Theralase Technologies Inc. Roger Dumoulin-White President, Chief Executive Officer AGM Corporate Presentation Theralase Technologies Inc - TLT: ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

CONFIDENTIAL February 17, 2015
Theralase Technologies Inc.
Roger Dumoulin-White
President, Chief Executive Officer
AGM Corporate Presentation
Theralase Technologies Inc. Chapter Title Section
Corporate Presentation – 3Q2017
TLT: TSXV TLTFF: OTC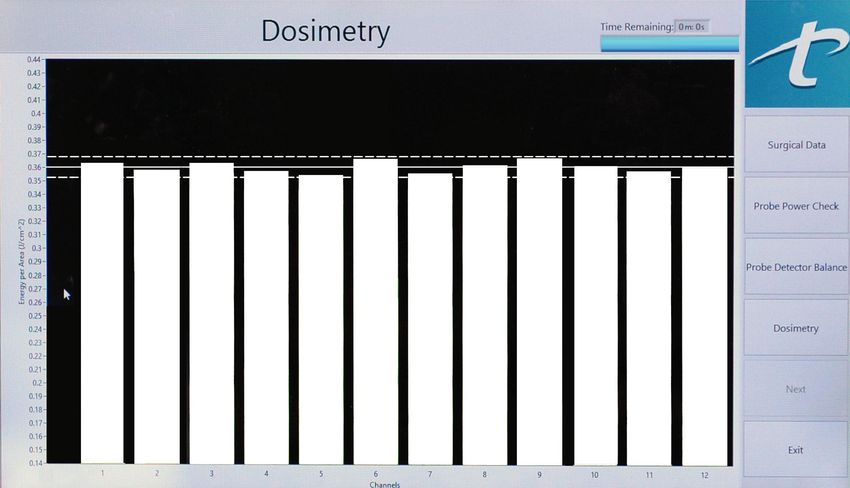
Forward Looking Statements
Certain statements contained or incorporated in this presentation, which deal with the financial condition and operating results of
Theralase Technologies Inc. (“Theralase” or the “Company”), include information, analyses and projections as to future corporate
developments which are currently in the planning stage, and on the projected operating financial performance of the Company, which
constitute forward-looking statements. Such forward-looking statements, made with special reference to the Company’s ongoing
technologically complex healthcare and medical device research and development efforts, which may include in-house and
independent clinical trials, testing new medical technologies and their applications, involve known and unknown risks and
uncertainties that could cause actual events and results to differ materially from those estimated or anticipated and which may have
been implied or expressed in such forward-looking statements.
No conclusions as to the successful outcome of the ongoing and planned research and development projects in which the Company
is involved are intended or implied nor can they be foreseen or predicted prior to definitive corporate announcements as to their
outcome. Certain forward looking statements are identified by words such as “believe”, “anticipate”, “should”, “could”, “would”,
“estimate”, “expect”, “intend”, “plan”, “expect”, “project”, “may”, and “will” and the negative of such expressions, although not all
forward looking statements contain these identifying words, any statements that refer to expectations, projections or other
characterizations of future events or circumstances are forward looking statements. Although Theralase believes that the expectations
reflected in any forward looking statements made in this presentation are reasonable, such statements are based on a number of
assumptions, which may prove to be incorrect; including, but not limited to assumptions related to the risks and factors set out in the
Company’s unaudited and audited financial statements and Management Discussion and Analysis, available at www.sedar.com
Accordingly, no assurances can be given that any of the events or circumstances contemplated by any such forward looking
statements will transpire or occur or, if any of them transpire or occur what impact they will have on Theralase’s results of operations
or financial condition.
Furthermore, the forward-looking statements contained in this presentation are made as of the date hereof. The Company does not
undertake any obligation to update publicly or to revise any of the included forward-looking statements, whether as a result of new
information, future events, or otherwise, unless required by applicable laws. The forward-looking statements contained in this
presentation are expressly qualified by this cautionary statement.
All references to dollars herein are to Canadian dollars except as otherwise indicated.
2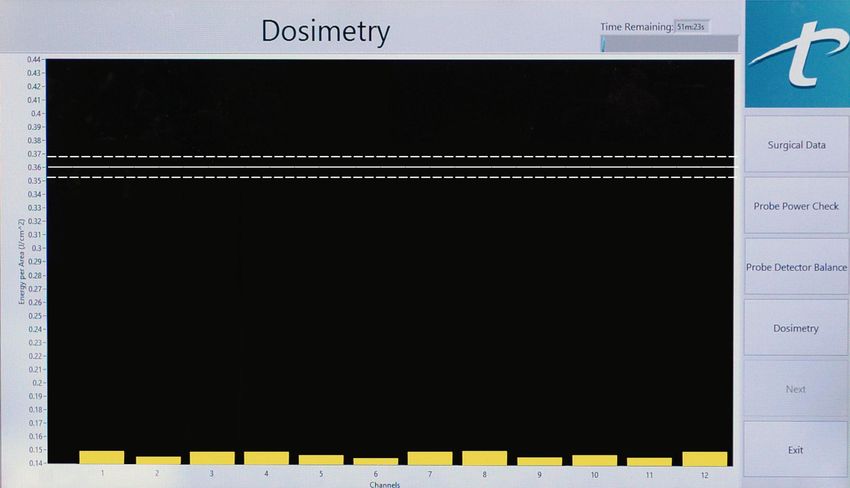
Investor Summary
Investment Considerations:
Anti-Cancer Division –Developing a Photo Dynamic Compound (“PDC”) that has an affinity for cancer
cells and when light activated has been proven clinically to be safe, tolerable and effective in the
treatment of Non-Muscle Invasive Bladder Cancer (“NMIBC”) in the first 3 patients treated in a Phase Ib
clinical study, evaluated at 90 days post treatment. Approved by Data Safety Monitoring Board to enroll 6
additional patients to be treated at a therapeutic dose.
Therapeutic Laser Division – Next generation therapeutic laser able to dramatically increase efficacy
over existing technologies in a $100 B pain management market
Strong Management Team - Proven and experienced management team that has partnered with world
renowned doctors and scientists at leading teaching hospitals
Strong IP Portfolio - 13 issued patents, 25 patents pending at the national phase, 2 pending at the
international PCT phase covering core technologies in both divisions
Risk Diversification and Reward - Combination of clinical stage, future breakthrough anti-cancer
technology and proven commercial therapeutic laser technology, both entering rapid growth periods
Inflection Point - > $30M invested to date in both divisions to develop and commercialize advanced
medical laser technologies to eliminate pain and destroy cancer that are poised for significant growth in
2017 / 2018
3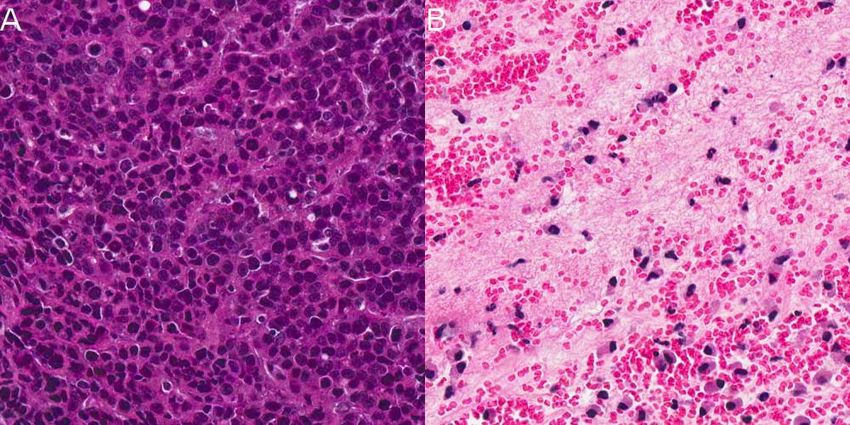
PDT Division
Anti-Cancer Division:
Clinical stage, biotech company that utilizes patented light activated Photo
Dynamic Compounds (“PDCs”), in combination with patent pending laser
technologies, to destroy various cancers with very high efficacy (> 99%)
Nontoxic to healthy tissue with preferential localization inside cancer cells
to effectively destroy them, when exposed to light (virtually 0% toxicity)
Phase Ib clinical study has demonstrated high safety, tolerability and
efficacy in the destruction of NMIBC and preclinically high safety,
tolerability and efficacy in both NMIBC and Glioblastoma Multiforme
(“GBM”) cancers
Phase 1b NMIBC clinical study being conducted at Princess Margaret
Cancer Center, University Health Network (“UHN”), one of the top
research cancer centres in the world
New cancer indications Phase Ib clinical studies to commence in 4Q2017
Able to be activated at various tissue depths allowing “patient specific”
treatments based on anatomical location and progression of cancer
Issued and Pending U.S. Patents Licensed to Theralase: 6,962,910,
7,612,057, 8,148,360, 8,445,475, PCT/US14/30194, 13/863,089,
PCT/US13/36595
4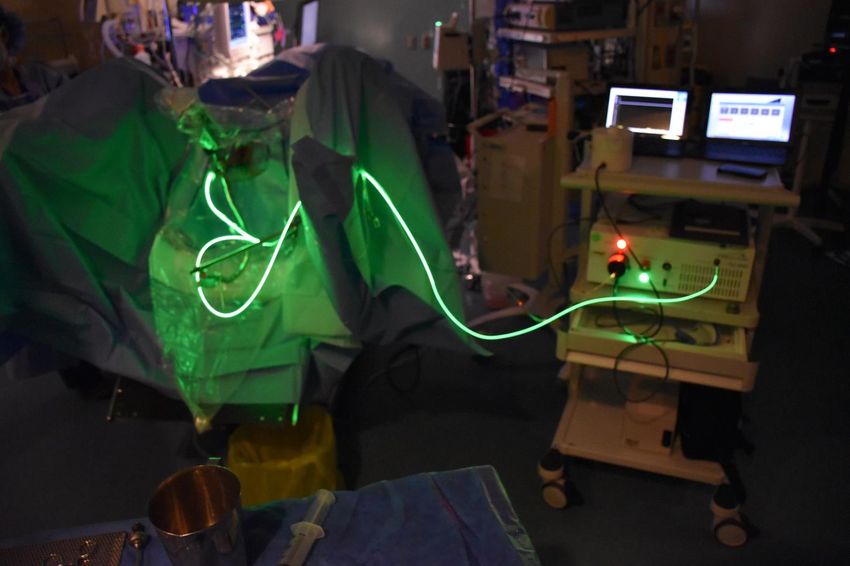
NMIBC (in-vitro)
Safety Efficacy
120
45 J cm-2 120 45 J cm-2
90 J cm-2 90 J cm-2
100 100
80
80
Cell Kill (%)
Cell Kill (%)
60
60
40
40
20
20
0
0
0.00125 0.0025 0.005 0.01 0.02 0.04
0.00125 0.0025 0.005 0.01 0.02 0.04
Concentration (mM)
Concentration (mM)
In-vitro study completed at UHN with HT-1376 (human bladder cancer cell line) with TLD-1433
(Theralase’s lead PDC) comparing cell kill (y axis) versus TLD-1433 concentration (x axis)
Left hand graph: shows HT-1376 cancer cells mixed with various concentrations of TLD-1433, but not
light activated, demonstrating a high safety and tolerability, as there is virtually no cell kill
Right hand graph: shows HT-1376 cancer cells mixed with various concentrations of TLD-1433 and
light activated at two different levels of light (45 J/cm2 and 90 J/cm2) demonstrating up to 100% efficacy
at various concentrations of TLD-1433
5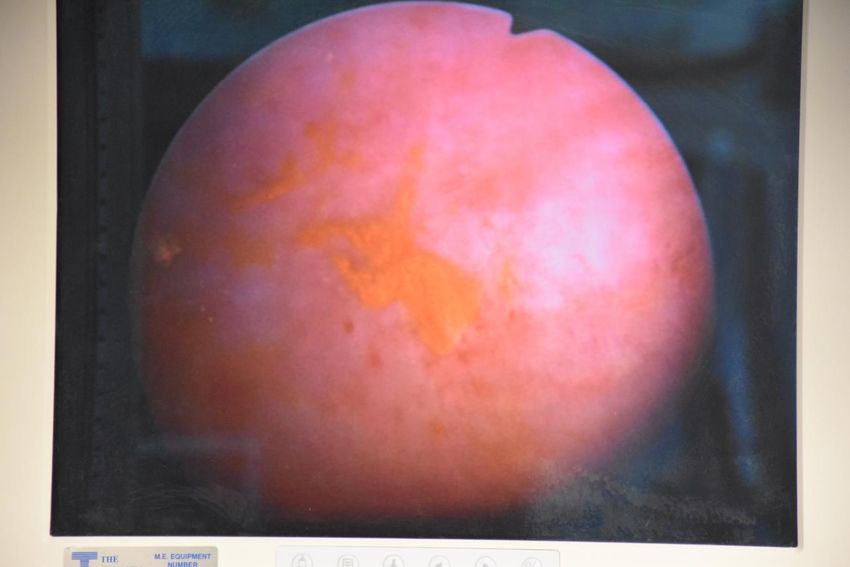
NMIBC (small animal in-vivo)
(>99% destruction of NMIBC tumors)
Left Image indicates elongated bladder removed from orthotopic rat model (in-situ AY-27 rat bladder
cancer cells) after intravesical instillation of TLD-1433 PDC demonstrating that TLD-1433 (yellow
compound) localizes preferentially to bladder cancer tumors at a rate 180 times greater than that of
healthy urothelium. (Arrows indicate localization of TLD-1433 in main bladder cancer tumors and in
microscopic tumors (may indicate why TURBT / BCG procedure has up to 80% recurrence rate
Center Image indicates biopsy of bladder cancer prior to PDT treatment demonstrating 100% viable
bladder cancer cells
Right Image indicates biopsy of bladder cancer after PDT treatment demonstrating virtually 0% viable
bladder cancer cells as verified by histopathology (>>99% destruction of bladder cancer tumors)
6
NMIBC (human)
Study Objectives:
Primary: Evaluate the safety and tolerability of PDT employing the PDC (TLD-1433), Medical Laser
(TLC-3200) and Dosimetry Fibre Optic Cage (“DFOC”) (TLC-3400)
Secondary: Evaluate the PharmacoKinetics (“PK”) (movement and exit of drug within tissue) of TLD-
1433
Exploratory: Evaluate the efficacy of PDT employing TLD-1433, TLC-3200 and TLC-3400
7
Overall Study Design
The Phase Ib NMIBC Clinical Study (“Study”) will consist of 2 phases:
1st phase: 3 subjects to receive PDT employing 0.35 mg/cm2 (Maximum Recommended Starting Dose
“MRSD”)) of TLD-1433. MRSD has not raised significant safety concerns; therefore:
2nd phase: 6 additional subjects will receive PDT with 0.70 mg/cm2 (therapeutic dose) TLD-1433.
8
NMIBC (human)
Preferential accumulation of TLD-1433 in the NMIBC tumour
regions of the bladder wall (post rinse)
9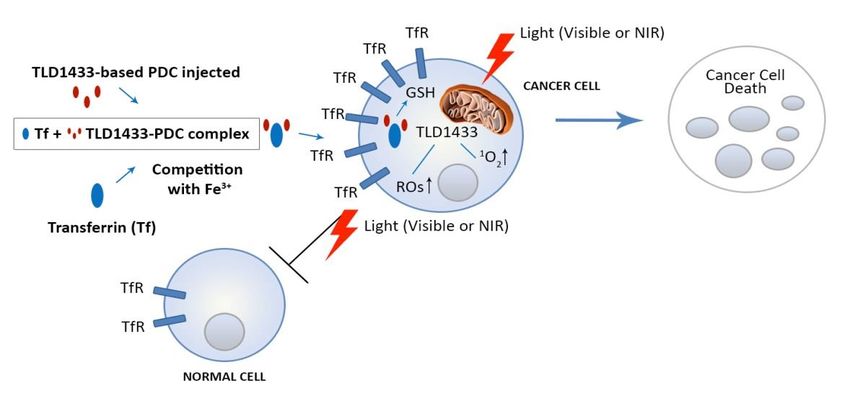
NMIBC (human)
Laser Light Delivery with TLC-3200 & TLC-3400
TLC-3200 Medical Laser System combines laser light delivery and dosimetry via the (TLC-3400)
Dosimetry Fibre Optic Cage (“DFOC”) to deliver laser light energy of a specific wavelength (“nm”) and
energy density (“J/cm2”) to the bladder wall
TLC-3200 visibly signals the surgeon when this irradiation has been achieved and to discontinue
treatment
DFOC allows the surgeon to adjust energy density delivery in direct response to: bladder shape,
volume and diffuse reflectance of the bladder wall, thus providing a consistent energy density to the
patient’s inner bladder wall surface
10Dosimetry Screen - Pre Treatment
11TLC-3200 Treatment Procedure
Bladder illuminated with green laser light (525nm) and treatment discontinued when TLC-3200
confirms delivery of approximately 90 J/cm2. TLC-3200 measures light delivery in real time, ensuring
that the final light dose delivery to the bladder remains at approximately 90 J/cm2.
12Dosimetry Screen - Post Treatment
13Irradiance for First 3 Patients
Average PDT Irradiance Achieved for the first 3 patients
Average Irradiance
(sensors 1 to 6)
Target Dose:
140 90 J/cm2 (+/- 20%)
Irradiance (J/cm2)
120
100
Achieved Dose:
80
90 J/cm2 (+ 10% /- 0%)
60
40
20
0
001 002 003
Patient
14Adverse Events
Subject 001-001 001-002 001-003
1 – Mild (ongoing @ 2 – Moderate
Pelvic Pain nil
day 30) (resolved @ day 6)
2 – Moderate 2 – Moderate
Bladder Spasms nil
(resolved @ day 6) (resolved@ day 21)
1 – Mild (resolved @ 1 – Mild (resolved @
Constipation nil
day 5) day 6)
2 – Moderate
Urge Incontinence nil nil
(resolved @ day 6)
1 – Mild (ongoing @
Fatigue nil nil
day 30)
Eye pain nil nil 1 – Mild (resolved @ day 1)
Penile discomfort nil nil 1 – Mild (resolved @ day 5)
Urinary Frequency nil nil 1 – Mild (resolved @ day 6)
15PK Analysis (TLD-1433)
Concentrations of Ruthenium Complex Concentrations of Ruthenium Complex
in Human Urine in Clinical Samples in Human Plasma in Clinical Samples
1,400 2.5
Concentration [ng/ml]
Concentration [ng/ml]
1,200
2.0
1,000
800 1.5
600 1.0
400
0.5
200
0 0.0
0 8 16 24 32 40 48 56 64 72 0 8 16 24 32 40 48 56 64 72
Time (hours) Time (hours)
Data points represent average TLD-1433 concentrations per ml of sample
(mean +/- standard deviations). n = 3 patients.
16GBM (in-vitro)
Human brain cancer
Safety (Glioblastoma Multiforme) Efficacy
100 100 ALA
Rat brain cancer
Cell Kill (%)
Cell Kill (%)
TPDC
50 (glioma) 50
0 0
0.0001 0.0002 0.0005 0.017
0.0001 0.0002 0.0005 0.017
U87 (Human Glioblastoma Multiforme (“GBM”) brain cancer cell line) and F98 (rat brain glioma cancer
cell line) with TLD-1433 comparing cell kill (y axis) versus TLD-1433 concentration (x axis)
Left hand graphs: U87 and F98 cancer cells mixed with various concentrations of TLD-1433, but not
light activated, demonstrating a high safety and tolerability, as there is virtually no cell kill.
Right hand graphs: U87 and F98 cancer cells mixed with various concentrations of TLD-1433 and light
activated at 90 J/cm2 demonstrating up to 100% efficacy at various concentrations of TLD-1433
ALA has virtually no impact on U87 and F98 cancer cells at these concentrations. Photofrin’s efficacy
drops as the concentration of PDC drops. The current limitation of ALA and Photofrin is that they are
porphyrin based PSs that are predominantly systemically injected and activated by red laser light,
limiting their use to various cancers. Photofrin was approved for bladder cancer in 1993, but has never
been used clinically due to the toxicity and morbidity exhibited to the bladder structure. They also may
render the patient extremely light sensitive for 30 to 90 days post treatment
17GBM (small animal in-vivo)
Sept. 9, 2016: Tumour diameter 1.44 mm (Volume 1.56 mm3) (202% daily
growth rate)
Sept. 10, 2016: Rutherrin® (TLD-1433 PDC (5 mg/kg) + transferrin) is injected
intravenously via the rat’s saphenous tail vein
Sept 11, 2016: 24 hours post injection, Rutherrin® infused animal brain is
exposed to 200 mW/cm2, 808 nm laser light (Total delivered energy 600 J/cm2)
Sept. 20, 2016 (9 days post PDT):Tumour undetectable by MRI
Sept. 30, 2016 (19 days post PDT): Tumour diameter 1.84 mm (Volume 3.26 mm3)
Oct. 7, 2016 (26 days post PDT): Tumor diameter 3.8 mm (Volume 28.74
mm3) (111% daily growth rate)
Oct. 12, 2016 (31 days post PDT): Rat still alive and functioning well.
Current median survival in humans without treatment: 8.1 months (0.7 years1)
Current median survival in humans with extensive treatment (maximal surgical
resection, radiotherapy and concomitant and adjuvant chemotherapy with
temozolomide): 14.1 months or 1.2 years2.
Oct. 22, 2016 (41 days post treatment):
925% survival increase over standard of
care
1 Johnson DR, O'Neill BP (2012) Glioblastoma survival in the United States before and during the temozolomide era. Journal of Neurooncology 107(2):359-64
2 Stupp R, Hegi ME, Gilbert MR, Chakravarti A (2007) Chemoradiotherapy in malignant glioma: standard of care and future directions. Journal of Clinical Oncology 25(26):4127–4136
18Immune Response
First slide – 350,000 colon cancer cells injected into
mouse subcutaneously (below skin surface). Tumor
allowed to grow to approximately 5 mm in diameter and
then 53 mg/kg of TLD-1433 injected intra-tumorly
Second slide – TLD-1433 allowed to absorb into colon
cancer cells for 4 hours. (pre-light activation)
Third slide – 24 hours after light activation, colon
cancer cells demonstrating clear necrosis (cell death)
Fourth slide – same mouse 20 months later (mice only
live 18 to 20 months) demonstrating no cancer cells (no
recurrence) and no scarring (no destruction of healthy
cells). Same mouse cohort injected up to three times
with 350,000 colon cancer cells, with no further
intervention. Cancer is unable to grow suggesting that
the immune system (“Killer T cells”) have memorized
the signature of the colon cancer cells and have
provided an “immune-mediated” response preventing Cancer necrosis
recurrence (cell death)
19Mechanisms of Action Transferrin + PDC targets cancer cells and destroys them Transferrin is a naturally occurring glyco-protein that transports iron to every cell in our body. Iron is a transitional VIII metal, as is Ruthenium and Osmium (main centers of Theralase PDCs) that are indistinguishable by transferrin; therefore, TLD-1433 is able to combine with transferrin to be transported through the blood stream to every cell with a Transferrin Receptor Site (“TfR”). Well documented that cancer cells have a larger number of transferrin receptors versus healthy cells. 3,4 TLD-1433 is preferentially attracted to a wide variety of cancer cells, allowing TLD-1433 to cross the cancer cell cellular membrane into the interior of the cell; whereby, when light activated it produce a very powerful cytotoxic (cell killing) form of singlet oxygen known as Reactive Oxygen Species (“ROS”). 3Transferrin receptor regulates pancreatic cancer growth by modulating mitochondrial respiration and ROS generation. Jeong SM, Hwang S, Seong RH 4A novel transferrin receptor-targeted hybrid peptide disintegrates cancer cell membrane to induce rapid killing of cancer cells. Megumi Kawamoto, Tomohisa Horibe, Masayuki Kohno, Koji Kawakami 20
TLT Division Therapeutic Laser Technology (“TLT”) Division Commercial operating division that designs, develops and sells therapeutic lasers to healthcare practitioners to eliminate pain, reduce inflammation and accelerate tissue healing generating approximately $2 M in revenue annually, minimizing the burn rate and dilution of the PDT division. Clinically proven5 and highly effective, patented Health Canada and FDA cleared commercial cold laser technology indicated for osteoarthritis and knee pain Used by healthcare practitioners, off-label, to treat various nerve, muscle and joint conditions healing patients and professional athletes Healthcare practitioners report that it heals patients safer, faster and more effectively than any other direct or indirect competitive product Legacy technology (TLC-1000) currently installed at approximately 1000 locations in Canada and the US Next Generation Therapeutic Laser (TLC-2000) launched in 2016 5 Marquina, Nelson, Dumoulin-White, Roger, Mandel, Arkady*, Lilge, Lothar, “Laser therapy applications for osteoarthritis and chronic joint pain – A randomized placebo-controlled clinical trial”, Photon Lasers Med 2012; 1(4): 299–307 21
Next Generation Therapeutic Laser
“Cell Sensing®” technology uses patented algorithms to
determine the depth of injury and automatically delivers the
precise amount of laser light required to heal the condition
(Uses set powers and time for chronic knee pain)
Dramatically increases efficacy over existing technologies by
precisely targeting injured tissue
Patients report 90% efficacy rate in healing nerve, muscle and
joint conditions
Rotator cuff clinical study to be commenced with Dr. James
Andrews in 4Q2017
Next generation technology increases efficacy and gross
margins over legacy technology through a recurring revenue
model
22Pain Market
US pain market exceeds $100B annually and
growing rapidly6
45% of this population remain in significant pain
post surgery or prescribed pain medicine7
Patients are seeking alternative treatment
methods as their pain is still present.
Doctors are not prescribing pain medication due
to high addiction rates and government
restrictions
TLC-2000 expected to be eligible for a unique
reimbursable Current Procedural Terminology
(“CPT”) code in the U.S. for national insurance
reimbursement due to Cell Sensing® technology
Allows easier sale of the TLC-2000 to doctors
and physical therapists that rely on CPT codes
to bill, as well as allows access to Medicare and
Medicaid
6 Institute of Medicine of the National Academies Report. Relieving Pain in America: A Blueprint for Transforming Prevention, Care, Education, and Research, 2011. The
National Academies Press, Washington DC.
7
23
Peter D. Hart Research Associates. Page 3. KEY FINDINGS. Americans in Pain.Business Model
Healthcare practitioners charge between $20 to $150 per 15 minute treatment (Average: $50 per
treatment session)
Healthcare practitioners perform between 100 and 500 treatment sessions per month (Average: 200
treatment sessions per month)
Healthcare practitioners generate on average $50 x 200 = $10,000 per month
Theralase TLC-2000 costs between $350 (1 probe) to $1,000 (4 probe + stands) per month* (Average
$500 per month for 2 probe laser system)
Average Monthly Return on Investment
($10,000 / $500 = 20 x or 2000%)
* Monthly cost includes: TLC-2000 product, in-person and video training, lifetime warranty, lifetime marketing support, direct patient referrals and lifetime software updates
24Next Steps
Anti-Cancer Division
Approximate Timing:
2Q2018 - Complete a Health Canada Phase Ib clinical study for NMIBC
1Q2019 - Complete a Health Canada Phase Ib clinical study for additional cancer indication
2Q2020 – Complete a pivotal Health Canada / FDA Phase II clinical study for NMIBC
1Q2021 – Complete a pivotal Health Canada / FDA Phase II clinical study for additional cancer indication
Therapeutic Laser Division
Approximate Timing:
2Q2018 – Expand TLC-2000 sales and marketing team into Canada and the US
25Key Metrics
Market Data (As of August 22, 2017)
Stock Price C$0.475
52 Week High / Low C$0.54/$0.175
Market Capitalization C$59.5 M
Basic Shares Outstanding 125,231,526
Warrants 31,343,075
Options 9,585,000
Fully Diluted Shares Outstanding 166,159,601
Insider Ownership 6.9% (10.9% fully diluted)
26Appendix - Management Team
Roger Dumoulin-White – President & Chief Executive Officer
President and CEO of Theralase Technologies Inc. since 2004 (Theralase Inc. since
1994)
Before founding Theralase Inc., served as a Product Team Manager with Ford
Electronics Manufacturing Corporation, a division of Ford Motor Corporation (NYSE:F),
where he managed a $40 million a year business (subset of $400 million annual
business), with approximately 400 employees reporting to him (subset of 2,500 total
employees)
Graduated from the University of Western (London, Ontario) with a bachelor degree in
Electrical Engineering (B.E.Sc)
Dr. Arkady Mandel – Chief Scientific Officer
One of the key founders of the therapeutic use of lasers in dermatology and other areas
of clinical medicine, as well as the originator and developer of phototherapy methods
Over 100 original papers and scientific monographs to his name, combined with over 200
international patents
Dr. Mandel earned his designation as a medical doctor from the Moscow State Medical
University
Doctor of Science accreditation majored in: biochemistry, microbiology, immunology,
biophysics, and photobiology
27Appendix - TLT Division Advisors
James Andrews, MD
World renowned orthopaedic sports surgeon. Founder of the American Sports Medicine
Institute (“ASMI”) President and Chairman of the Andrews Research and Education
Foundation dedicated to prevention, education and research at the Andrews Institute.
Mentored more than 314 orthopaedic/sports medicine Fellows and more than 84 primary
care sports medicine Fellows who have trained under him through the Sports Medicine
Fellowship Program
Jeffrey Dugas, MD
Orthopaedic sports surgeon. Member of American Academy of Orthopedic Surgeons
(“AAOS”), ASMI, International Cartilage Repair Society, Treats all types of orthopedic
sports injuries, including injuries of the shoulder, elbow and knee, including total joint
replacement surgery of the shoulder and knee
Lyle Cain, MD
Orthopaedic sports surgeon. Specializes in arthroscopy and treatment of sports related
injuries, as well as open and arthroscopic treatment of knee, ankle, shoulder and elbow
injuries. Performs surgical joint replacement for arthritis of the knee and shoulder.
Certified to treat cartilage injuries in the knee with articular cartilage implantation and
meniscal transplantation
Kevin Wilk, DPT
Distinguished career as a clinical physical therapist for the past 29 years and as a leading
authority in rehabilitation of sports injuries and orthopaedic lesions. Provided significant
contributions to laboratory research, bio-mechanical research and clinical outcome
studies
28Appendix - PDT Division Advisors
Michael Jewett, MD: (UHN)
Professor of Surgery (Urology) at the University of Toronto, Surgical Oncology at Princess
Margaret Cancer Centre, University Health Network (“UHN”). Clinical practice is in urologic
oncology with research interests in testicular cancer and superficial bladder cancer
Lothar Lilge, Ph.D.: (UHN)
Professor in the Department of Medical Biophysics, University of Toronto and Senior Scientist
at the Ontario Cancer Institute, UHN. Research is focused on Photo Dynamic Therapy, optical
diagnostics, destruction of cancer and bacteria by light activated PDCs and the use of light as a
microscopic tool for biomedical research
Ashish Kamat, MD: (MD Anderson)
Internationally recognized expert in urologic oncology. Authority in the management of urologic
cancers. Expertise in bladder cancer, organ sparing and minimally invasive techniques.
Maintains an active research portfolio with focus on efforts to develop novel therapies and
identify predictors of response to therapy (i.e.: intravesical immunotherapy), as a first step
towards personalized cancer therapeutics. Initiated, led and active in several large studies
including multinational trials in bladder cancer, findings published in high impact journals
Michael O’Donnell, MD: (University of Iowa)
Uro-oncologist. Long history of focusing on bladder immunology and bladder cancer
immunotherapy, particularly the anti-cancer mechanisms of bacillus Calmette-Guerin (“BCG”)
and its enhancement with combination therapies. Recently headed a national trial of bladder
cancer treatment utilizing BCG plus interferon (a natural protein which induces healthy cells to
combat disease) comprised of over 1,000 patients and holds several U.S. patents for his work
Brian Wilson, Ph.D: (UHN)
Senior Scientist and Head of the Applied Biophotonics group at UHN. Professor in the
Department of Medical Biophysics at the University of Toronto. Research focus of the Applied
Biophotonics group is the development and application of new therapeutic and diagnostic
techniques based on the use of lasers and other optical technologies
29Appendix - TLT Division Research
1.Action of a Diode Laser in Orthopaedics and Traumatology:
http://theralase.com/wp-content/uploads/2014/09/Action-of-Diode-Laser-in-Orthopaedic-and-
Traumatology.pdf
2. A Renaissance in Low-Level Laser Therapy:
http://theralase.com/wp-content/uploads/2014/05/A-Renaissance-in-Low-Level-Laser-light-Therapy.pdf
3.A role of INOS Gene Expression in the Anti-Inflammatory and Tissue Protection Mechanisms of 905
nm Pulse:
http://theralase.com/wp-content/uploads/2014/05/A-Role-of-iNOS-Gene-Expression-in-the-Anti-
inflammatory-and-Tissue-Protective-Mechanisms-of-905-nm-Pulse.pdf
4.In-Vivo Effects of Low Level Laser Therapy on Inducible Nitric Oxide Synthase:
http://theralase.com/wp-content/uploads/2014/05/In-Vivo-Effects-of-Low-Level-Laser-Therapy-on-
Inducible-Nitric-Oxide-Synthase.pdf
5.Laser Therapy Applications for Osteoarthritis and Chronic Joint Pain – A Randomized Placebo
Controlled Clinical Trial:
http://theralase.com/wp-content/uploads/2014/05/Laser-Therapy-Applications-for-Osteoarthritis-and-
Chronic-Joint-Pain-Clinical-Trial.pdf
6.Laser Acupuncture Therapy for the Treatment of Tobacco Addiction:
http://theralase.com/wp-content/uploads/2014/05/Smoking-Cessation-Clinical-Study.pdf
30Appendix - PDT Division Research
1. Arenas, Yaxal, Susan Monro, Ge Shi, Arkady Mandel, Sherri McFarland, and Lothar Lilge. 2013.
“Photodynamic Inactivation of Staphylococcus Aureus and Methicillin-Resistant Staphylococcus
Aureus with Ru(II)-Based Type I/type II Photosensitizers.” Photodiagnosis and Photodynamic
Therapy 10 (4): 615–25. doi:10.1016/j.pdpdt.2013.07.001.
2. Fong, Jamie, Kamola Kasimova, Yaxal Arenas, Pavel Kaspler, Savo Lazic, Arkady Mandel, and
Lothar Lilge. 2015. “A Novel Class of Ruthenium- Based Photosensitizers Effectively Kills in Vitro
Cancer Cells and in Vivo Tumors.” Photochemical & Photobiological Sciences: Official Journal of
the European Photochemistry Association and the European Society for Photobiology 14 (11): 2014–
23.doi:10.1039/c4pp00438h.
3. Holder, Alvin A., David F. Zigler, Maria T. Tarrago-Trani, Brian Storrie, and Karen J. Brewer. 2007.
“Photobiological Impact of [{(bpy)2Ru(dpp)}2RhCl2]Cl5 and [{(bpy)2Os(dpp)}2RhCl2]Cl5 [bpy=2,2’-
Bipyridine; dpp=2,3-Bis(2-Pyridyl)pyrazine] on Vero Cells.” Inorganic Chemistry 46 (12): 4760–62.
doi:10.1021/ic0619916.
4. Kaspler, Pavel, Savo Lazic, Sarah Forward, Yaxal Arenas, Arkady Mandel, and Lothar Lilge. 2016.
“A Ruthenium(ii) Based Photosensitizer and Transferrin Complexes Enhance Photo-Physical
Properties, Cell Uptake, and Photodynamic Therapy Safety and Efficacy.” Photochemical &
Photobiological Sciences: Official Journal of the European Photochemistry Association and the
European Society for Photobiology 15 (4): 481– 95. doi:10.1039/c5pp00450k.
5. Lincoln, Richard, Lars Kohler, Susan Monro, Huimin Yin, Mat Stephenson, Ruifa Zong, Abdellatif
Chouai, et al. 2013. “Exploitation of Long- Lived 3IL Excited States for Metal-Organic Photodynamic
Therapy: Verification in a Metastatic Melanoma Model.” Journal of the American Chemical Society 135
(45): 17161–75. doi:10.1021/ja408426z.
31Appendix - PDT Division Research
6. Reichardt, Christian, Mitch Pinto, Maria Wächtler, Mat Stephenson, Stephan Kupfer, Tariq
Sainuddin, Julien Guthmuller, Sherri A. McFarland, and Benjamin Dietzek. 2015. “Photophysics of
Ru(II) Dyads Derived from Pyrenyl-Substitued Imidazo[4,5-f][1,10]phenanthroline Ligands.” The
Journal of Physical Chemistry. A 119 (17): 3986–94. doi:10.1021/acs.jpca.5b01737.
7. Shi, Ge, Susan Monro, Robie Hennigar, Julie Colpitts, Jamie Fong, Kamola Kasimova, Huimin Yin,
et al. 2015. “Ru(II) Dyads Derived from α- Oligothiophenes: A New Class of Potent and Versatile
Photosensitizers for PDT.” Coordination Chemistry Reviews 282-283 (January): 127– 38.
doi:10.1016/j.ccr.2014.04.012.
8. Stephenson, Mat, Christian Reichardt, Mitch Pinto, Maria Wächtler, Tariq Sainuddin, Ge Shi, Huimin
Yin, et al. 2014. “Ru(II) Dyads Derived from 2-(1-Pyrenyl)-1H-imidazo[4,5-f][1,10]phenanthroline:
Versatile Photosensitizers for Photodynamic Applications.” The Journal of Physical Chemistry. A 118
(45): 10507–21. doi:10.1021/jp504330s.
9. Yin, Huimin, Mat Stephenson, Jordan Gibson, Eric Sampson, Ge Shi, Tariq Sainuddin, Susan
Monro, and Sherri A. McFarland. 2014. “In Vitro Multiwavelength PDT with 3IL States: Teaching Old
Molecules New Tricks.” Inorganic Chemistry 53 (9): 4548–59. doi:10.1021/ic5002368.
32Appendix - Key Customers
Business relationships with world-class organizations:
Research Institutions
Sports Teams and Organizations
33Appendix - Bladder Cancer
Bladder Cancer by the Numbers:8, 9,10
$3.9 Billion (2016), 76,960 new cases, 16,390 deaths in the US each year
Bladder cancer starts from the inside of the organ and grows into the organ,
making it a prime target for intravesical PDT
5th most common cancer, 4th in men, 8th in women
70% of new bladder cancer cases are early stage disease and 90% of bladder
cancers are Transitional Cell Carcinoma (“TCC”)
Current Standard of Care:5
Early stage disease (Carcinoma In-Situ (“CIS”), Ta, T1): Trans Urethral Resection of the Bladder
Tumour (“TURBT”) followed by treatment with bacillus Calmette-Guérin (“BCG”) – 5 year survival rate of
96%
Mid Stage disease (T2, T3a/b): Entire bladder removed along with nearby reproductive organs and
lymph nodes in a procedure called a radical cystectomy - 5 year survival rate of 34 to 70% depending
on progression of disease
Late stage disease (T4): Disease has spread to distant sites, such as the bones, liver and lungs and is
generally regarded as incurable - 5 year survival rate of 5%
8 American Cancer Society
9 http://www.cancer.net/cancer-types/bladder-cancer/statistics
10 National Cancer Institute
34Appendix - NMIBC Clinical Trial
Title:
A Phase Ib Trial of Intravesical Photodynamic Therapy in Patients with Non-Muscle Invasive Bladder Cancer at High Risk
of Progression Who are Refractory to Therapy with Bacillus Calmette-Guerin (“BCG”) and Who are Medically Unfit for or
Refuse a Cystectomy
Objectives:
Primary: Evaluate the safety of PDT employing TLD1433 and controlled uniform laser light (TLC-3200 System) in
subjects with high risk, Ta/T1 or Tis non-muscle invasive bladder cancer (“NMIBC”) that are intolerant or refractory to
BCG, and who are not candidates or refuse radical cystectomy
Secondary: Evaluate the pharmacokinetics (PK) of TLD1433
Exploratory: Efficacy of PDT employing TLD1433 and controlled uniform laser light (TLC-3200 System)
Methodology:
Phase Ib, open-label, single-arm, single-center study conducted in Canada. BCG intolerance or refractory disease are
defined as inability to tolerate or failure to achieve a tumour-free state after at least one induction (a minimum of 5
instillations) followed by either a second induction (a minimum of 5 instillations) or at least 2 maintenance instillations.
Subjects experiencing disease relapse within 12 months or less after finishing the second course of BCG therapy are also
considered refractory. 2 phases: In the first phase, 3 subjects will receive PDT (TLC-3200 System) employing 0.35
mg/cm2 (maximum recommended starting dose) TLD1433. If treatment with the maximum recommended starting dose
does not raise significant safety concerns, as determined by the safety monitoring committee, an additional 6 subjects will
receive PDT with 0.70 mg/cm2 (therapeutic dose) TLD1433
NMIBC PDT Treatment:
•Insert catheter into urethra and install PDC into bladder intravesically for 60 minutes to allow localization into bladder
cancer cells
•Flush bladder to remove any non-adhering PDC
•Insert rigid cystoscope through urethra into bladder, fill bladder with distilled water, insert fibre optic bundle and activate
PDC for 30 to 120 minutes
•Void bladder to remove sterile water
35You can also read

















































