Revisiting Oto-acoustic Emissions
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
REVIEW
Revisiting Oto-acoustic Emissions
Leonard Jie Min Soh, MBBS, MRCS, Yew Meng Chan, MBBS, FRCS, FAMS
Department of Otorhinolaryngology, Singapore General Hospital, Singapore
ABSTRACT
Oto-acoustic emissions (OAEs) are an audiometric diagnostic test that allows quick objective measure of hair cell
function in the inner ear. It is a reflection of hearing function at the interface of conductive and sensorineural
components in the human ear. Unfortunately, it is not commonly used due to the unique expertise and niche
equipment required to successfully carry it out. This article is to further shed light about the use of such tests
to junior doctors so that such resources can be better utilised. It also reviews the current and possible future
applications of OAEs at the frontiers in otology today.
Keywords: Oto-acoustic emissions, TEOAE, DPOAE
INTRODUCTION battery. It is a means of non-invasively acquiring
The Singapore General Hospital ENT hearing centre information about disorders of an essential element
has an armamentarium of audiological resources to of sound processing and hence allows assessment
help establish hearing thresholds accurately and to of loss of sensitivity, compression, and frequency-
determine the presence of impairment; site, type selectivity of the hearing organ. They are a fast and
(conductive, sensorineural or mixed) and severity easy-to-handle method for objectively examining
of the hearing loss. Tests are mainly divided into cochlear function.
behavioural (pure tone and speech) and objective
(tympanometry, auditory evoked potentials, Present OAEs in an ear indicate many things about
otoacoustic emissions etc.) the auditory system. First, they tell us that the
conductive mechanism of the ear is functioning
By and far, the workhorse audiological properly. This includes proper forward and reverse
investigations of choice are mainly behavioural transmission, no blockage of the external auditory
pure tone and speech audiometry testing which canal, normal tympanic membrane movement,
requires the cooperation of the patient. However, and a functioning impedance matching system.
objective tests such as the acoustic reflexes and Present OAEs also indicate that outer hair cell
oto-acoustic emissions (OAEs) are not commonly (OHC) function is normal, which, in most cases,
used due to the unique expertise and niche correlates with normal hearing sensitivity.
equipment required to successfully carry it out. Subjective tests such as pure tone audiometry, are
only able to assess disorders of sound processing
Oto-acoustic emission measurements are a as a whole. Tympanometry, OAEs, and auditory
standard part of the audiological diagnostic test brainstem responses (ABRs), in combination, allow
86 Proceedings of Singapore Healthcare Volume 24 Number 2 2015Revisiting OAEs
for a differentiation between sound-conductive, provide a means of conveying vibrational energy
cochlear, and neural hearing loss. Minute changes back to the middle ear in a reversal of the process
in hearing capability are detectable by OAEs. They that normally delivers auditory stimulation to the
are therefore a suitable means for detecting early hair cells. Theses sounds can be picked up and
impairment, for example, caused by noise exposure recorded by a sensitive microphone fitted in the ear
or ototoxic drugs, as well as for monitoring hearing canal. Most patients with cochlear sensorineural
recovery after a sudden hearing loss. They are also hearing impairment have a loss of this amplification
the first choice investigations for newborn hearing mechanism.
screening programs around the world. They are
easy to obtain, non-invasive, and provide reliable Oto-acoustic emissions are generated only when
information regarding cochlear status in a relatively the organ of corti and the middle ear are in near
short time. With all its benefits, OAE testing does normal conditions; Being able to reach as loud as
have some limitations; It does not evaluate the 30dB SPL. They measure specifically cochlear hair
inner hair cells (IHC), 8th cranial nerve function, function in the peripheral auditory system.
ascending central auditory pathway, or auditory
processing function. Thus, they are not always used HISTORY OF OAEs
in isolation. Oto-acoustic emissions were discovered in July
1977 by Professor David Kemp, a physicist working
THE SCIENCE BEHIND OAEs at the Royal National Ear, Nose and Throat Hospital
Oto-acoustic emissions are air pressure fluctuations at that time1. Kemp was conducting psychoacoustic
in the ear canal caused by vibration of the experiments on his own ears measuring changes
eardrum driven by the cochlea. It is a common in hearing thresholds and loudness perception
misconception to think of OAE as sounds “emitted” associated with small changes in frequency. He
by the cochlea itself, but technically sound pressure was motivated by his observations that hearing
is not produced in any measurable quantity until thresholds exhibited periodic patterns of peaks and
the eardrum, driven by the cochlea, vibrates against valleys, as did loudness estimates, when measured
the adjacent air in the ear canal. The physical in small increments of frequency. Interestingly,
construction of the middle ear positively helps us the valleys in hearing thresholds (frequencies
to observe OAEs. The efficient coupling that the where hearing appeared to be most sensitive)
middle ear provides between the low impedance approximately aligned with peaks in loudness
of the thin light eardrum and the high impedance estimates (frequencies where sounds seemed
of the closed fluid-filled capsule, that is the inner disproportionately louder). These observations
ear, operates equally well in both directions. It reminded Kemp of a prediction made by the British
matches cochlea to eardrum just as well as eardrum astrophysicist Thomas Gold. Upon observing the
to cochlea. expansive dynamic range of hearing, Gold had
postulated that the ear must contain a nonlinear
How does the cochlea vibrate the eardrum to amplifier – an amplifier that provided gain for low
create sound, i.e., an OAE? Simply put, moving the inputs to make them audible but became passive
eardrum from within the sealed fluid-filled cochlea to make high inputs tolerable. This is known today
requires an imbalance of vibrational fluid pressure as the cochlea amplifier; Kemp connected his
on the oval and round windows. This requires the observation of the peaks and valleys in behavioural
diversion of vibrational energy away from the data and Gold’s predictions and hypothesised
primary hearing process and the transmission of that the valleys in hearing sensitivity and peaks
that energy back to the base of the cochlea in a way in loudness estimates could be due to these
that can physically create this pressure difference sounds produced by the ear. That is, the presence
and cause middle ear motion. The initial source of an internal sound source at a given frequency
of vibrational energy needed to generate OAEs is would add to any external tone played leading to
generally considered to be the electromotility of hypersensitivity in threshold measures as well as
the three outer rows of the cochlea’s sensory hair a heightened perception of loudness. With this
cells, the outer hair cells (OHCs)1,2. Motility of OHCs notion, he salvaged a miniature microphone from a
as they respond to auditory stimulation provides hearing aid and sealed it with silicone putty to keep
the engine of the “cochlear amplifier.” A reverse the sound in over his ear, and attached the output
travelling wave along the basilar membrane would to an analyser to see if sounds could be picked up.
Proceedings of Singapore Healthcare Volume 24 Number 2 2015 87Review
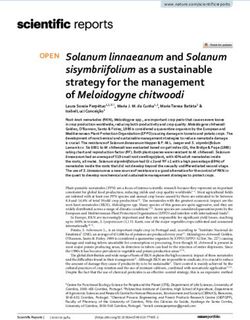
Temporal bone
Pinna
Malleus
Waveform 1 Attenuator
Semicircular
Waveform 2 Attenuator canals
Sound source 1 Cochlear
nerve (VIII)
Sound source 2
Microphone
Cochlea
Analyser Amplifier Incus
External Stapes in Eustachian tube
auditory oval
Earpiece sealed canal window
into ear canal
Cochlear emission
Fig. 1. Oto-acoustic emission system.
Indeed they did and today we know them as oto- from patients who are comatose. The recording
acoustic emissions (OAEs) and use them routinely time for OAEs is quick. Quiet and cooperative
for a multitude of clinical purposes. patients usually require less than a few minutes
per ear to get an accurate reading but for
METHOD uncooperative or noisy patients, recordings may
Oto-acoustic emissions are measured by presenting take significantly longer or may be impossible to
a series of sounds or “clicks” to the ear through a obtain on a given visit. Each individual has his/
probe that is snugly inserted into the ear canal her own characteristic repeatable OAEs and hence
probe (Fig. 1). It contains: repeatability or reproducibility of OAEs can help to
verify the response.
1. A loudspeaker that generates the sounds
Although testing does not require patient
2. A sensitive microphone that measures the cooperation, a seal probe, which helps to block
resulting OAEs that are produced in the out external noise, ear canal patency with an
cochlea and are transmitted through the unobstructed outer ear canal and absence of
middle ear into the outer ear canal significant middle ear pathology and background
room noise should be below 40dB due to the
3. A signal separating processor that can sensitivity of OAEs to noise. All OAEs are analysed
discriminate the sound of the OAE from the relative to the noise floor; therefore, reduction of
stimulus sound and other noise. physiologic and acoustic ambient noise is critical
for good recordings. Depending on the intended
A probe with a soft flexible tip is inserted in the ear portion of the cochlea that is of concern (frequency
canal to obtain a seal. Different probes are used specific response), the acoustic stimulus can be
for neonates and adults and are calibrated varied from no stimulus, to click stimuli (wide-band
differently because of the significant difference in noise), or tones (narrow band noise).
ear canal volume.
Oto-acoustic emissions are the only audiological
Oto-acoustic emissions are appropriate for use in test to selectively assess cochlear dysfunction.
difficult to test patients: newborn infants, young Along with tympanometry and auditory
uncooperative children and individuals with brain stem responses, OAEs can aid in the
developmental delays. Because no behavioural differentiation between middle-ear, cochlear, and
response is required, OAEs can be obtained even neural disorders.
88 Proceedings of Singapore Healthcare Volume 24 Number 2 2015Revisiting OAEs
Table 1. Types of OAEs.
Sounds emitted without an acoustic stimulus (i.e., spontaneously)
Spontaneous OAEs in humans usually consist of a stable tone with a bandwidth (frequency stability)
within the 1-2 kHz region; amplitudes are between -5 and 14 dB SPL. They are generally not found
Spontaneous OAEs (SOAEs)
in individuals with hearing thresholds worse than 30 dB HL. Therefore, the presence of SOAEs are
usually considered a sign of cochlear health, but the absence of SOAEs are not necessarily a sign of
abnormality.
Occur during or after a stimulus and can be further classified into:
Transient evoked OAEs (TEOAEs) Sounds emitted in response to an acoustic stimulus of very
short duration; usually clicks but can be tone-bursts.
Produces complex frequency-dispersed oscillation consisting
mainly of the frequencies present in the stimulus. Because OAEs
are evoked by transient signals that have a wide frequency
response, a broad region of the cochlea responds, providing
information on the frequency range from 1 to 4 kHz, and only if
hearing thresholds are 20 dB HL or better.
Stimulus frequency OAEs (SFOAEs) Stimulus frequency OAEs are responses recorded by stimulation
Evoked OAEs (EOAEs) of a continuous pure tone. Because the stimulus and the
emission overlap in the ear canal, the recording microphone
detects both. Therefore, interpretation depends on reading
complicated series of ripples in the recording. At present,
SFOAEs are not used clinically.
Distortion product OAEs (DPOAEs) Occur as a response to two simultaneous pure tones (typically
55 & 65 dB SPL) at two different frequencies.
It allows greater frequency specificity and can be used to record
at higher frequencies than TOAEs.
The use of different frequency combinations allows a larger
portion of the basilar membrane to be stimulated and its
response analysed (between 1–8 kHz frequency range).
TYPES OF OAEs that patient can still be monitored (so long as
Oto-acoustic emissions can be broadly classified their hearing loss is not too great) for possible
into two groups (Table 1). Two main types of evoked progression. Lastly, using DPOAEs can provide
OAE are used in clinical practice: TEOAEs & DPOAEs. some indication of degree and configuration
Both are complementary, as the former is best of the hearing loss given its ability to estimate
detecting threshold elevation below 4kHz, giving (albeit not accurately) thresholds as well as its
an overview of cochlear activity; the latter above spectrum of frequency detection.
it, giving specific quantitative information about
sound processing at distinct cochlear places. In CLINICAL APPLICATIONS
short, the TEOAE response “sees” almost the whole There are four main OAE applications in clinical
cochlea, whereas the DPOAE response reflects only diagnostics: newborn hearing screening,
a limited region of the cochlea but gives some Topological diagnostics, quantitative evaluation
indication of the extent of loss. of hearing loss and recruitment, and monitoring
cochlear function.
The advantages of DPOAE as compared to TEOAE
are summarised as below: Newborn Hearing Screening
Otoacoustic emissions (TEOAE and DPOAE) are
• First, DPOAEs are able to test higher frequencies widely regarded as being suitable for screening in
than TEOAEs, making them more sensitive newborns and infants3–5, since they are not present
to the high frequencies affected first in in the case of OHC dysfunction6,7. The premise
certain conditions e.g. ototoxicity and noise for this approach is that inner-ear hearing loss
induced damage. always includes OHC damage or malfunction. Its
use is widely incorporated into universal newborn
• Secondly, DPOAEs can be recorded in the hearing screening programs and in pediatric clinics
presence of mild to moderate hearing loss as where the patients are too young to be cooperative
compared to TEOAEs, which give a more binary in conventional hearing tests8. The OAE technology
response. Therefore, if hearing loss already exists, can have a sensitivity of 95% and specificity of 90%9
Proceedings of Singapore Healthcare Volume 24 Number 2 2015 89Review
whilst the referral rate is 5–20% when screening is evaluation before the age of 3 months. With
performed within the first 24 hours of life10. successful implementation of an extensive UNHS
coupled with early and effective intervention,
This is usually combined with ABR methods for this maximises the chances of affected children to
screening protocols due to the disadvantage of better integrate into mainstream society.
OAEs giving false positive results ranging from 11
to 35%7,11 in paediatric patients with significant Topological Diagnostics
conductive losses12; more often than not due to The management for a hearing disorder can be
Eustachian tube dysfunction or residual amniotic developed only after knowing which stage of the
fluid in the tympanic cavity which attenuates auditory pathway is impaired. Psychoacoustic
the OAE signal. To avoid high referral rates, some tests are able to differentiate between conductive,
hearing screening protocols add on ABR screening sensorineural or mixed hearing loss by evaluating
before referral for diagnostic assessment13. the difference between air and bone-conductive
pure-tone thresholds. However, the differentiation
It is widely accepted that children with untreated between a sensory (cochlear) and a neural disorder
loss generally perform poorly academically as with subjective testing is unreliable. In addition, in
compared to their peers. Hearing loss affects uncooperative patients or infants, psychoacoustic
both reading and writing skills, resulting in tests cannot be performed. In such cases, only
poor communication and language skills. The objective tests help in achieving the goal of
literature supports the trend that the longer the determining end-organ integrity.
delay in intervention, the poorer the academic
outcomes tended to be14. In Yoshinaga-Itano’s The use of OAEs to assist in the diagnosis of retro-
10-year longitudinal study15 on the effect of early cochlear pathologies have become standard in
identification on the development of deaf and clinical practice. OAEs arise from the peripheral
hard-of-hearing infants and toddlers, the language auditory system; therefore, a logical conclusion is
abilities of hearing-impaired children identified that they will be present in cases of retro-cochlear
before 6 months were pitted against those pathology. One of the most common applications
identified after 6 months. The results were not would be in the diagnosis of auditory neuropathy;
surprising, whereby those detected early before 6 In such a condition, the patient displays auditory
months had a significantly better average language characteristics consistent with normal OHC and
quotient as compared to those after 6 months, abnormal neural function at the level of the VIIIth
across all degrees of hearing loss. In addition, if nerve; where these characteristics are observed
such a disability is untreated, it can also lead to on clinical audiologic tests as normal oto-acoustic
emotional and psychosocial handicaps16. Delayed emissions (OAEs) in an absent or severely abnormal
identification and management can impede a auditory brainstem response (ABR), result in
child’s ability to adapt to the hearing world, and poor word recognition and variable audiogram
if remedied early facilitates full advantage of the findings18,19. These patients are distinguished
plasticity of the developing sensory systems, so as from patients with space-occupying lesions, such
to allow normal social development and improved as VIIIth nerve tumours, or multiple sclerosis, in
future prospects. that radiological evaluation yields normal results
and even the most peripheral responses from the
In Singapore, the Universal National Hearing VIIIth nerve are absent. The role of OAEs is evident
Screening programme was set up in 2002, and in ruling out OHC dysfunction, and together
first implemented in KK Women’s and Children’s with a normal tympanometry points to a retro-
Hospital (KKWCH) which accounts for a third cochlear lesion.
of deliveries; and subsequently adopted by all
public and private hospitals in the country which A combination of present OAEs with altered
boasts obstetrics services. The programme17 aims ABRs must also bring into mind other differential
to screen all neonates before they are discharged diagnosis. These cases belong to clinical profiles
from the hospital. Newborns who failed the involving vestibular schwanommas and other
screening had a repeat screening within 4 to 6 central auditory system disorders. In the setting of a
weeks; failing both screening tests would result tumour in the internal auditory canal, interestingly
in referral for audiological diagnosis and medical OAEs (TEOAES or DPOAEs) can be affected or
90 Proceedings of Singapore Healthcare Volume 24 Number 2 2015Revisiting OAEs
unaffected by the presence of space occupying frequencies first, with hearing loss systematically
lesion such as a vestibular schwanomma. An progressing to the lower frequencies26,27.
explanation for such data can be derived from
information of how the growth of the tumor affects The biggest limitation to OAEs is that they are
the vascular supply of the cochlea; especially if it very sensitive to middle ear dysfunction, which is
impinges on the internal auditory artery or how common in children and in those who are immuno-
the growth of the tumors induces mechanical compromised. Although OAEs are being employed
pressure alterations on the vascular supply and the for ototoxicity monitoring, they are rarely used in
cochlea itself20. OAE-based measures can provide isolation. A change in OAEs from one test session to
information on the sensory component of any the next is a strong indicator for the need for more
hearing disorder, thus they can provide precise conventional and HFA testing. This allows cost
indices of evaluating sensori-neural hearing effective testing whereby further testing is avoided
impairment cases. In addition, in patients with unless OAEs suggest otherwise. Early detection
suspected labrynthine schwanommas, the OAE of ototoxicity is an important signal for alternate
can be of some assistance in the differentiation management options such as substitution of
of cochlea and vestibular types of schwannomas medications, change of dosages, and mode
serving as an adjunct to imaging investigations21. of administration.
Quantitative Evaluation of Hearing Response Much like the use of OAEs in ototoxicity
and Recruitment monitoring, OAEs can be used to provide objective
The concept behind this lies in the ability of OAEs confirmation of cochlea dysfunction in patients
to identify regions of the cochlea with damage, with normal audiograms. In noise induced hearing
which can assist in programming a hearing aid. loss, threshold elevations are proven to be in the
Simply explained, when OAEs are absent, we mid to high frequencies28; OAE protocols can thus
assume hearing loss of greater than about 25 dB HL be used very efficiently to monitor small elevations
at the frequency where the emission is absent and in threshold progress29. Oto-acoustic emissions
this gives us some idea of hearing levels. Bear in can provide an early and reliable warning sign of
mind however, amplification protocols for different cochlea dysfunction due to noise/music exposure
patient groups are much more complex, usually before any problem is evident on the audiogram30.
requiring a battery of tools such as ABR before we Some studies even go as far as to say that OAEs
can use this data to program amplification for these can be a diagnostic predictor for noise-induced-
patients. Oto-acoustic emissions are one of the hearing-loss-risk31.
many tools that help influence the programming.
Intra-operatively, its use can be seen in its live
Monitoring Cochlea Function monitoring of changes in cochlea status over
Oto-acoustic-emission measures are stable time during surgery, where morbidity is high
through time in any particular individual and and utmost care is taken to minimise damage
hence are capable of monitoring recovery from to cochlea nerve function32. For example in the
OHC impairment22,23. Three main approaches have context of vestibular schwanomma surgery, OAEs
been used for monitoring the effects of ototoxic are taken during pre- as well as intraoperative
medications: basic audiologic assessment, high monitoring to prognosticate post-operative
frequency audiometry (HFA; 10–18 kHz), and cochlea function33,34.
OAEs24. Ototoxic drugs exert their effect on OHC
function (although not solely on OHCs), and Future Applications
OAEs are OHC dependent. With ototoxicity, OAEs Our persistent uncertainties about OAEs are a
have been shown to decrease simultaneously testament to their complex nature. Not only are we
with changes in HFA thresholds and before still debating about their generation mechanisms,
changes appear in the conventional audiometric different ideas about how they transmit out of
frequencies24. Part of this group are therapeutic the cochlea still exist. One thing is clear, the uses
drugs such as antibiotic (e.g., aminoglycosides) of OAE measurements as diagnostic tools have
and antitumor chemotherapeutic (e.g., cisplatin) obvious advantages (especially in their objectivity
agents25, are reported to induce an irreversible and restriction to the cochlea) that they have been
hearing loss, which typically affects the highest rapidly incorporated as clinical tools.
Proceedings of Singapore Healthcare Volume 24 Number 2 2015 91Review
Arch Otorhinolaryngol 1979;224(1–2):37–45 doi:
The holy grail is to be able to use OAEs to 10.1007/BF00455222.
definitively determine hearing thresholds; 3. American Academy of Pediatrics, Joint Committee
on Infant Hearing. Year 2007 position statement:
currently it cannot be used in isolation for such a Principles and guidelines for early hearing detection and
purpose. In many cases, it is probably better off intervention programs. Pediatrics 2007;120(4):898–921
to stick with behavioural threshold estimation, doi: 10.1542/peds.2007-2333.
4. Berninger E, Westling B. Outcome of a universal newborn
but one can certainly see the benefit of having an
hearing-screening programme based on multiple
objective non-invasive tool for gathering threshold transient-evoked otoacoustic emissions and clinical
information in certain populations and situations. brainstem response audiometry. Acta Otolaryngol
2011;131(7):728–39 doi: 10.3109/00016489.2011.554440.
So far, attempts to predict hearing thresholds from
5. Akinpelu OV, Peleva E, Funnell WR, Daniel SJ. Otoacoustic
DPOAE and TEOAE levels measured in response emissions in newborn hearing screening: A systematic
to fixed-level stimuli varied in frequency were not review of the effects of different protocols on test
conclusive35,36. However, there have been efforts at outcomes. Int J Pediatr Otorhinolaryngol 2014;78(5):711–
7 doi: 10.1016/j.ijporl.2014.01.021.
predicting hearing thresholds using DPOAE input/ 6. Kemp DT, Ryan S. Otoacoustic emission tests in
output functions37 which may open the door to neonatal screening programmes. Acta Otolaryngol
such an avenue in future. 1991;111(s482):73–84 doi: 10.3109/00016489109128029.
7. Norton SJ, Gorga MP, Widen JE, Folsom RC, Sininger Y,
Cone-Wesson B, et al. Identification of neonatal hearing
Age related hearing loss is one of the most impairment: Evaluation of transient evoked otoacoustic
ubiquitous pathology that is commonly seen emission, distortion product otoacoustic emission, and
auditory brain stem response test performance. Ear Hear
in clinics. It is well known that signs of aging are 2000;21(5):508–28 doi: 10.1097/00003446-200010000-
evident at higher frequencies. However, new 00013.
findings have demonstrated that signs of aging 8. Berg AL, Prieve BA, Serpanos YC, Wheaton MA. Hearing
screening in a well-infant nursery: Profile of automated
are visible in DPOAE levels at frequencies as low as abr-fail/oae-pass. Pediatrics 2011;127(2):269–75 doi:
1000 Hz for individuals as young as 20 years old38. 10.1542/peds.2010-0676.
This forces us to change our perception about 9. Taylor CL, Brooks RP. Screening for hearing loss and
middle-ear disorders in children using teoaes. Am J Audiol
auditory aging and when might be the right time 2000;9(1):50–5 doi: 10.1044/1059-0889(2000/001).
to start awareness campaigns to protect our ears. 10. Erenberg A, Lemons J, Sia C, Trunkel D, Ziring P. Newborn
and infant hearing loss: Detection and intervention.
American academy of pediatrics. Task force on
With innovative applications of OAEs emerging
newborn and infant hearing, 1998–1999. Pediatrics
everyday, there is no lack of controversy over its 1999;103(2):527–30 doi: 10.1542/peds.103.2.527.
reliability in uses such as for tinnitus monitoring, 11. Barker SE, Lesperance MM, Kileny PR. Outcome of
newborn hearing screening by ABR compared with four
Meniere’s disease and even acoustic fingerprinting.
different DPOAE pass criteria. Am J Audiol 2000;9(2):142–
Further research has to be put into its validation for 8 doi: 10.1044/1059-0889(2000/017).
such purposes. No doubt, OAEs have been able to 12. Doyle KJ, Rodgers P, Fujikawa S, Newman E. External
effectively segregate good and bad ears over the and middle ear effects on infant hearing screening test
results. Otolaryngol Head Neck Surg 2000;122(4):477–81
past decade, with newborn hearing screening as doi: 10.1067/mhn.2000.102573.
the main driving force. The techniques for making 13. Arslan S, Isik AU, Imamoglu M, Topbas M, Aslan Y, Ural
such decisions are still being refined today39. A. Universal newborn hearing screening; automated
transient evoked otoacoustic emissions. B-ENT
2012;9(2):122–31.
Its main strength is in its non-invasive, frequency 14. Yoshinaga-Itano C, Apuzzo ML. The development of deaf
specific, objective measurement of cochlea and hard of hearing children identified early through the
high-risk registry. Am Ann Deaf 1998;143(5):416–24 doi:
audiological function, which charges it with 10.1353/aad.2012.0118.
invaluable roles. It is safe to say that OAEs will 15. Yoshinaga-Itano C, Sedey AL, Coulter DK, Mehl AL.
continue to play an important role in routine Language of early- and later-identified children with
hearing loss. Pediatrics 1998;102(5):1161–71.
audiological assessments as well as its less known 16. Filipo R, Bosco E, Barchetta C, Mancini P. Cochlear
uses. Its promise in further developments can only implantation in deaf children and adolescents: Effects on
open up exciting possibilities in the years to come. family schooling and personal well-being. Int J Pediatr
Otorhinolaryngol 1999;49(1 Suppl):S183–7 doi: 10.1016/
S0165-5876(99)00212-8.
REFERENCES 17. Low WK, Pang KY, Ho LY, Lim SB, Joseph R. Universal
1. Kemp DT. Stimulated acoustic emissions from newborn hearing screening in Singapore: The need,
within the human auditory system. J Acoust Soc Am implementation and challenges. Ann Acad Med
1978;64(5):1386–91 doi: 10.1121/1.382104. Singapore 2005;34(4):301–6.
2. Kemp DT. Evidence of mechanical nonlinearity and 18. Narne VK, Prabhu PP, Chatni S. Time-frequency analysis
frequency selective wave amplification in the cochlea. of transient evoked-otoacoustic emissions in individuals
92 Proceedings of Singapore Healthcare Volume 24 Number 2 2015Revisiting OAEs
with auditory neuropathy spectrum disorder. Hear Res 30. Baradarnfar MH, Karamifar K, Mehrparvar AH,
2014;313:1–8 doi: 10.1016/j.heares.2014.04.005. Mollasadeghi A, Gharavi M, Karimi G, et al. Amplitude
19. Norrix LW, Velenovsky DS. Auditory neuropathy spectrum changes in otoacoustic emissions after exposure to
disorder (ANSD): A review. J Speech Lang Hear Res industrial noise. Noise Health 2012;14(56):28–31 doi:
2014;57(4):1564–76 doi: 10.1044/2014_JSLHR-H-13-0213. 10.4103/1463-1741.93329.
20. Telischi FF, Roth J, Stagner BB, Lonsbury-Martin BL, Balkany 31. Lapsley Miller JA, Marshall L, Heller LM, Hughes LM. Low-
TJ. Patterns of evoked otoacoustic emissions associated level otoacoustic emissions may predict susceptibility
with acoustic neuromas. Laryngoscope 1995;105(7 Pt to noise-induced hearing loss. J Acoust Soc Am
1):675–82 doi: 10.1288/00005537-199507000-00002. 2006;120(1):280–96 doi: 10.1121/1.2204437.
21. Kagoya R, Shinogami M, Kohno M, Yamasoba T. 32. Cueva RA. Preoperative, intraoperative, and postoperative
Distortion-product otoacoustic emission tests evaluate auditory evaluation of patients with acoustic neuroma.
cochlear function and differentiate cochlear and Otolaryngol Clin North Am 2012;45(2):285–90 doi:
vestibular schwannoma. Otolaryngol Head Neck Surg 10.1016/j.otc.2011.12.002.
2013;148(2):267–71 doi: 10.1177/0194599812469502. 33. Morawski K, Namyslowski G, Lisowska G, Bazowski P,
22. McMillan GP, Reavis KM, Konrad-Martin D, Dille MF. The Kwiek S, Telischi FF. Intraoperative monitoring of cochlear
statistical basis for serial monitoring in audiology. Ear Hear function using distortion product otoacoustic emissions
2013;34(5):610–8 doi: 10.1097/AUD.0b013e31828a21b3. (dpoaes) in patients with cerebellopontine angle tumors.
23. Reavis KM, Phillips DS, Fausti SA, Gordon JS, Helt WJ, Otol Neurotol 2004;25(5):818–25 doi: 10.1097/00129492-
Wilmington D, et al. Factors affecting sensitivity of 200409000-00028.
distortion-product otoacoustic emissions to ototoxic 34. Kim AH, Edwards BM, Telian SA, Kileny PR, Arts HA.
hearing loss. Ear Hear 2008;29(6):875–93 doi: 10.1097/ Transient evoked otoacoustic emissions pattern as a
AUD.0b013e318181ad99. prognostic indicator for hearing preservation in acoustic
24. American academy of audiology clinical practice neuroma surgery. Otol Neurotol 2006;27(3):372–9 doi:
guidelines on ototoxicity monitoring oct 2009; 10.1097/00129492-200604000-00014.
25. Reavis KM, McMillan G, Austin D, Gallun F, Fausti SA, 35. Mertes IB, Goodman SS. Short-latency transient-evoked
Gordon JS, et al. Distortion-product otoacoustic emission otoacoustic emissions as predictors of hearing status and
test performance for ototoxicity monitoring. Ear Hear thresholds. J Acoust Soc Am 2013;134(3):2127–35 doi:
2011;32(1):61–74 doi: 10.1097/AUD.0b013e3181e8b6a7. 10.1121/1.4817831.
26. Kopelman J, Budnick AS, Sessions RB, Kramer MB, 36. Shaffer LA, Dhar S. DPOAE component estimates and
Wong GY. Ototoxicity of high-dose cisplatin by bolus their relationship to hearing thresholds. J Am Acad
administration in patients with advanced cancers and Audiol 2006;17(4):279–92 doi: 10.3766/jaaa.17.4.6.
normal hearing. Laryngoscope 1988;98(8 Pt 1):858–64 37. Neely ST, Johnson TA, Kopun J, Dierking DM, Gorga MP.
doi: 10.1288/00005537-198808000-00014. Distortion-product otoacoustic emission input/output
27. Stavroulaki P, Apostolopoulos N, Segas J, Tsakanikos characteristics in normal-hearing and hearing-impaired
M, Adamopoulos G. Evoked otoacoustic emissions--an human ears. J Acoust Soc Am 2009;126(2):728–38 doi:
approach for monitoring cisplatin induced ototoxicity in 10.1121/1.3158859.
children. Int J Pediatr Otorhinolaryngol 2001;59(1):47–57 38. Poling GL, Siegel JH, Lee J, Lee J, Dhar S. Characteristics
doi: 10.1016/S0165-5876(01)00455-4. of the 2f1-f2 distortion product otoacoustic emission
28. Attias J, Horovitz G, El-Hatib N, Nageris B. Detection in a normal hearing population. J Acoust Soc Am
and clinical diagnosis of noise-induced hearing loss by 2014;135(1):287–99 doi: 10.1121/1.4845415.
otoacoustic emissions. Noise Health 2001;3(12):19–31. 39. Reuven ML, Neely ST, Kopun JG, Rasetshwane DM, Allen
29. Sisto R, Chelotti S, Moriconi L, Pellegrini S, Citroni A, JB, Tan H, et al. Effect of calibration method on distortion-
Monechi V, et al. Otoacoustic emission sensitivity to low product otoacoustic emission measurements at and
levels of noise-induced hearing loss. J Acoust Soc Am around 4 kHz. Ear Hear 2013;34(6):779–88 doi: 10.1097/
2007;122(1):387–401 doi: 10.1121/1.2737668. AUD.0b013e3182994f15.
Proceedings of Singapore Healthcare Volume 24 Number 2 2015 93You can also read