Mandatory surveillance of methicillin-resistant Staphylococcus aureus (MRSA) bacteraemia in England: the first 10 years
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Journal of Antimicrobial Chemotherapy Advance Access published January 4, 2012
J Antimicrob Chemother
doi:10.1093/jac/dkr561
Mandatory surveillance of methicillin-resistant Staphylococcus aureus
(MRSA) bacteraemia in England: the first 10 years
Alan P. Johnson*, John Davies, Rebecca Guy, Julia Abernethy, Elizabeth Sheridan, Andrew Pearson†
and Georgia Duckworth‡
Department of Healthcare-Associated Infection and Antimicrobial Resistance, HPA Centre for Infections, Colindale, London NW9 5EQ, UK
*Corresponding author. Tel: +44-208-327-6043; Fax: +44-208-205-9185; E-mail: alan.johnson@hpa.org.uk
†Present address: Department of Advanced Computational Biology, University of Maryland, Washington, DC, USA.
‡Present address: Niterói, Rio de Janeiro, Brazil.
Since 2001 it has been mandatory for acute hospital Trusts (groups of hospitals under the same management)
Downloaded from http://jac.oxfordjournals.org/ by guest on July 19, 2015
in England to report all cases of bacteraemia due to Staphylococcus aureus together with information on their
susceptibility or resistance to methicillin. This allowed the incidence of methicillin-resistant S. aureus (MRSA)
bacteraemia (expressed as the number of cases per 1000 occupied bed days) to be determined for each
Trust. In late 2005, the scheme was enhanced to collect demographic, clinical and epidemiological information
on each case using a web-based data collection system. Analysis of this mandatory dataset has provided
important information on the trends in MRSA bacteraemia in England and has documented a year-on-year
decrease in incidence since 2006, following a government initiative in which Trusts were tasked with halving
their MRSA bacteraemia rates over a 3 year period. In addition, the enhanced mandatory surveillance
scheme has captured a wealth of data that have helped to further define the epidemiology of MRSA bacter-
aemia. It is to be hoped that based on the English experience of mandatory surveillance, other countries
will consider the implementation of similar schemes, not only for MRSA but for other pathogens of public
health importance.
Keywords: nosocomial infections, S. aureus, antibiotic resistance
Introduction system, lessons from it are likely to be applicable to other
countries.
A long-running surveillance scheme in which hospital microbiol-
ogy laboratories voluntarily report cases of bacteraemia to a The introduction of mandatory surveillance
national database (LabBase2) showed a dramatic rise in the of MRSA bacteraemia
occurrence of invasive methicillin-resistant Staphylococcus
aureus (MRSA) infections in England, Wales and Northern The collection, analysis and feedback of data from the manda-
Ireland throughout the 1990s.1 This seemingly inexorable rise tory surveillance scheme were tasked to the then Public Health
in MRSA bacteraemia generated considerable public and media Laboratory Service, which became the HPA in 2003. Guidance
interest, with the result that MRSA became the subject of political on the mandatory surveillance scheme was published in a
debate, with opposition politicians using data on healthcare- letter from the Chief Medical Officer (CMO), which outlined the
associated infections to criticize the government of the day minimum dataset to be collected by Trusts.3 This comprised:
regarding their management of the health service.2 By way of re- (i) the total number of blood cultures (sets taken, not individual
sponse and in an effort to drive down rates of MRSA bacter- bottles); (ii) the total number of positive blood cultures; (iii) the
aemia, the Department of Health in England decided to total number of blood cultures positive for S. aureus; and
improve the robustness of surveillance by making the reporting (iv) MRSA-positive blood cultures expressed as a proportion of
of MRSA bacteraemia mandatory for all English acute hospital all S. aureus-positive blood cultures. These data were to be col-
Trusts (groups of hospitals under the same management) from lected quarterly by each Trust in England and submitted to the
April 2001, with the resulting data for individual Trusts being HPA via their regional offices. The CMO’s letter further explained
put in the public domain. This article discusses the initiation, that the government’s objective at that stage was the imple-
implementation, evolution and outputs of this innovative surveil- mentation of a national surveillance scheme that would allow
lance scheme over a 10 year period. Although this is a review of a comparison of MRSA bacteraemia rates between similar types
scheme in a European country with a socialized healthcare of hospital, with data for 6 or 12 month periods being published
# The Author 2012. Published by Oxford University Press on behalf of the British Society for Antimicrobial Chemotherapy. All rights reserved.
For Permissions, please e-mail: journals.permissions@oup.com
1 of 8Review
from April 2002.4 – 8 In order to allow comparison of MRSA rates remain in hospital overnight. As an example, renal patients are
between similar types of hospital, Trusts were initially classified prone to develop bacteraemia with S. aureus (including MRSA),
into three categories, namely: ‘single specialty’ (e.g. those only but mostly do not remain in hospital overnight. Thus, renal
undertaking orthopaedics, cancer or children’s health services), patients who develop MRSA bacteraemia would be included in
‘specialist’ (those with specialist services that receive patients the numerator data collected as part of the mandatory surveil-
referred from other Trusts for these services) and ‘general lance scheme, but would be excluded from the denominator
acute’ (which provide general acute healthcare services).4 Subse- used for calculating the rate of MRSA bacteraemia. Thus,
quently, this classification scheme was refined to comprise six further work is required to generate a fuller understanding of
categories, namely: small acute Trusts, medium acute Trusts, the relative risk of developing MRSA bacteraemia in this particular
large acute Trusts, acute teaching Trusts, acute specialist Trusts setting.
and acute specialist Children’s Trusts (Figure S1, available as
Supplementary data at JAC Online).
Enhancement of mandatory surveillance
The reporting of aggregate numbers of positive MRSA blood cul-
The issue of denominator data tures provided robust figures on the total number of MRSA bac-
teraemias in England and the incidence of MRSA bacteraemia
The incidence of MRSA bacteraemia in individual Trusts was
in individual Trusts. However, the purpose of surveillance is not
determined using figures derived from the KH03 national
Downloaded from http://jac.oxfordjournals.org/ by guest on July 19, 2015
simply to measure rates of infection per se, but to gather rele-
dataset as the denominator. The KH03 data, which are collated
vant clinical and epidemiological information so that potential
by the Department of Health, provide a count of the average
interventions aimed at reducing rates of infection can be intro-
number of beds occupied overnight in a Trust each day (bed
duced and their impact assessed. With this in mind, the manda-
days) and can be used as a measure of hospital activity in
tory MRSA surveillance scheme was enhanced in 2005 to capture
each Trust.9 For the purposes of comparison, the MRSA rate for
comprehensive data on individual cases of MRSA bacteraemia,
each Trust was presented as the number of MRSA bacteraemia
including patient demographics, date of admission, date of bac-
cases per 1000 occupied bed days. An initial report published
teraemia, location at time of blood culture, consultant specialty
after the first 6 months of mandatory surveillance (April –
and type of clinical care at the time the blood sample was taken.
September 2001) indicated that single-specialty Trusts generally
The implementation of this MRSA Enhanced Surveillance
had lower mean rates of MRSA bacteraemia (0 –0.23 per
Scheme required all Trusts in England to submit data via a
1000 bed days) than general acute Trusts (0.01 –0.41 per
web-enabled data capture system with mandatory data fields
1000 bed days), which in turn generally had lower rates than
from October 2005. This was in contrast to the earlier phase of
specialist Trusts (0.5 –0.69 per 1000 bed days).4 The report com-
surveillance when Trusts submitted data in a range of formats
mented that this ranking of Trust types was not unexpected,
through a range of reporting routes. In 2006, this system was
since patients with complicated clinical courses are frequently
further enhanced to support the collection of data on the prob-
referred to specialist Trusts, which, as a result, often have high
able source of the MRSA bacteraemia, although these data were
numbers of vulnerable patients prone to infection. In addition,
submitted by Trusts on a voluntary basis. Although the reporting
specialist Trusts frequently receive patient referrals from other
of enhanced data for MRSA bacteraemia was made mandatory
Trusts, which may include patients colonized with MRSA acquired
for English Trusts in 2005, the submission of enhanced data
in the first hospital. Colonization with MRSA was not recorded as
for cases of bacteraemia caused by methicillin-susceptible
part of the national mandatory surveillance, which only mea-
S. aureus (MSSA) was optional until January 2011, when it also
sured MRSA bacteraemia. However, colonization with MRSA is a
became mandatory.11,12
risk factor for the development of infection with MRSA10 and
any bloodstream infection developing in a colonized referred
patient after admittance to the specialist Trust would count
Feedback of data to stakeholders
towards its MRSA rate. A similar ranking of Trust types was
noted after the mandatory surveillance scheme had been An essential component of surveillance is the analysis and feed-
running for 3 years (April 2001–March 2004), the mean MRSA back of collated data to relevant stakeholders. Hence, the HPA
rates for single-specialty, general acute and specialist Trusts in was tasked from the outset with providing data on MRSA bacter-
the third year of surveillance being 0.09 (range 0 –0.28), 0.16 aemia rates for each acute Trust, the data (expressed as total
(range 0.04–0.33) and 0.24 (0.07 –0.45) cases per 1000 bed cases per 1000 occupied bed days) initially being published at
days, respectively.7 6 or 12 monthly intervals.4 – 8 Following enhancement of the
While bed occupancy figures were regarded as a useful de- mandatory surveillance programme, the additional data col-
nominator for undertaking broad comparisons of the MRSA lected allowed Trusts to determine the number of cases where
rates in different Trusts, there was increasing awareness that MRSA bacteraemia was likely to have been acquired while
they were not ideal in two regards. Firstly, the KH03 data for patients were in their care (referred to as ‘Trust-apportioned’
the current year are usually not available at the time the MRSA cases). Trust-apportioned cases were defined as inpatients, day-
figures are being analysed, so bed occupancy figures from patients or emergency assessment patients in their Trust who
earlier time periods have to be used initially, with the data had a positive blood culture taken ≥2 days after the date of
being reanalysed when newer figures become available. Second- admission.13 MRSA bacteraemia data analysed on the basis of
ly, bed occupancy data, which are based on overnight bed occu- these criteria were published from May 2010 onwards. In add-
pancy, are not applicable to specialties where patients do not ition, surveillance outputs were extended to include data on
2 of 8Review JAC
MRSA bacteraemia rates for each Primary Care Organisation the numbers reported by Trusts through the mandatory surveil-
(PCO), which are the bodies responsible for commissioning lance system with other available data sources, such as the
primary and secondary care from providers, such as hospital numbers of blood culture isolates of MRSA reported by hospital
Trusts. From 2009, the reporting frequency was amended, with microbiology laboratories through the voluntary scheme. Any
data thereafter being published on a monthly, quarterly and inconsistencies detected through such checking were fed back
annual basis;14 the data being produced according to the code to Trusts for investigation and comment.
of practice for the production of official statistics.15 The same cri- An additional measure to ensure accurate reporting by Trusts
teria were subsequently applied to the routine publication of was the announcement by the CMO in March 2006, that the
mandatory surveillance data on MSSA bacteraemia.14 From Chief Executive of each Trust would assume personal responsibil-
June 2010, however, data have also been made available on a ity for the accuracy of their data,22 it being implicit in this state-
weekly basis (as a rolling 12 week period of MRSA bacteraemia ment that Chief Executives supplying erroneous data would be
counts) via the HPA web site16 and the government web site liable to severe penalties. Critically, for Trusts failing to meet
data.gov.uk.17 However, the weekly data are not official statistics their target, the onus was on the Chief Executive to explain
but are provisional, as they simply reflect the best data available why and to develop a plan to remedy this in agreement with
at the time of publication and can change as outstanding labora- the Department of Health. In addition, the CMO’s letter stipu-
tory test results for susceptibility to methicillin become available. lated a shorter timescale for the reporting of data to the HPA,
The HPA also produces quarterly Commentaries, which aim to as the HPA was to subsequently supply the data to the Health-
disseminate collated information on the epidemiology of MRSA care Commission (now the Care Quality Commission) for inclu-
Downloaded from http://jac.oxfordjournals.org/ by guest on July 19, 2015
bacteraemia derived from analysis of the enhanced mandatory sion in their annual ‘health checks’, which assessed whether
dataset.13,18 – 20 standards of patient care and safety were being met. The intro-
duction of these measures marked a shift in approach, as previ-
ously the burden of responsibility would have fallen on the Trust’s
Setting of a national target to reduce MRSA infection control team, which may not have had access to the
resources needed to remedy the problem. In this way, Trust
bacteraemia
management teams became responsible for addressing the
Having established a surveillance system for monitoring rates of issue and allocating the necessary resources.
MRSA bacteraemia in hospital Trusts, the Health Secretary, Despite some doubts that the required reduction in MRSA
speaking at the Chief Nursing Officer’s conference in November rates could be achieved in the designated timescale,23 national
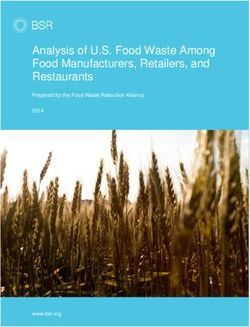
2004, announced that the government was setting Trusts a data from the mandatory surveillance scheme showed a 56%
target of reducing MRSA bloodstream infections by 50% by reduction in the number of reports of MRSA bacteraemia
2008.21 This target was made a priority by the Department of between 2004 and 2008 (Figure 1).24 The interventions used by
Health and additional resource was made available to reinforce Trusts in their efforts to reduce MRSA bacteraemia have not
the work of hospital infection control teams. Strategic Health been formally documented at a national level, but would likely
Authorities [organizations with management responsibility for have included improved hand hygiene (actively promoted by
the National Health Service (NHS) at a local level, such as all the National Patient Safety Agency’s ‘CleanYourHands’ cam-
acute Trusts and PCOs within a defined geographical area] paign),25 contact precautions, active surveillance cultures,
were required to produce Trusts-level trajectories for reducing improved management of intravascular lines, changes in anti-
bacteraemia numbers over this period for all Trusts within their biotic prescribing and deep cleaning of clinical areas.26 Many
boundaries. Any Trusts deviating from their target trajectory hospitals are also likely to have introduced the ‘care bundle’
were subject to inspection by teams of relevant experts
brought together by the Department of Health Improvement
Team. In addition, Trusts were required to show a reduction 9000
from the first year, so that the onus for the reduction should
not fall to an incoming Chief Executive should a Trust change 8000
its senior management near the end of the period.
MRSA bacteraemias (no.)
7000
Given the pressure placed on Trusts by the setting of a govern-
ment target for a 50% reduction in their rates of MRSA bacter- 6000
aemia, there was concern that some Trusts might be tempted 5000
to manipulate their data to facilitate a favourable outcome.
4000
Hence, a number of measures were put in place to minimize
the risk of this happening. To prevent Trusts spuriously claiming 3000
that isolates of MRSA from blood culture were contaminants or
2000
not clinically significant and thus not reportable, the Department
of Health stipulated that all positive blood cultures yielding 1000
growth of MRSA must be reported. A downside of this is that 0
the rationale for introducing mandatory surveillance (i.e. to gen- 2002 2003 2004 2005 2006 2007 2008 2009 2010
erate robust data on the incidence of MRSA bacteraemia) was
Year
potentially compromised by introducing a source of bias that
might overestimate the scale of the problem. An additional Figure 1. Numbers of MRSA bacteraemias in England reported through
check undertaken by the HPA involved routine comparison of the mandatory surveillance system, 2002–10.30
3 of 8Review
2500
Bacteraemia reports (no.)
2000
Female
1500 Male
1000
500
0
0–9 10–19 20–29 30–39 40–49 50–59 60–69 70–79 80+
Age group (years)
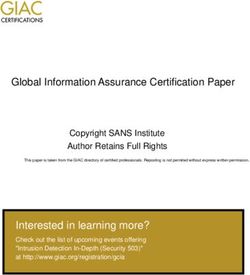
Figure 2. Age and sex distribution of cases of MRSA bacteraemia, April 2006– March 2008.31
Downloaded from http://jac.oxfordjournals.org/ by guest on July 19, 2015
approach, particularly for indwelling lines, following the Depart- Uncategorized
ment of Health’s ‘Saving Lives’ initiative.27 One author has specif- (7%)
ically suggested that the decolonization of MRSA carriers,
particularly in intensive care units, may have played a central
role.28 However, it may prove difficult to unequivocally define
which interventions were critical in reducing MRSA bloodstream
infections, as most hospitals probably introduced multiple inter- Within 2 days
ventions simultaneously. A confounding factor is that strain (29%)
typing data have indicated that the prevalence of EMRSA-16,
one of the two dominant strains of MRSA in England, was
already in decline at the time Trusts were implementing mea-
sures to reduce their rates of MRSA bacteraemia, making it diffi-
cult to determine what contribution active interventions made to
the overall decrease in MRSA bacteraemia.29 Despite these un-
certainties as to the reasons for the decline in MRSA bacteraemia >2 days
(64%)
in English Trusts, the decline has continued since 2008 (Figure 1),
with ,1500 cases reported in the financial year 2010/11 (a 22%
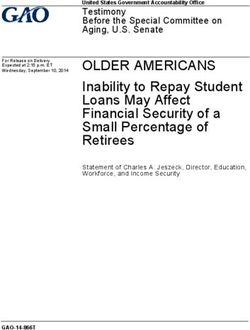
reduction from the number of cases seen in 2009/10 and a 50% Figure 3. Timing of detection of MRSA bloodstream infection in relation
reduction from the number of cases in 2008/09).30 With specific to presentation of patient to reporting Trust, April 2006–March 2008.31
regard to Trust-apportioned cases, there was a 57% reduction in Uncategorized includes regular attenders, accident and emergency
the number cases between 2008/09 and 2010/11, the corre- patients and outpatients.
sponding incidence rates decreasing from 4.3 to 1.8 cases per
100 000 bed days.30
admission (and hence not thought likely to have been acquired
during that admission), the majority (67%) were admitted from
Epidemiology of MRSA bacteraemia home, but a further 18% were admitted from nursing homes
Analysis of patient demographic data has shown that the major- and 8% from another hospital.31 With regard to the last of
ity of MRSA bloodstream infections occurred in elderly patients these findings, the pressure on Trusts to meet the government
(Figure 2), with patients .60 years old accounting for about target of halving their MRSA bacteraemia rates was such that,
three-quarters of cases.31,32 The mean age of patients with on occasion, the early (i.e. within 2 days of admission) isolation
MRSA bacteraemia between 2008 and 2010 was 69 years, with of MRSA from the blood of a patient transferred between hospi-
the mean age in individual months during this time ranging tals occasionally resulted in interhospital disputes as to the loca-
from 65 to 71 years.31,32 For reasons that are not currently tion where the patient developed their MRSA bacteraemia, and
known, MRSA bacteraemia was more common in males than which hospital Trust should take responsibility for reporting the
females, this differential effect being seen in all age groups case. A further study of probable sources of MRSA bacteraemia
(Figure 2). (discussed in more detail below) also found that while bacterae-
Analysis of the timing of detection of MRSA bacteraemia (i.e. mias associated with central venous catheters (CVCs) or other
taking of blood samples for culture) relative to the date of admis- invasive devices were more often seen in cases provisionally
sion to hospital showed that approximately two-thirds of cases classified as hospital-associated on the basis that blood cultures
were detected ≥2 days after admission (Figure 3), which is com- had been taken .2 days after admission, 20% of CVC-associated
monly taken to indicate likely nosocomial infection. Among the MRSA bacteraemias were in cases classified as community-
patients with MRSA bacteraemia occurring within 2 days of associated as their blood cultures were taken within 2 days of
4 of 8Review JAC
Rate per 10000 bed days
3.00
2.50
2.00
1.50
2.00
0.50
0.00
y
cs
e
y
gy
y*
ry
re
y
*
og
er
in
gy
og
di
ge
og
ca
lo
ic
rg
l
ae
lo
ol
ro
ro
ur
ed
ol
rly
su
co
Ur
ph
op
te
at
ls
lm
de
On
ic
en
em
Ne
th
ra
ac
El
ra
ne
ro
or
Ha
or
ne
st
Ge
&
th
Ga
Ge
a
io
m
rd
au
Ca
Tr
Specialty
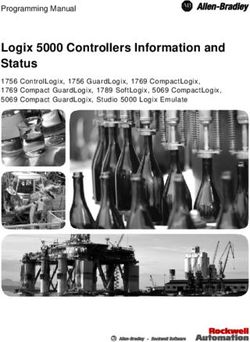
Figure 4. Incidence of MRSA bacteraemia (per 10000 bed days) by specialty in England between April 2006 and March 2008.31 *Specialties clinical
haematology and haematology, and clinical oncology and medical oncology have been combined into haematology and oncology, respectively.
Downloaded from http://jac.oxfordjournals.org/ by guest on July 19, 2015
admission.33 However, the presence of a CVC clearly indicates a marker of healthcare-associated infection in general (despite
recent contact with the healthcare system. Hence, it is not pos- this picture being muddied by the emergence of community-
sible to reliably infer the proportion of MRSA bacteraemias that associated MRSA in the USA).35 The majority of surveillance
are genuinely community-associated, as bloodstream infections schemes collect data on a voluntary basis, but in 2001, the gov-
incubating at the time (or within 2 days) of admission may often ernment in England took the bold step of deciding to make the
have been associated with prior healthcare contact. reporting of MRSA bacteraemia mandatory for all acute hospital
A further analysis of those patients whose bacteraemia was Trusts in light of concerns about the rising incidence and its
detected ≥2 days after admission was undertaken with regard effect on public confidence in national hospitals. This review
to the hospital specialties in which they were being treated. has highlighted how this mandatory surveillance scheme has
The numbers of bed days in a range of hospital specialties was evolved over a 10 year period, from an initial scheme solely col-
derived from the Hospital Episode Statistics available from the lecting data on numbers of blood cultures yielding S. aureus and
NHS Information Centre.34 Using these as the denominator, the the proportion that were MRSA to an enhanced system collecting
incidence of MRSA bacteraemia, expressed as the rate per demographic and clinical data that give considerable insight into
10 000 bed days, was found to vary between specialties, the epidemiology of MRSA bacteraemia. Although not discussed
ranging from 2.48 for nephrology to 0.43 in trauma and ortho- in this review, the same data system has also allowed the man-
paedics (Figure 4).31 However, it is important to bear in mind datory surveillance of intestinal infections caused by Clostridium
that a high incidence of MRSA bacteraemia in a particular spe- difficile and bacteraemia caused by vancomycin-resistant
cialty does not necessarily equate to a large number of such enterococci.
infections, if the number of bed days is relatively low. In terms In contrast to many other national surveillance schemes
of the data shown in Figure 4, the actual counts of MRSA bacter- that report either total national numbers of MRSA infections
aemia were highest in general medicine and general surgery, or the proportion of S. aureus infections that are due to
reflecting the higher numbers of admissions to these specialties MRSA, the mandatory surveillance scheme in England reported
relative to nephrology.31 the incidence of MRSA bacteraemia in individual acute hospital
As mentioned above, from 2006, Trusts have been able to vol- Trusts. This made Trust managers aware of the extent of the
untarily report data on the probable source of the MRSA bacter- problem they faced locally and how it compared with other
aemia. A recent analysis of 4404 episodes of MRSA bacteraemia hospitals. The fact that Trust incidence rates were put in the
reported between 2006 and 2009 showed that nearly half were public domain further served to put both public and political
attributed to intravascular devices (20%) or skin or soft tissue pressure on Trust managers to reduce their rates of MRSA infec-
infection (28%).33 However, there was a significant decline in tions. The well-known definition of surveillance is ‘information
the proportion of bacteraemia associated with invasive devices for action’, and in the case of the mandatory surveillance
such as CVCs and with surgical site infections between 2006 scheme, the information produced was used for rigorous per-
and 2009. This may reflect increased standards of line manage- formance management against the target set by the govern-
ment and surgical wound care introduced when hospitals active- ment, namely the halving of rates of MRSA bacteraemia over
ly sought to reduce their rates of MRSA bacteraemia in response a 3 year period. To enhance the achievement of this target,
to the targets set by the government. the whole panoply of government might and influence was
rolled out, including the involvement of organizations such as
the Healthcare Commission, as well as the full management
Discussion hierarchy of the NHS, including Strategic Health Authorities
Most surveillance systems aimed at healthcare-associated infec- and PCOs. A result of these initiatives was that the issue of
tions or at infections caused by antibiotic-resistant bacteria MRSA rates in individual Trusts was no longer a matter solely
include MRSA, as this pathogen is still often deemed to be for the infection control team and their Chief Executive.
5 of 8Review
The requirement to halve rates of MRSA bacteraemia clearly extent or over the same time frame if there had not been an
had an impact on the surveillance system, as the minimal intense regimen of monitoring and performance managing of
dataset initially collected proved inadequate for allowing Trusts Trusts. While many think this unlikely, hard evidence is difficult
and NHS management above them to determine whether indi- to come by. What does seem clear, however, is that following
vidual patients with MRSA bacteraemia acquired their infection the prominence given to the fight against MRSA, infection
in that Trust (Trust-apportioned cases) or elsewhere, be it control was no longer seen as a backwater but became a key
another Trust or in the community. Thus, enhancements to the quality indicator for Trusts that was increasingly regarded as
dataset were driven by the necessity to determine (attribute) everybody’s business, from the Chief Executive of the Trust
where the infection was acquired, which is crucial for perform- down.
ance management, as interventions aimed at preventing hos- Several aspects of the mandatory surveillance system
pital acquisition of MRSA bacteraemia (e.g. improved line care) described here were innovative. These included the coupling of
are unlikely to prevent the importation of cases. This need epidemiological surveillance with performance management,
for close performance management also made demands on as well as the development of a web-based reporting system
both the timeliness and completeness of the data collection, to enable fast transfer of standard data, with instant, controlled
and contributed to the decision to develop and introduce a access by specified personnel at different levels of the NHS. The
web-enabled system to ensure rapid, accurate and secure data mandatory system also highlights the value of linking the epi-
transmission. demiological numerator data collected via surveillance with
In terms of the 50% reduction in the number cases of MRSA other available datasets, such as the routinely generated infor-
Downloaded from http://jac.oxfordjournals.org/ by guest on July 19, 2015
bacteraemia required by the government, it is notable that this mation on hospital bed occupancy (used as the denominator).
target was met nationally. However, while there was an Other notable aspects of the system include the evolution of a
undoubted decline in the incidence of MRSA bacteraemia (and categorization system for hospitals by case mix to enable fairer
other healthcare-associated infections not discussed here) comparisons and the capture of epidemiological information
there is a question as to whether this can be ascribed to the on patient admission to hospital. However, the dramatic fall in
surveillance system and allied interventions. The answer to MRSA bacteraemia in England means that it is now time to
this is not straightforward, since as with any preventive take stock. Bacteraemia was a useful measure when it was
measure, whether infection control or immunization, the coun- common, and served its purpose in drawing attention to the
terfactual is impossible to prove, as the evidence is largely cir- problem posed by MRSA and the need for rigorous interventions.
cumstantial. It is sometimes stated that the particularly However, now that the prevalence is very low in some hospitals it
‘spreadable’ EMRSA-16 was on the wane and so the incidence would arguably be more worthwhile to use other measures
of MRSA bacteraemia would have dropped naturally. However, for surveillance, such as infections generally, colonization or
this underplays the enormous burden of MRSA infections both.26,37
faced by most hospitals at the time the targets were set, At the start of the mandatory surveillance in 2001, the pro-
when the problem seemed intractable and some healthcare portion of S. aureus bacteraemia in the UK that was due to
workers were even discussing abandoning control measures MRSA was one of the highest in Europe and many were sceptical
against MRSA, arguing that it should be regarded in the same that a reduction in MRSA infections was feasible. The subsequent
way as penicillin-resistant S. aureus. Reflecting this confusion, decline in MRSA bacteraemia seen in England, particularly over
the wide variation in experts’ viewpoints on the appropriate ap- the last 5 years, is testimony to the important role that surveil-
proach to MRSA prevention and control made the 2006 update lance coupled with feedback of data to stakeholders together
of the national MRSA guidelines36 the most difficult to write with political pressure for change can have in reducing rates of
since 1986 (G. D., personal comment). Moreover, although infection.
EMRSA-16 waned, the other major epidemic strain of MRSA
continued in circulation. Hence, it would be presumptuous to
argue that the decline in MRSA was simply due to the waning
of an epidemic strain. Transparency declarations
If it is accepted that the reductions in MRSA bacteraemia A. P. J. is Editor-in-Chief of JAC, but took no part in and did not influence
were in large measure associated with the measures taken by the editorial process. Other authors: none to declare.
hospitals, which elements made a difference? Again, it is diffi-
cult to say, as in many instances multiple measures were intro-
duced simultaneously. For example, it is clear from an
evaluation of the ‘CleanYourHands’ campaign that the procure-
Supplementary data
ment of soap and alcohol hand gel increased, suggesting that Figure S1 is available as Supplementary data at JAC Online (http://jac.
oxfordjournals.org/).
increased levels of hand hygiene may have played a prominent
role.25 Conversely, others have highlighted the likely impact of
decolonization of MRSA carriers.28 There is also debate about
the factors that motivated Trusts to reduce their rates of References
MRSA and other healthcare-associated infections, in particular 1 Johnson AP, Pearson A, Duckworth G. Surveillance and epidemiology of
the role of the government. While the government undoubtedly MRSA bacteraemia in the UK. J Antimicrob Chemother 2005; 56: 455–62.
took a proactive approach, their actions were seen by some as 2 HANSARD 1803–2005. Written Answers — March 11, 1997. http://
punitive. This begs the question as to whether Trusts would hansard.millbanksystems.com/search/mrsa%20nhs?page=4 (28 November
have reduced their rates of MRSA bacteraemia to the same 2011, date last accessed).
6 of 8Review JAC
3 Department of Health. Surveillance of Healthcare Associated Infections, 18 HPA. Quarterly Epidemiological Commentary: Mandatory MRSA
CMO’s Update 30. 2001. http://www.dh.gov.uk/prod_consum_dh/ Bacteraemia and Clostridium difficile Infection (up to April–June 2010).
groups/dh_digitalassets/@dh/@en/documents/digitalasset/dh_4013652.pdf http://www.hpa.org.uk/Topics/InfectiousDiseases/InfectionsAZ/Staphylo
(29 November 2011, date last accessed). coccusAureus/EpidemiologicalData/MandatorySurveillance/HCAIQuart
4 PHLS. First report of the Department of Health’s mandatory MRSA erlyEpidemiology/ (28 November 2011, date last accessed).
bacteraemia surveillance scheme in acute NHS Trusts in England: April 19 HPA. Quarterly Epidemiological Commentary: Mandatory MRSA
to September 2001. CDR Wkly 2002; 12: no. 6, 7 February 2002. http:// Bacteraemia and Clostridium difficile Infection (up to October–December
www.hpa.org.uk/cdr/archives/2002/cdr0602.pdf (28 November 2011, 2010). http://www.hpa.org.uk/Topics/InfectiousDiseases/InfectionsAZ/
date last accessed). StaphylococcusAureus/EpidemiologicalData/MandatorySurveillance/HCAI
5 PHLS. The first year of the Department of Health’s mandatory MRSA QuarterlyEpidemiology/ (28 November 2011, date last accessed).
bacteraemia surveillance scheme in acute NHS Trusts in England: April 20 HPA. Quarterly Epidemiological Commentary: Mandatory MRSA
2001– March 2002. CDR Wkly 2002; 12: no. 25, 20 June 2002. http:// Bacteraemia, Clostridium difficile Infection and MSSA Bacteraemia (up to
www.hpa.org.uk/cdr/archives/2002/cdr2502.pdf (28 November 2011, January–March 2011). http://www.hpa.org.uk/Topics/InfectiousDiseases/
date last accessed). InfectionsAZ/StaphylococcusAureus/EpidemiologicalData/Mandatory
6 HPA. The second year of the Department of Health’s mandatory MRSA Surveillance/HCAIQuarterlyEpidemiology/ (28 November 2011, date last
bacteraemia surveillance scheme in acute NHS Trusts in England: April accessed).
2002– March 2003. CDR Wkly 2003; 13: no. 25, 19 June 2003. http:// 21 HPA. Health Secretary announces MRSA target. CDR Wkly 2004; 14:
www.hpa.org.uk/cdr/archives/2003/cdr2503.pdf (28 November 2011, no. 46, 11 November 2004. http://www.hpa.org.uk/cdr/archives/2004/
Downloaded from http://jac.oxfordjournals.org/ by guest on July 19, 2015
date last accessed). cdr4604.pdf (28 November 2011, date last accessed).
7 HPA. The third year of regional and national analyses of the 22 Department of Health. Reporting MRSA Data: Overview of
Department of Health’s mandatory MRSA surveillance scheme Arrangements. 2006. http://www.dh.gov.uk/en/Publicationsandstatistics/
in England: April 2001– March 2004. CDR Wkly 2004; 14: no. 29, 15 Lettersandcirculars/Professionalletters/Chiefmedicalofficerletters/DH_
July 2004. http://www.hpa.org.uk/cdr/archives/2004/cdr2904.pdf (28 4132578 (28 November 2011, date last accessed).
November 2011, date last accessed). 23 BBC News. MRSA Target ‘Likely to be Missed’. 2007. http://news.bbc.co.
8 HPA. The fourth year of regional and national analyses of the uk/1/hi/6249149.stm (28 November 2011, date last accessed).
Department of Health’s mandatory Staphylococcus aureus surveillance 24 Pearson A, Chronias A, Murray M. Voluntary and mandatory
scheme in England: April 2001– March 2005. CDR Wkly 2005; 15: no. surveillance for methicillin-resistant Staphylococcus aureus (MRSA)
25, 23 June 2005. http://www.hpa.org.uk/cdr/archives/2005/cdr2505. and methicillin-susceptible S. aureus (MSSA) bacteraemia in England.
pdf (28 November 2011, date last accessed). J Antimicrob Chemother 2009; 64 Suppl 1: i11–7.
9 Department of Health. Hospital Activity Team. Guidance/Definitions: 25 Stone S, Slade R, Fuller C et al. Early communication: does a national
KH03 http://www.performance.doh.gov.uk/hospitalactivity/nhsweb/kh03fq. campaign to improve hand hygiene in the NHS work? Initial English and
htm (28 November 2011, date last accessed). Welsh experience from the NOSEC study (National Observational Study
10 Safdar N, Bradley EA. The risk of infection after nasal colonization with to Evaluate the CleanYourHandsCampaign). J Hosp Infect 2007; 66:
Staphylococcus aureus. Am J Med 2008; 121: 310–5. 293–6.
11 Department of Health. NHS to Track Wider Range of Infections. 26 Enoch DA, Cargill JS, Sismey A et al. MRSA surveillance in a UK district
2010. http://www.dh.gov.uk/en/MediaCentre/Pressreleases/DH_120208 hospital: measuring clinical isolates with MRSA is more useful than
(28 November 2011, date last accessed). measuring MRSA bacteraemias. J Hosp Infect 2011; 79: 287–91.
12 Department of Health. Extension of Mandatory Surveillance to Meticillin 27 Department of Health. Saving Lives: Reducing Infection, Delivering
Sensitive Staphylococcus aureus (MSSA) and Updated Healthcare Clean and Safe Care. 2007. http://webarchive.nationalarchives.gov.uk/
Associated Infections Clinical Guidance (HCAI Compendium). 2011. http:// +/www.dh.gov.uk/en/Publicationsandstatistics/Publications/Publications
www.dh.gov.uk/en/Publicationsandstatistics/Lettersandcirculars/Dear PolicyAndGuidance/DH_078134 (28 November 2011, date last accessed).
colleagueletters/DH_123275 (28 November 2011, date last accessed). 28 Edgeworth JD. Has decolonization played a central role in the decline
13 HPA. Quarterly Epidemiological Commentary: Mandatory MRSA in UK methicillin-resistant Staphylococcus aureus transmission? A focus
Bacteraemia and Clostridium difficile Infection (up to July–September on evidence from intensive care. J Antimicrob Chemother 2011; 66
2010). http://www.hpa.org.uk/webc/HPAwebFile/HPAweb_C/1296682346 Suppl 2: 41–7.
613 (28 November 2011, date last accessed). 29 Wyllie D, Paul J, Crook D. Waves of trouble: MRSA strain dynamics and
14 HPA. Mandatory Surveillance of Staphylococcus aureus Bacteraemia. assessment of the impact of infection control. J Antimicrob Chemother
2011. http://www.hpa.org.uk/web/HPAweb&HPAwebStandard/HPAweb_C/ 2011; 66: 2685– 8.
1233906818165 (28 November 2011, date last accessed). 30 HPA. Results From the Mandatory Surveillance of MRSA Bacteraemia,
15 UK Statistics Authority. Code of Practice for Official Statistics. 2009. Acute Trust Counts and Rates by Quarter and Financial Year (FY) - April
http://www.statisticsauthority.gov.uk/assessment/code-of-practice/index. 2007 Onwards. http://www.hpa.org.uk/web/HPAweb&HPAwebStandard/
html (28 November 2011, date last accessed). HPAweb_C/1233906819629 (29 November 2011, date last accessed).
16 HPA. Mandatory Surveillance Weekly Reports. http://www.hpa.org.uk/ 31 HPA. Surveillance of Healthcare Associated Infections Report: 2008.
web/HPAweb&HPAwebStandard/HPAweb_C/1274089052145 (28 November http://www.hpa.org.uk/Publications/InfectiousDiseases/AntimicrobialAnd
2011, date last accessed). HealthcareAssociatedInfections/0807HCAIAnnualReport2008/ (29
17 HM Government. NHS Weekly MRSA Data Set. http://data.gov.uk/ November 2011, date last accessed).
dataset/nhs-meticillin-resistant-staphylococcus-aureus-bacteraemia- 32 HPA. Quarterly Epidemiological Commentary: Mandatory MRSA
dataset-weekly (28 November 2011, date last accessed). Bacteraemia and Clostridium difficile Infection (up to January–March
7 of 8Review
2010). http://www.hpa.org.uk/web/HPAweb&HPAwebStandard/HPAweb_ 35 Tenover FC, Goering RV. Methicillin-resistant Staphylococcus aureus strain
C/1259151891722 (30 November 2011, date last accessed). USA300: origin and epidemiology. J Antimicrob Chemother 2009; 64: 441–6.
33 Wilson J, Guy R, Elgohari S et al. Trends in sources of 36 Coia JE, Duckworth GJ, Edwards DI et al. Guidelines for the control
meticillin-resistant Staphylococcus aureus (MRSA) bacteraemia: data and prevention of meticillin-resistant Staphylococcus aureus (MRSA) in
from the national mandatory surveillance of MRSA bacteraemia in healthcare facilities. J Hosp Infect 2006; 63 Suppl 1: S1– 44.
England, 2006– 2009. J Hosp Infect 2011; 79: 211– 7. 37 Mumtaz S, Bishop LA, Wright AL et al. Burden of meticillin-resistant
34 NHS Information Centre. Hospital Episode Statistics. http://www. Staphylococcus aureus colonization and infection in London acute
hesonline.nhs.uk/Ease/servlet/ContentServer?siteID=1937 (29 November hospitals: retrospective on a voluntary surveillance programme. J Hosp
2011, date last accessed). Infect 2011; 79: 309–12.
Downloaded from http://jac.oxfordjournals.org/ by guest on July 19, 2015
8 of 8You can also read