Primary intra-osseous liposarcoma of the femur: a case report
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Journal of Orthopaedic Surgery 2009;17(3):374-8
Primary intra-osseous liposarcoma of the
femur: a case report
Simon Macmull, Henry Dushan Edward Atkinson, Srdjan Saso, Roberto Tirabosco, Paul O’Donnell, John Andrew
Skinner
Royal National Orthopaedic Hospital, Brockley Hill, Stanmore, Middlesex, United Kingdom
the 16-month follow-up, he remained independently
ambulatory, with no local or distant recurrence. Tissue
ABSTRACT diagnosis and multimodal imaging, rather than any
single radiological investigation, are important in
We report a rare case of an intra-osseous liposarcoma making the diagnosis.
of the proximal femur. A 26-year-old man presented
with a 6-month history of left groin pain radiating to Key words: chemotherapy, adjuvant; femur; limb salvage;
the knee and an antalgic gait. Radiology showed a liposarcoma
predominantly fatty lesion in the medial aspect of the
femoral neck extending toward the lesser trochanter;
most of the marrow in the femoral neck had been CASE REPORT
replaced without evidence of an extra-osseous
mass; and the posterior cortex had been destroyed. In June 2007 a 26-year-old man presented with a 6-
Histological and immunohistochemical analyses of month history of left groin pain radiating to the knee
the tumour after open biopsy were indicative of high- and an antalgic gait. He had no signs of systemic
grade liposarcomatous malignancy. After exclusion disease or any history of trauma. Radiology showed a
of any other primary tumour foci or metastases predominantly fatty lesion in the medial aspect of the
on regional and whole-body magnetic resonance femoral neck extending toward the lesser trochanter;
images, the diagnosis of a high-grade intra-osseous most of the marrow in the femoral neck had been
primary liposarcoma of the proximal femur was replaced without evidence of an extra-osseous mass;
made. The patient received 2 preoperative courses of and the posterior cortex had been destroyed (Fig.
neoadjuvant doxorubicin, cisplatin and methotrexate. 1). These aggressive features were unusual for an
After proximal femoral replacement following en indolent tumour such as an intra-osseous lipoma.
bloc excision of the proximal femur, 4 more cycles of A fluoroscopy-guided biopsy failed to obtain
adjuvant ifosfamide and etoposide were given. At adequate tissue for an accurate diagnosis, but the
Address correspondence and reprint requests to: Mr Simon Macmull, Royal National Orthopaedic Hospital, Brockley Hill,
Stanmore, Middlesex, HA7 4LP, United Kingdom. E-mail: simonmacmull@hotmail.comVol. 17 No. 3, December 2009 Primary intra-osseous liposarcoma of the femur 375
Figure 1 Multimodal radiology showing a fatty lesion in the femoral neck (arrow), with destruction of the posterior femoral
neck.
histology suggested an aggressive fat-containing Immunohistochemistry showed that the tumour
neoplasm. An open biopsy and curettage was cells were negative for SM-actin, desmin, CD45, and
performed, followed by polymethylmethacrylate pankeratin MNF116, thus excluding smooth muscle,
cementation and stabilisation with a dynamic hip screw neural, haematological and epithelial malignancies,
(Fig. 2). The postoperative course was complicated by respectively. Nonetheless, S100 immunostaining was
a small pulmonary embolus (confirmed by computed positive in the well-differentiated fatty component
tomographic pulmonary angiography), and oral indicating a liposarcomatous malignancy: either
anticoagulation was prescribed. a primary intra-osseous liposarcoma or a bony
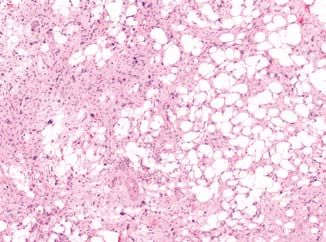
Microscopically, the lesion did not contain metastasis from a primary soft-tissue sarcoma.
osteoid or cartilaginous malignant differentiation. Further staging radiological investigations of the
It comprised lobules of well-differentiated adipose chest and whole body excluded any extra-osseous
tissue intermingled with atypical spindle cells spread of the tumour or other primary or metastatic
with pleomorphic nuclei (Fig. 3). Lipoblasts lesions elsewhere.
and numerous atypical mitoses were identified. The patient received 2 cycles of neoadjuvant
The fatty tissue showed scattered enlarged and doxyrubicin, cisplatin, and methotrexate to reduce the
hyperchromatic nuclei. There was no evidence of tumour size. In October 2007, he underwent a proximal
malignant osteoid or cartilaginous differentiation. femoral replacement following en bloc excision of the
Figure 2 C e m e n t a t i o n
and stabilisation with a Figure 3 Histological examination showing the high-grade
dynamic hip screw after spindle cells intermingled with lobules of well-differentiated
curettage. adipose tissue (H&E, 5x).376 S Macmull et al. Journal of Orthopaedic Surgery
Figure 4 En bloc excision of the proximal femur shows
cement material surrounded by residual fatty tumour Figure 5 A proximal femoral replacement is performed
(arrow). following en bloc excision of the proximal femur with the
dynamic hip screw in situ.
proximal femur with the dynamic hip screw in situ prognosis than osteosarcomas.
(Figs. 4 and 5). A repeated histopathological analysis Of 23 cases of intra-osseous liposarcoma reviewed
confirmed the diagnosis of a 7x3-cm, high-grade (Table), no single treatment appeared to be wholly
intramedullary liposarcoma. The patient made a good effective. Outcomes were extremely poor following
postoperative recovery and had 4 cycles of adjuvant radiotherapy alone; outcomes tended to be better
ifosfamide 14 g/m2 and etoposide 500 mg/m2. The in those who had radical surgery (amputations
fourth cycle was reduced by 20% due to suggestions rather than resections). 11 (48%) patients died after a
of renal failure on blood chemistry. At the 16-month mean of 12 (range, 2–36) months, whereas 12 (52%)
follow-up, he remained independently ambulatory, were alive at a mean follow-up of 33 (range, 5–144)
with no recurrence. months. 13 patients developed distant metastases
following treatment, and one died from the disease
after only 3 months.25 Liposarcoma of the humerus
DISCUSSION appeared to have the worst outcome; those affecting
the tibia appeared to have better survival rates,
Liposarcomas are uncommon tumours of primitive similar to the pattern seen in soft-tissue liposarcomas
mesenchymal derivation occurring mostly in adults,1–4 where survival rates are better in patients with lower-
with an annual incidence of 2.5 per million in the US. extremity tumours.36 Only one patient had a follow-
They account for 10 to 15% of soft-tissue sarcomas.5 up period of >5 years,1 thus no long-term survival
Primary liposarcomas of the bone, arising from can be inferred. No conclusions can be drawn about
lipoblasts in the fatty bone marrow, are extremely rare variations in prognosis based on tumour grade or
and constituteVol. 17 No. 3, December 2009 Primary intra-osseous liposarcoma of the femur 377
Table
A literature review of primary liposarcoma of the bone
Study Patient age Tumour Enneking Treatment Metastasis or Outcome*
(years)/sex site stage at recurrence (months)
presentation
Barnard,15 1934 30/F Humerus M1 Amputation (wide) Lung DOD (2)
Johnson et al.,14 1962 25/M Humerus M0 Amputation (wide) Lung DOD (26)
Johnson et al.,14 1962 46/M Humerus M0 Amputation (wide) Lung DOD (18)
Addison and Payne,17 1982 19/M Humerus M0 Amputation (wide), Lung DOD (10)
radiotherapy,
chemotherapy
Torigoe et al.,3 2006 38/F Humerus M0 Resection (wide) Liver DOD (3)
Duffy and Stewart,11 1938 49/M Femur M1 Amputation (wide), No ANED (60)
radiotherapy
Stojanovic et al.,1 2007 58/M Femur M0 Amputation (wide), Multiple AWED (144)
radiotherapy,
chemotherapy
Cremer et al.,10 1981 n/a Femur M0 Amputation (wide) No ANED (30)
Larsson et al.,7 1975 52/F Femur M1 Radiation Lung DOD (5)
Torok et al.,9 1983 34/M Femur M1 Resection (wide), Lung DOD (16)
radiotherapy,
chemotherapy
Dawson,12 1955 28/F Femur M0 Amputation (wide) Lung DOD (11)
Retz,20 1961 40/M Tibia M0 Amputation (wide) No ANED (24)
Schwartz, et al.18 1970 49/M Tibia M0 Amputation (wide) No ANED (7)
Catto and Stevens,17 1963 16/F Tibia M0 Amputation (wide) Lung AWED (9)
Schneider et al.,22 1980 69/M Fibula M0 Amputation (wide) No ANED (24)
Ross and Hadfield,21 1968 15/M Fibula M1 Resection (marginal), Lung DOD (5)
radiotherapy
Hamlat et al.,24 2005 45/F Thoracic M0 Resection (marginal), Lung and ribs AWED (19)
spine radiotherapy
Lmejjati et al.,25 2008 35/M Lumbar M0 Resection (intralesional), Locally DOD (3)
spine radiotherapy invasive
Kenan et al.,26 1991 57/M Scapula M0 Curettage (marginal) No ANED (36)
Goldman,23 1964 33/M Ulna M0 Amputation (wide) No ANED (5)
Cremer et al.,10 1981 - Ilium M0 Radiotherapy, chemo- Locally DOD (36)
therapy invasive
Seo et al.,28 2007 69/M Temporal M0 Resection (marginal) No ANED (24)
Present study, 2009 26/M Femur M0 Resection (wide), No ANED (16)
chemotherapy
* DOD denotes dead of disease, ANED alive with no evidence of disease, AWED alive with evidence of disease
monthly for 10 years.33,36 This case emphasises the radiological imaging, rather than relying on any
importance of a tissue diagnosis and multimodal single investigation.
REFERENCES
1. Stojanovic M, Goldner B, Djukic S. Unusual biological behaviour of femoral liposarcoma. Srp Arh Celok Lek 2007;135:468–
71.
2. Rabah R, Lucas DR, Farmer DL, Ryan JR, Ravindranath Y. Primary liposarcoma of bone in an adolescent: a case report. Int
J Surg Pathol 1999;7:45–52.
3. Torigoe T, Matsumoto T, Terakado A, Takase M, Yamasaki S, Kurosawa H. Primary pleomorphic liposarcoma of bone: MRI
findings and review of the literature. Skeletal Radiol 2006;35:536–8.
4. Bosman C, Boldrini R, Guzzanti V. Primary osteoliposarcoma of bone. First observation in the pediatric age group. Appl
Pathol 1988;6:56–60.
5. US National Cancer Institute’s Surveillance, Epidemiology, and End Results (SEER) Programme. Available at: http://seer.
cancer.gov. Accessed in 2002.378 S Macmull et al. Journal of Orthopaedic Surgery
6. Rosenberg AE. Liposarcoma of bone, in WHO classification of tumours. Fletcher CD, Unni KK, Mertens F, editors. Lyon:
IARC Press; 2002.
7. Larsson SE, Lorentzon R, Boquist L. Primary liposarcoma of bone. Acta Orthop Scand 1975;46:869–76.
8. Zhou WX. Primary liposarcoma of the long bone (report of 3 cases) [in Chinese]. Zhonghua Fang She Xue Za Zhi
1988;22:151–3.
9. Torok G, Meller Y, Maor E. Primary liposarcoma of bone. Case report and review of the literature. Bull Hosp Jt Dis Orthop
Inst 1983;43:28–37.
10. Cremer H, Koischwitz D, Tismer R. Primary osteoliposarcoma of bone. J Cancer Res Clin Oncol 1981;101:203–11.
11. Duffy J, Stewart FW. Primary liposarcoma of bone. Report of a case. Am J Pathol 1938;14:621–6.
12. Dawson EK. Liposarcoma of bone. J Pathol Bacteriol 1955;70:513–20.
13. Tatic V, Cerovic S, Skaro-Milic A, Jovanovic Z. Primary liposarcoma of bone [in Serbian]. Vojnosanit Pregl 2001;58:91–3.
14. Johnson LC, Vetter H, Putschar WG. Sarcomas arising in bone cysts. Virchows Arch Pathol Anat Physiol Klin Med
1962;335:428–51.
15. Barnard L. Primary liposarcoma of bone. Arch Surg 1934;29:560–5.
16. Pardo-Mindan FJ, Ayala H, Joly M, Gimeno E, Vazquez JJ. Primary liposarcoma of bone: light and electron miscroscopic
study. Cancer 1981;48:274–80.
17. Addison AK, Payne SR. Primary liposarcoma of bone. Case report. J Bone Joint Surg Am 1982;64:301–4.
18. Schwartz A, Shuster M, Becker SM, Amboy P. Liposarcoma of bone. Report of a case and review of the literature. J Bone
Joint Surg Am 1970;52:171–7.
19. Catto M, Stevens J. Liposarcoma of bone. J Pathol Bacteriol 1963;86:248–53.
20. Retz LD Jr. Primary liposarcoma of bone: report of a case and review of the literature. J Bone Joint Surg Am 1961;43:123–
9.
21. Ross CF, Hadfield G. Primary osteo-liposarcoma of bone (malignant mesenchymoma). Report of a case. J Bone Joint Surg
Br 1968;50:639–43.
22. Schneider HM, Wunderlich T, Puls P. The primary liposarcoma of the bone. Arch Orthop Trauma Surg 1980;96:235–9.
23. Goldman RL. Primary liposarcoma of bone: report of a case. Am J Clin Pathol 1964;42:503–8.
24. Hamlat A, Saikali S, Gueye EM, Le Strat A, Carsin-Nicol B, Brassier G. Primary liposarcoma of the thoracic spine: case
report. Eur Spine J 2005;14:613–8.
25. Lmejjati M, Loqa C, Haddi M, Hakkou M, BenAli SA. Primary liposarcoma of the lumbar spine. Joint Bone Spine
2008;75:482–5.
26. Kenan S, Lewis MM, Abdelwahab IF, Hermann G, Klein MJ. Case report 652: primary intraosseous low grade myxoid
sarcoma of the scapula (myxoid liposarcoma). Skelet Radiol 1991;20:73–5.
27. Srivastava KP, Chandra SH, Sharma RD, Agarwal BM. Primary liposarcoma of the skull. Int Surg 1976;61:234.
28. Seo T, Nagareda T, Shimano K, Saka N, Kashiba K, Mori T, et al. Liposarcoma of temporal bone: a case report. Auris Nasus
Larynx 2007;34:511–3.
29. Agarwal PN, Mishra SD, Pratap VK. Primary liposarcoma of the mastoid. J Laryngol Otol 1975;89:1079–82.
30. Nakanishi K, Kobayashi M, Nakaguchi K, Kyakuno M, Hashimoto N, Onishi H, et al. Whole-body MRI for detecting
metastatic bone tumor: diagnostic value of diffusion-weighted images. Magn Reson Med Sci 2007;6:147–55.
31. Pearlstone DB, Pisters PW, Bold RJ, Feig BW, Hunt KK, Yasko AW, et al. Patterns of recurrence in extremity liposarcoma:
implications for staging and follow-up. Cancer 1999;85:85–92.
32. Skubitz KM, D’Adamo DR. Sarcoma. Mayo Clin Proc 2007;82:1409–32.
33. Delshad E, Spanknebel K, Ratner D. Surgical capsules: diagnosis and management of liposarcoma. Skinmed 2004;3:222–
4.
34. Potter DA, Glenn J, Kinsella T, Glatstein E, Lack EE, Restrepo C, et al. Patterns of recurrence in patients with high-grade soft-
tissue sarcomas. J Clin Oncol 1985;3:353–66.
35. Issakov J, Soyfer V, Kollender Y, Bickels J, Meller I, Merimsky O. Liposarcoma in adult limbs treated by limb-sparing surgery
and adjuvant radiotherapy. J Bone Joint Surg Br 2006;88:1647–51.
36. Whooley BP, Gibbs JF, Mooney MM, McGrath BE, Kraybill WG. Primary extremity sarcoma: what is the appropriate follow-
up? Ann Surg Oncol 2000;7:9–14.You can also read