioembolization with holmium-166 microspheres and yttrium-90 microspheres are similar (27). 16
The treatment with radioembolization could be optimized with the possibility of intra-procedural imaging of the infusion of the microspheres. The outcome of the treatment could be predicted by the post-procedural assessment which allows the visualization of the distribution of the microspheres. The current commercially viable and clinically used Yttrium-90 microspheres have the big disadvantage that they cannot be detected in vivo with medical imaging techniques. This hinders intra- and post-procedural feedback. As mentioned before, the new Holmium-166 microspheres can be visualized with CT and MRI, what makes real-time monitoring of the infusion of the microspheres and post-procedural imaging possible (28). Radioembolization with Yttrium-90 is shown to be effective in the treatment of unresectable primary HCC and colorectal hepatic metastasis. TARE showed tumor response rates from 40% to 90% in cohort studies. It showed antitumor activity but no proven survival benefit (4). Its tumoricidal effect may provide symptomatic improvement because of a decreased tumor burden. It is usually well tolerated but there are reported several side effect due to irradiation of other organs such as severe gastrointestinal toxicities (nausea, vomiting, abdominal pain, gastrointestinal ulcers, gastritis, and transaminitis) and fatigue (3, 6, 9). These side effects are probably due to the deposition of radioembolic material in undesired locations which is possible through variant or collateral circulation (6). Another side effect which develops 4 to 8 weeks after treatment is known as radioembolization-induced liver disease, a form of sinusoidal obstruction syndrome. These patients present with mild ascites, jaundice and moderate cholestasis (3). Signs and symptoms of hepatic abscess, radiation cholecystitis, perihepatic ascites, pleural effusion, and radiation pneumonitis are also possible (9). The adverse events of radioembolization with yttrium-90 and holmium-166 were comparable, mainly fatigue and abdominal pain. Two prospective phase I and phase II clinical studies showed that a mean whole-liver dose of 60Gy of holmium-166 radioembolization induces tumor response and is safe. These studies were performed in a population of liver metastases and there are ongoing trials investigating the effect of holmium-166 radioembolization in patients with hepatocellular carcinoma, neuroendocrine tumor metastases, and colorectal cancer metastases (27). Until today, the safety and toxicity of this new therapy is not yet proven for hepatocellular carcinoma (HCC), particularly in patients with liver cirrhosis (29). Validated predictors of recurrence of the tumor after radioembolization are tumor size, macroscopic and microscopic vascular invasion, multifocality and poor differentiation. In contrast to early recurrence (
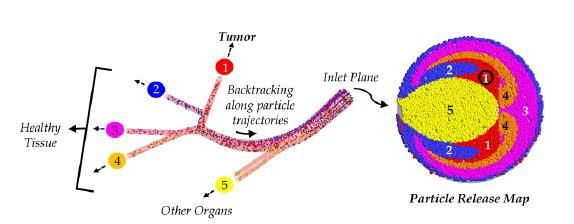
1.2 Search for optimizing the transarterial embolotherapy The optimal transarterial procedure should deliver the injected particles into the target tumor and there should be no delivery in the healthy liver tissue or elsewhere in the body to avoid systemic toxicity (21). Although transarterial therapies show improvement of the prognosis of intermediate HCC, there are quite some differences in the post-treatment outcomes. This can probably be explained considering the fact that these transarterial treatments are not well standardized and vary in chemotherapeutic agents with different doses and embolizing agents, therapeutic schedules and treatment devices depending on the operator’s choice (10, 21). The fact that some particles do not reach the targeted tissue and end up in healthy tissue can lead to patients who do not respond to the treatment, non-responders, instead of patients who do respond to the treatment, responders (19, 32). One of the challenges is to improve the efficiency of the transarterial therapies by targeting only the target tumor. After injection, not all particles end up in the targeted region. A considerable percentage of the injected particles deviate to the non-targeted regions and expose these areas to toxic drugs/radiation and/or embolization, which may lead to severe side-effects. This also means that there is an increased amount of the intended drug/radiation and/or embolization reaching the tumor which reduces the efficacy of the treatment (10, 32). It is shown that a personalized intervention can cause a high concentration dose in the tumor, while sparing the surrounding parenchyma (25). Although TARE is a safe treatment option for HCC, non-target radiation may cause complications. The non-target radiation can be caused by differences in the injected microspheres used in pretreatment and treatment. It can also be caused by alterations in the hemodynamics at the part of the artery lumen near the tip of the catheter, the blood flow in this part of the lumen is straightly affected by the injection of the microspheres (near-tip hemodynamics). In this regard, the physical characteristics and quantity of the injected microspheres can be valuable. The injection velocity and the placement of the microcatheter in the artery (radial and axial location) can play an important role in the alterations in the near-tip hemodynamics. There have been several studies who have analyzed these parameters (31). Other variables that are associated with the particle distribution are the vessel geometry and injection timing (19, 33). Kennedy et al. tested the impact of two types of microsphere release distributions in the inlet plane of the main hepatic artery, namely uniform (evenly spaced particles) and parabolic (more particles around the center of the vessel). By backtracking the trajectory of the injected microspheres, the 18
relation between the particles distribution and their radial position on the injection plane was shown in a particle release map (PRM). The particle release maps (PRMs) (see Figure 1.3) can visually link the injection position with the corresponding exit branch. By generating multiple PRMs from injections with alternating injection parameters, these PRMs can help to determine the appropriate injection parameters to target the correct area. This study showed that the type of micron particle release distribution and the release position have an important impact on particle distribution between the outlets (33). Also the best injection interval can be determined by generating multiple PRMs at subsequent intervals throughout the cardiac cycle (19). Figure 1.3: Particle release map. Particle injection in the red Figure 1.4: A graph in which the ratio of area leads to particle disposition in the tumor region. Particle catheter injection velocity to vessel velocity injection in the blue, purple or orange area leads to particle ratio is plotted versus the time for four disposition in the healthy tissue. Particle injection in the microsphere-suspension input functions (1). yellow area leads to particle disposition in other organs (2). Presently, a standard catheter with a manually operated syringe is used for delivering the radioactive microspheres into the liver. This results in a limited control of the catheter-tip placement. Kleinstreuer et al developed a new type of catheter, Smart Microcatheter (SMC) and evaluated its effect on the local bloodflow and particle distribution in the hepatic artery system. It is an anchored, radially adjustable catheter with struts that can provide a stable and precise positioning of the catheter-tip in vessel plane, allowing a better targeting (34). The same study group further investigated this methodology in a more complex geometry by using a patient-inspired model. The complexity of the used geometry seemed to have a considerable impact on the PRM. Using the more complex patient-specific geometry, the release regions shifted more drastically throughout the cardiac pulse compared to the basic geometry in their previous study and were not as well defined. The SMC was connected to an automated microsphere supply apparatus (MSA). This ensures that particles can be injected with different distributions (see Figure 1.4) such as ramp, S- curve, and step. The less abrupt injection functions (ramp and S-curve) seemed to be better options for tumor-targeting because they provide a more compact particle stream (1). 19
Another study of Childress et al analyzed the influence of the moment of injection within a cardiac pulse on the particle release maps (PRMs). This study showed that compared to systolic injections, the injections at diastolic phase generated a more relatively constant PRM, due to its semisteady flow conditions (2). Aramburu et al performed a study to analyze the impact of following parameters: catheter-tip position, tumor burden and the particle characteristics on the particles transport. The study showed that the catheter-tip location within the hepatic artery plays a very significant role in the particles distribution and is much more important than the microagent characteristics. According to their study, the tumor burden is another important parameter in the particle distribution. The tumor- bearing segments of the liver have an increased blood flow rate which increases the power to drag particles to these segments (30). In the master thesis of Bomberna, the impact of the sizes and the distribution of tumor nodules throughout the liver was investigated. A case with outflow boundary conditions defined using Murray’s law was compared with the particle distribution for eleven different cancer scenarios. His research showed that the particle distribution in the arterial network is greatly influenced by the cancer burden, what signifies that the choice of boundary conditions is crucial (35). This is in agreement with the work of Aramburu et al. However, Koudehi and Sánchez noted that the particle characteristics do play a critical role in particle distribution (10, 32). These findings are in contrast with the findings of Aramburu et al. Another study of Aramburu et al analyzed the impact of the orientation of the angled tip of the catheter and the injection velocity on the distribution of the injected resin microspheres in the liver on a segment-to-segment basis. The results of this study suggests that injection velocity and microcatheter tip orientation have a minor role in the particle distribution since the particle distribution tries to match the blood flow split (31). In Koudehi’s and Sánchez’s research, the injection velocity had also a minor role in the particle distribution (10, 32). Both Koudehi and Sánchez found that the injecting place of the particles, near a bifurcation or further away from it, had a remarkable impact on the PRMs. In Sánchez’s research the PRMs were more dissimilar to each other than the PRMs in Koudehi’s research (10, 32). However, these results are hard to generalize since they are highly patient-specific. Because each patient has a specific liver cancer state and hepatic artery structure, which plays a valuable role in the outcome of TARE, the conclusions of these studies cannot be generalized (31). Studies with a larger number of patient-specific cases are needed. Furthermore, good validations 20
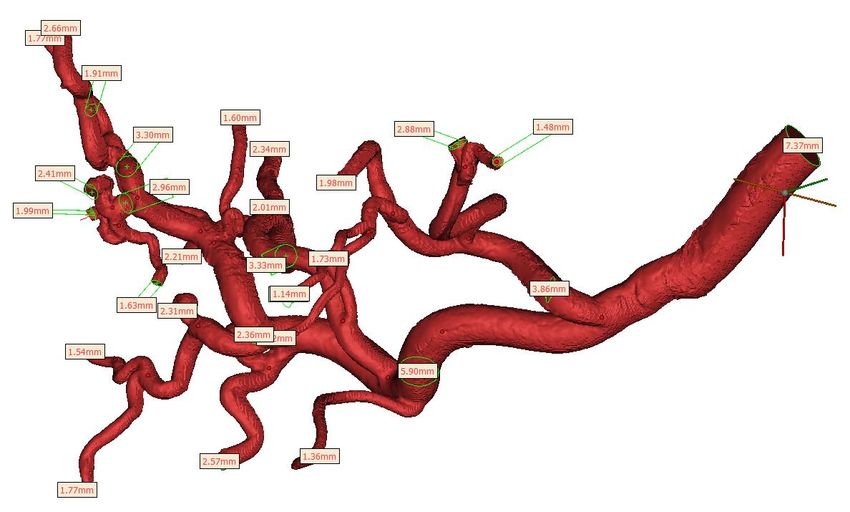
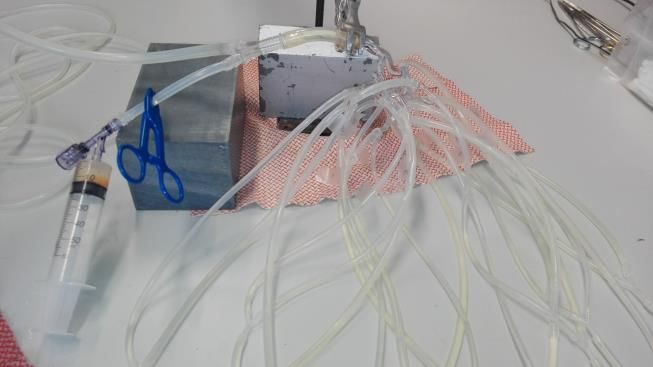
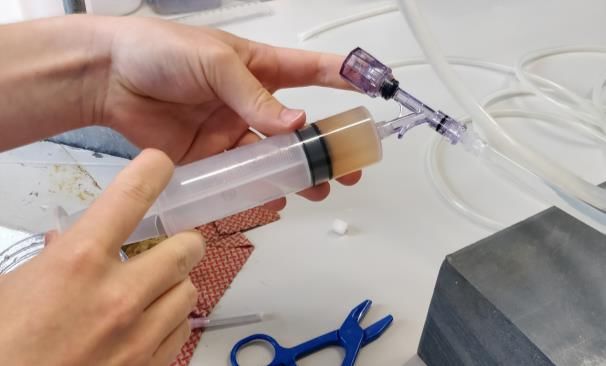
of the computational fluent dynamics are still needed to see if their predictions of the particle distributions correspond to reality. 1.3 Goal of this master thesis The aim of this master thesis is to evaluate the effect of different parameters on the particle trajectory and distribution in the liver. This is studied by modelling a patient-specific embolization treatment by creating three-dimensional reconstructions and a 3D print of the arterial vascularity of the patient’s liver. The effect of different parameters on the outcome of the embolization is studied by means of an in vitro experiment to simulate the targeted injections. The master thesis of Ghazal Adeli Koudehi (10) on this topic also included computer simulations followed by a validation study. In the validation study, the computational PRM was validated by an experimental in vitro set-up with a 3D printed model of the arterial vasculature of the liver. The bachelor thesis of Elena Jiménez Sánchez (32) included computer simulations in a liver from a radioembolization responder patient but no validation study. In this thesis, the computer simulations are not performed or discussed. But the experimental research in this master thesis focuses on refinement and further optimization of the experimental setup. Furthermore, the presented work can serve as a partial validation study for the computer simulations of Bomberna. For the computer simulations on this arterial model, see the master thesis of Tim Bomberna (35). 2 Methods To obtain detailed imaging data of the hepatic vasculature of a cirrhotic liver, vascular corrosion casting and micro-CT imaging was performed by Peeters et al. Thereafter, the segmentation of the arteries was done using Mimics (Materialise, Leuven, Belgium). Afterwards, the segmentation was reconstructed into a 3D geometry. To create a hollow 3D geometry the model was further edited in Magics (Materialise, Leuven, Belgium). Subsequently, the model was uploaded on the website of Materialise® (Leuven, Belgium) for 3D printing the model. Once the model was printed, it was implemented in the experimental setup. Afterwards, the experiments were performed to simulate the flow and particle distribution and to demonstrate the influence of boundary conditions on the flow and particle distribution. 2.1 Data of the cirrhotic liver Detailed imaging data of the hepatic vasculature of a cirrhotic liver was obtained by Peeters et al. in two succinct steps: vascular corrosion casting and micro-CT imaging (36). Thereafter, the segmentation of the arteries and generation of a 3D print of the arterial vascularity was done. 21
You can also read